The Association of Domestic Incense Burning with Hypertension and Blood Pressure in Guangdong, China


 ,
,
Abstract
:1. Introduction
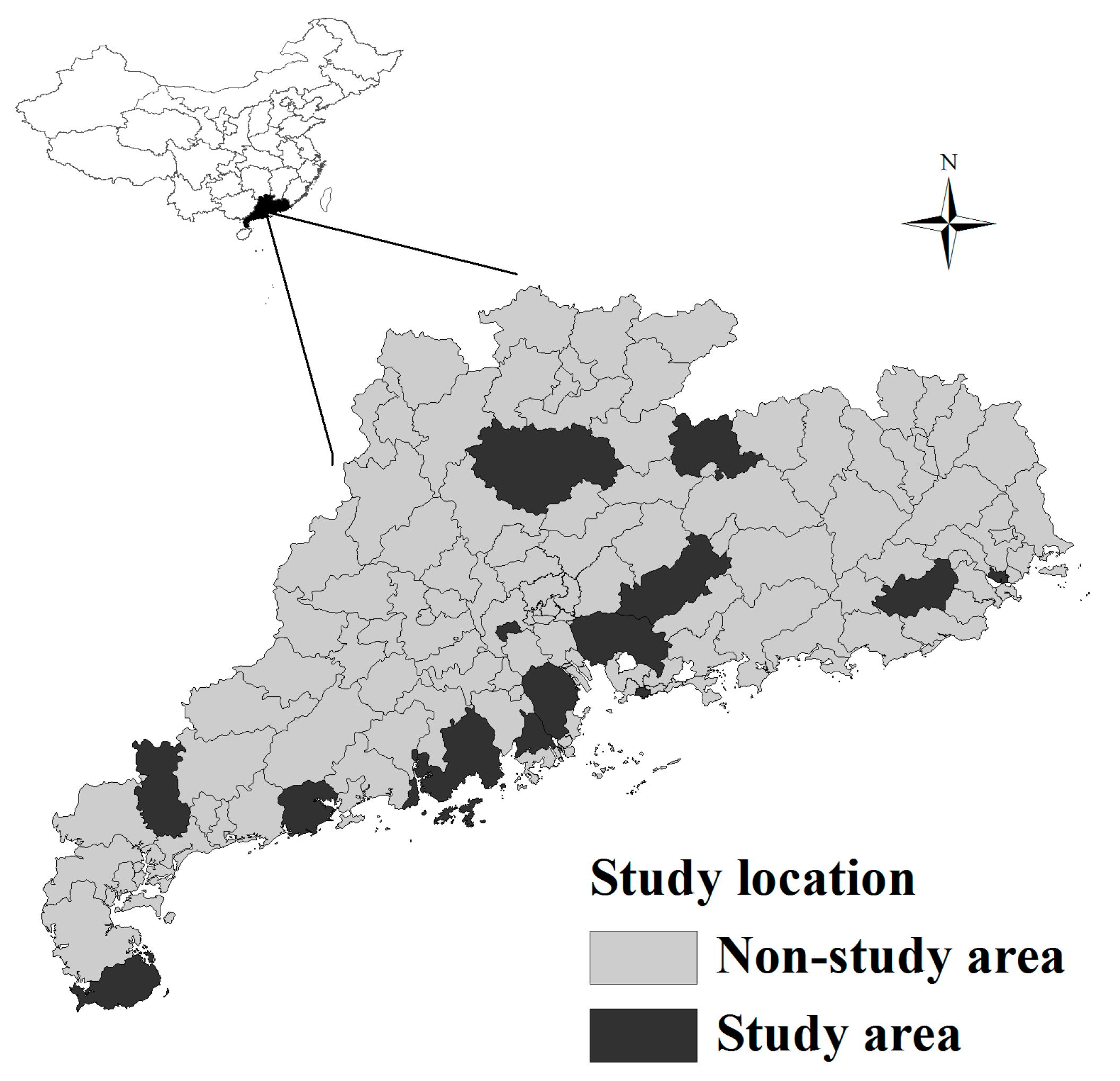
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Lawes, C.M.; Vander Hoorn, S.; Rodgers, A. Global burden of blood-pressure-related disease, 2001. Lancet 2008, 371, 1513–1518. [Google Scholar] [CrossRef]
- Perkovic, V.; Huxley, R.; Wu, Y.; Prabhakaran, D.; MacMahon, S. The burden of blood pressure-related disease: A neglected priority for global health. Hypertension 2007, 50, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Xu, Z.; Xu, X.; Cai, Q.; Xu, Y. Prevalence, awareness, treatment, and control of hypertension among residents in Guangdong Province, China, 2004 to 2007. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Dong, G.H.; Qian, Z.M.; Xaverius, P.K.; Trevathan, E.; Maalouf, S.; Parker, J.; Yang, L.; Liu, M.M.; Wang, D.; Ren, W.H. Association between long-term air pollution and increased blood pressure and hypertension in China. Hypertension 2013, 61, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, J.; Schauer, J.J.; Ezzati, M.; Lu, L.; Cheng, C.; Patz, J.A.; Bautista, L.E. Indoor air pollution and blood pressure in adult women living in rural China. Environ. Health Perspect. 2011, 119, 1390. [Google Scholar] [CrossRef] [PubMed]
- Van den Hooven, E.H.; de Kluizenaar, Y.; Pierik, F.H.; Hofman, A.; van Ratingen, S.W.; Zandveld, P.Y.; Mackenbach, J.P.; Steegers, E.A.; Miedema, H.M.; Jaddoe, V.W. Air pollution, blood pressure, and the risk of hypertensive complications during pregnancy the generation R study. Hypertension 2011, 57, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.L.; Bazemore, H.; Reynolds, S.J.; Heiderscheidt, J.M.; Conway, S.; Bachand, A.M.; Volckens, J.; Peel, J.L. A baseline evaluation of traditional cook stove smoke exposures and indicators of cardiovascular and respiratory health among Nicaraguan women. Int. J. Occup. Environ. Health 2011, 17, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.H.; Van Hee, V.C.; Bergen, S.; Szpiro, A.A.; DeRoo, L.A.; London, S.J.; Marshall, J.D.; Kaufman, J.D.; Sandler, D.P. Long-term air pollution exposure and blood pressure in the sister study. Environ. Health Perspect. 2015, 123, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Mukherjee, B.; Das, D.; Banerjee, A.; Ray, M. Hypertension with elevated levels of oxidized low-density lipoprotein and anticardiolipin antibody in the circulation of premenopausal Indian women chronically exposed to biomass smoke during cooking. Indoor Air 2011, 21, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Bonjour, S.; Adair Rohani, H.; Wolf, J.; Bruce, N.G.; Mehta, S.; PrüssUstün, A.; Lahiff, M.; Rehfuess, E.A.; Mishra, V.; Smith, K.R. Solid fuel use for household cooking: Country and regional estimates for 1980–2010. Headache 2008, 48, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.M.; Chen, S.C.; Chen, J.W.; Liang, H.M. Contributions of Chinese-style cooking and incense burning to personal exposure and residential PM concentrations in Taiwan region. Sci. Total. Environ. 2006, 358, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Wang, B. Characteristics of emissions of air pollutants from burning of incense in a large environmental chamber. Atmos. Environ. 2004, 38, 941–951. [Google Scholar] [CrossRef]
