
Cost-Effectiveness of the Strategies to Reduce the Incidence of Dengue in Colima, México

 , , ,
, , , 
Abstract
:1. Introduction