- Lin, T.C.; Krishnaswamy, G.; Chi, D.S. Incense smoke: Clinical, structural and molecular effects on airway. Clin. Mol. Allergy 2008, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Dalibalta, S.; Elsayed, Y.; Alqtaishat, F.; Gomes, I.; Fernandes, N. A health risk assessment of Arabian incense (Bakhour) smoke in the United Arab Emirates. Sci. Total. Environ. 2015, 511, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, Y.; Dalibalta, S.; Gomes, I.; Fernandes, N.; Alqtaishat, F. Chemical composition and potential health risks of raw Arabian incense (Bakhour). J. Saudi Chem. Soc. 2014, 20, 465–473. [Google Scholar] [CrossRef]
- Chen, C.C.; Lee, H. Genotoxicity and DNA adduct formation of incense smoke condensates: Comparison with environmental tobacco smoke condensates. Mutat. Res. Genet. Toxicol. 1996, 367, 105–114. [Google Scholar] [CrossRef]
- Friborg, J.; Yuan, J.M.; Wang, R.; Koh, W.P.; Lee, H.P.; Yu, M. Incense use and respiratory tract carcinomas: A prospective cohort study. Cancer Res. 2007, 67, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.H.; Yu, I.T.S.; Tse, L.A.; Au, J.S.K.; Wang, F.; Lau, J.S.M.; Zhang, B. Domestic incense burning and nasopharyngeal carcinoma: A case-control study in Hong Kong Chinese. Environ. Mol. Mutagen. 2014, 55, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Clark, M.L.; Ang, L.W.; Yu, M.C.; Yuan, J.M.; Koh, W.P. Incense use and cardiovascular mortality among Chinese in Singapore: The Singapore Chinese Health Study. Environ. Health Perspect. 2014, 122, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Lyu, S.R.; Su, J.; Xiang, Q.Y.; Wu, M. Suggestion on improvement of surveillance technique for chronic disease and related risk factors in China. Dis. Surveill. 2014, 29, 247–249. [Google Scholar]
- Lao, X.Q.; Ma, W.; Chung, R.Y.N.; Zhang, Y.; Xu, Y.; Xu, X.; Nie, S.; Cai, Q.; Xia, L.; Su, X. The diminishing socioeconomic disparity in obesity in a Chinese population with rapid economic development: Analysis of serial cross-sectional health survey data 2002–2010. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for the Management of Hypertension; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Ge, K.; Jia, J.; Liu, H. Food-based dietary guidelines in China—Practices and problems. Ann. Nutr. Metab. 2007, 51, 26–31. [Google Scholar] [CrossRef]
- Lewington, S.; Li, L.; Sherliker, P.; Guo, Y.; Millwood, I.; Zheng, B.; Whitlock, G.; Ling, Y.; Collins, R.; Junshi, C. Seasonal variation in blood pressure and its relationship with outdoor temperature in 10 diverse regions of China: The China Kadoorie Biobank. J. Hypertens. 2012, 30, 1383. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.; Lochner, K.A.; Kawachi, I. Neighborhood differences in social capital: A compositional artifact or a contextual construct? Health Place 2003, 9, 33–44. [Google Scholar] [CrossRef]
- Grotto, I.; Huerta, M.; Sharabi, Y. Hypertension and socioeconomic status. Curr. Opin. Cardiol. 2008, 23, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Ritz, B.; Wilhelm, M.; Hoggatt, K.J.; Ghosh, J.K.C. Ambient air pollution and preterm birth in the environment and pregnancy outcomes study at the University of California, Los Angeles. Am. J. Epidemiol. 2007, 166, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Guo, Y.; Zheng, Y.; Zhao, X.; Cao, Z.; Rigdon, S.E.; Xian, H.; Li, X.; Liu, T.; Xiao, J.; et al. Exposure to ambient PM2.5 associated with overall and domain-specific disability among adults in six low- and middle-income countries. Environ. Int. 2017, 104, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Lin, H.; Liang, Y.; Zhang, T.; Luo, C.; Jiang, Z.; Xu, Q.; Xue, F.; Liu, Y.; Li, X. The short-term association between meteorological factors and mumps in Jining, China. Sci. Total. Environ. 2016, 568, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Barregard, L.; Sällsten, G.; Gustafson, P.; Andersson, L.; Johansson, L.; Basu, S.; Stigendal, L. Experimental exposure to wood-smoke particles in healthy humans: Effects on markers of inflammation, coagulation, and lipid peroxidation. Inhal. Toxicol. 2006, 18, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Dwyer-Lindgren, L.; Lofgren, K.T.; Rajaratnam, J.K.; Marcus, J.R.; Levin-Rector, A.; Levitz, C.E.; Lopez, A.D.; Murray, C.J. Age-specific and sex-specific mortality in 187 countries, 1970–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013, 380, 2071–2094. [Google Scholar] [CrossRef]
- Al Attas, O.S.; Hussain, T.; Ahmed, M.; Al daghri, N.; Mohammed, A.A.; De Rosas, E.; Gambhir, D.; Sumague, T.S. Ultrastructural changes, increased oxidative stress, inflammation, and altered cardiac hypertrophic gene expressions in heart tissues of rats exposed to incense smoke. Environ. Sci. Pollut. Res. 2015, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Young, B.; Dockery, D. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef] [PubMed]
- Bautista, L.; Vera, L.; Arenas, I.; Gamarra, G. Independent association between inflammatory markers (C-reactive protein, interleukin-6, and TNF-α) and essential hypertension. J. Hum. Hypertens. 2005, 19, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Urch, B.; Dvonch, J.T.; Bard, R.L.; Speck, M.; Keeler, G.; Morishita, M.; Marsik, F.J.; Kamal, A.S.; Kaciroti, N. Insights into the mechanisms and mediators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension 2009, 54, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D. You are what you breathe: Evidence linking air pollution and blood pressure. Curr. Hypertens. Rep. 2005, 7, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Langrish, J.P.; Mills, N.L.; Chan, J.; Leseman, D.; Aitken, R.J.; Fokkens, P.; Cassee, F.R.; Li, J.; Donaldson, K.; Newby, D.E. Beneficial cardiovascular effects of reducing exposure to particulate air pollution with a simple facemask. Part Fibre Toxicol. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Urch, B.; Silverman, F.; Corey, P.; Brook, J.R.; Lukic, K.Z.; Rajagopalan, S.; Brook, R.D. Acute blood pressure responses in healthy adults during controlled air pollution exposures. Environ. Health Perspect. 2005, 113, 1052. [Google Scholar] [CrossRef] [PubMed]
- Weber, L.P.; Al Dissi, A.; Marit, J.S.; German, T.N.; Terletski, S.D. Role of carbon monoxide in impaired endothelial function mediated by acute second-hand tobacco, incense, and candle smoke exposures. Environ. Toxicol. Pharmacol. 2011, 31, 453–459. [Google Scholar] [CrossRef] [PubMed]
- McCracken, J.P.; Smith, K.R.; Díaz, A.; Mittleman, M.A.; Schwartz, J. Chimney stove intervention to reduce long-term wood smoke exposure lowers blood pressure among Guatemalan women. Environ. Health Perspect. 2007, 115, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Chiang, K.C.; Liao, C.M. Heavy incense burning in temples promotes exposure risk from airborne PMs and carcinogenic PAHs. Sci. Total. Environ. 2006, 372, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Chiang, K.C.; Chio, C.P.; Chiang, Y.H.; Liao, C.M. Assessing hazardous risks of human exposure to temple airborne polycyclic aromatic hydrocarbons. J. Hazard. Mater. 2009, 166, 676–685. [Google Scholar] [CrossRef] [PubMed]
- Chuang, H.C.; BéruBé, K.; Lung, S.C.C.; Bai, K.J.; Jones, T. Investigation into the oxidative potential generated by the formation of particulate matter from incense combustion. J. Hazard. Mater. 2013, 244, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Lung, S.C.C.; Hu, S.C. Generation rates and emission factors of particulate matter and particle-bound polycyclic aromatic hydrocarbons of incense sticks. Chemosphere 2003, 50, 673–679. [Google Scholar] [CrossRef]
- Jetter, J.J.; Guo, Z.; McBrian, J.A.; Flynn, M.R. Characterization of emissions from burning incense. Sci. Total. Environ. 2002, 295, 51–67. [Google Scholar] [CrossRef]
- Fang, G.C.; Chu, C.C.; Wu, Y.S.; Fu, P.P.C. Emission characters of particulate concentrations and dry deposition studies for incense burning at a Taiwanese temple. Toxicol. Ind. Health 2002, 18, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.S.H.; Yu, J.Z. Concentrations of formaldehyde and other carbonyls in environments affected by incense burning. J. Environ. Monit. 2002, 4, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Sexton, K.G.; Yeatts, K.B. Hazard assessment of United Arab Emirates (UAE) incense smoke. Sci. Total. Environ. 2013, 458, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Su, T.C.; Lin, Y.L.; Chan, C.C. Short-term effects of air pollution on pulse pressure among nonsmoking adults. Epidemiology 2012, 23, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Chuang, K.J.; Yan, Y.H.; Cheng, T.J. Effect of air pollution on blood pressure, blood lipids, and blood sugar: A population-based approach. J. Occup. Environ. Med. 2010, 52, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, M.; Hoffmann, B.; Hvidberg, M.; Ketzel, M.; Jensen, S.S.; Andersen, Z.J.; Tjonneland, A.; Overvad, K.; Raaschou Nielsen, O. Long-term exposure to traffic-related air pollution associated with blood pressure and self-reported hypertension in a Danish cohort. Environ. Health Perspect. 2012, 120, 418–424. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Hypertensive (N (%)) | Normotensive (N (%)) | p-Value * |
|---|---|---|---|
| Age (years, mean (SD)) | 61.03 (13.87) | 46.45 (15.27) | 0.01 |
| Sex | |||
| Male | 817 (70.86) | 2838 (64.04) | |
| Female | 336 (29.14) | 1594 (35.97) | 0.01 |
| BMI (kg/m2) | 23.59 (3.44) | 22.36 (2.84) | 0.01 |
| Monthly household income (RMB) | 4670 (7814) | 4947 (5771) | 0.31 |
| Ambient temperature (°C) | 22.40 (5.37) | 22.48 (5.01) | 0.63 |
| Education | |||
| Low | 732 (63.49) | 1717 (38.74) | |
| High | 421 (36.51) | 2715 (61.26) | 0.01 |
| Smoking status | |||
| Nonsmoker | 856 (74.24) | 3279 (73.98) | |
| Smoker | 297 (25.76) | 1153 (26.02) | 0.89 |
| ETS exposure # | |||
| Never | 455 (39.46) | 1584 (35.74) | |
| Ever | 698 (60.54) | 2848 (64.26) | 0.02 |
| Drinking status | |||
| Nondrinking | 852 (73.89) | 3140 (70.85) | |
| Drinking | 301 (26.11) | 1292 (29.15) | 0.05 |
| Physical exercise | |||
| No | 879 (76.24) | 2847 (64.25) | |
| Yes | 274 (23.76) | 1584 (35.75) | 0.01 |
| Indoor fuel type | |||
| Clean | 879 (76.24) | 3601 (81.25) | |
| Unclean | 274 (23.76) | 831 (18.75) | 0.01 |
| Ventilation | |||
| No | 197 (17.09) | 619 (13.97) | |
| Yes | 956 (82.91) | 3813 (86.03) | 0.01 |
| Salt restriction | |||
| No | 1070 (92.80) | 4133 (93.25) | |
| Yes | 82 (7.20) | 299 (6.75) | 0.70 |
| Variables | Hypertensive (N = 1153) | Normotensive (N = 4432) | Crude OR (95% CI) | p-Value | Adjusted OR* (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Overall | ||||||
| Incense Burning | ||||||
| No | 250 (21.68) | 1086 (24.50) | Reference | Reference | ||
| Yes | 903 (78.32) | 3346 (75.50) | 1.24 (1.03–1.50) | 0.02 | 1.18 (0.97–1.44) | 0.10 |
| Frequency of Incense Burning | ||||||
| Never | 250 (21.68) | 1086 (24.50) | Reference | Reference | ||
| Occasional | 663 (57.50) | 2634 (59.43) | 1.21 (0.99–1.48) | 0.06 | 1.16 (0.94–1.43) | 0.18 |
| Daily | 240 (20.82) | 712 (16.06) | 1.37 (1.04–1.80) | 0.03 | 1.27 (0.94–1.71) | 0.11 |
| P for trend | 0.02 | 0.05 | ||||
| Male | ||||||
| Incense Burning | ||||||
| No | 206 (25.21) | 810 (28.54) | Reference | Reference | ||
| Yes | 611 (74.79) | 2028 (71.46) | 1.18 (0.96–1.46) | 0.12 | 1.11 (0.88–1.39) | 0.39 |
| Frequency of Incense Burning | ||||||
| Never | 206 (25.21) | 810 (28.54) | Reference | Reference | ||
| Occasional | 429 (52.51) | 1508 (53.14) | 1.15 (0.95–1.77) | 0.24 | 1.08 (0.85–1.37) | 0.55 |
| Daily | 182 (22.28) | 520 (18.32) | 1.29 (0.95–1.77) | 0.11 | 1.20 (0.86–1.68) | 0.29 |
| P for trend | 0.09 | 0.29 | ||||
| Female | ||||||
| Incense Burning | ||||||
| No | 44 (13.10) | 276 (17.31) | Reference | Reference | ||
| Yes | 292 (86.90) | 1318 (82.69) | 1.50 (1.01–2.22) | 0.04 | 1.45 (0.96–2.20) | 0.08 |
| Frequency of Incense Burning | ||||||
| Never | 44 (13.10) | 276 (17.31) | Reference | Reference | ||
| Occasional | 234 (69.64) | 1126 (70.64) | 1.43 (0.96–2.14) | 0.08 | 1.39 (0.91–2.12) | 0.12 |
| Daily | 58 (17.26) | 192 (12.05) | 1.81 (1.06–3.09) | 0.03 | 1.79 (1.01–3.16) | 0.04 |
| P for trend | 0.03 | 0.04 | ||||
| Variable | Diastolic Blood Pressure | Systolic Blood Pressure | ||
|---|---|---|---|---|
| Estimate * (95% CI) | p-Value | Estimate * (95% CI) | p-Value | |
| Overall | ||||
| Incense burning | ||||
| No | Reference | Reference | ||
| Yes | 1.26 (0.69–1.83) | 0.01 | 1.02 (0.06–1.99) | 0.04 |
| Frequency of incense burning | ||||
| Never | Reference | Reference | ||
| Occasional | 1.25 (0.66–1.85) | 0.01 | 0.67 (−0.35–1.68) | 0.20 |
| Daily | 1.28 (0.52–2.05) | 0.01 | 2.09 (0.79–3.39) | 0.01 |
| P for trend | 0.01 | 0.01 | ||
| Males | ||||
| Incense burning | ||||
| No | Reference | Reference | ||
| Yes | 0.95 (0.26–1.63) | 0.01 | 0.89 (−0.27–2.05) | 0.13 |
| Frequency of incense burning | ||||
| Never | Reference | Reference | ||
| Occasional | 0.81 (0.08–1.53) | 0.03 | 0.30 (−0.93–1.52) | 0.63 |
| Daily | 1.30 (0.40–2.21) | 0.01 | 2.36 (0.83–3.89) | 0.01 |
| P for trend | 0.01 | 0.01 | ||
| Females | ||||
| Incense burning | ||||
| No | Reference | Reference | ||
| Yes | 2.05 (1.00–3.10) | 0.01 | 1.23 (−0.55–3.02) | 0.17 |
| Frequency of incense burning | ||||
| Never | Reference | Reference | ||
| Occasional | 2.20 (1.13–3.26) | 0.01 | 1.15 (−0.66–2.97) | 0.21 |
| Daily | 1.28 (−0.19–2.74) | 0.09 | 1.66 (−0.82–4.14) | 0.19 |
| P for trend | 0.03 | 0.17 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, X.; Ma, W.; Xu, X.; Liu, T.; Xiao, J.; Zeng, W.; Li, X.; Qian, Z.; Xu, Y.; Lin, H. The Association of Domestic Incense Burning with Hypertension and Blood Pressure in Guangdong, China. Int. J. Environ. Res. Public Health 2017, 14, 788. https://doi.org/10.3390/ijerph14070788
Song X, Ma W, Xu X, Liu T, Xiao J, Zeng W, Li X, Qian Z, Xu Y, Lin H. The Association of Domestic Incense Burning with Hypertension and Blood Pressure in Guangdong, China. International Journal of Environmental Research and Public Health. 2017; 14(7):788. https://doi.org/10.3390/ijerph14070788
Chicago/Turabian StyleSong, Xiuling, Wenjun Ma, Xiaojun Xu, Tao Liu, Jianpeng Xiao, Weilin Zeng, Xing Li, Zhengmin Qian, Yanjun Xu, and Hualiang Lin. 2017. "The Association of Domestic Incense Burning with Hypertension and Blood Pressure in Guangdong, China" International Journal of Environmental Research and Public Health 14, no. 7: 788. https://doi.org/10.3390/ijerph14070788
APA StyleSong, X., Ma, W., Xu, X., Liu, T., Xiao, J., Zeng, W., Li, X., Qian, Z., Xu, Y., & Lin, H. (2017). The Association of Domestic Incense Burning with Hypertension and Blood Pressure in Guangdong, China. International Journal of Environmental Research and Public Health, 14(7), 788. https://doi.org/10.3390/ijerph14070788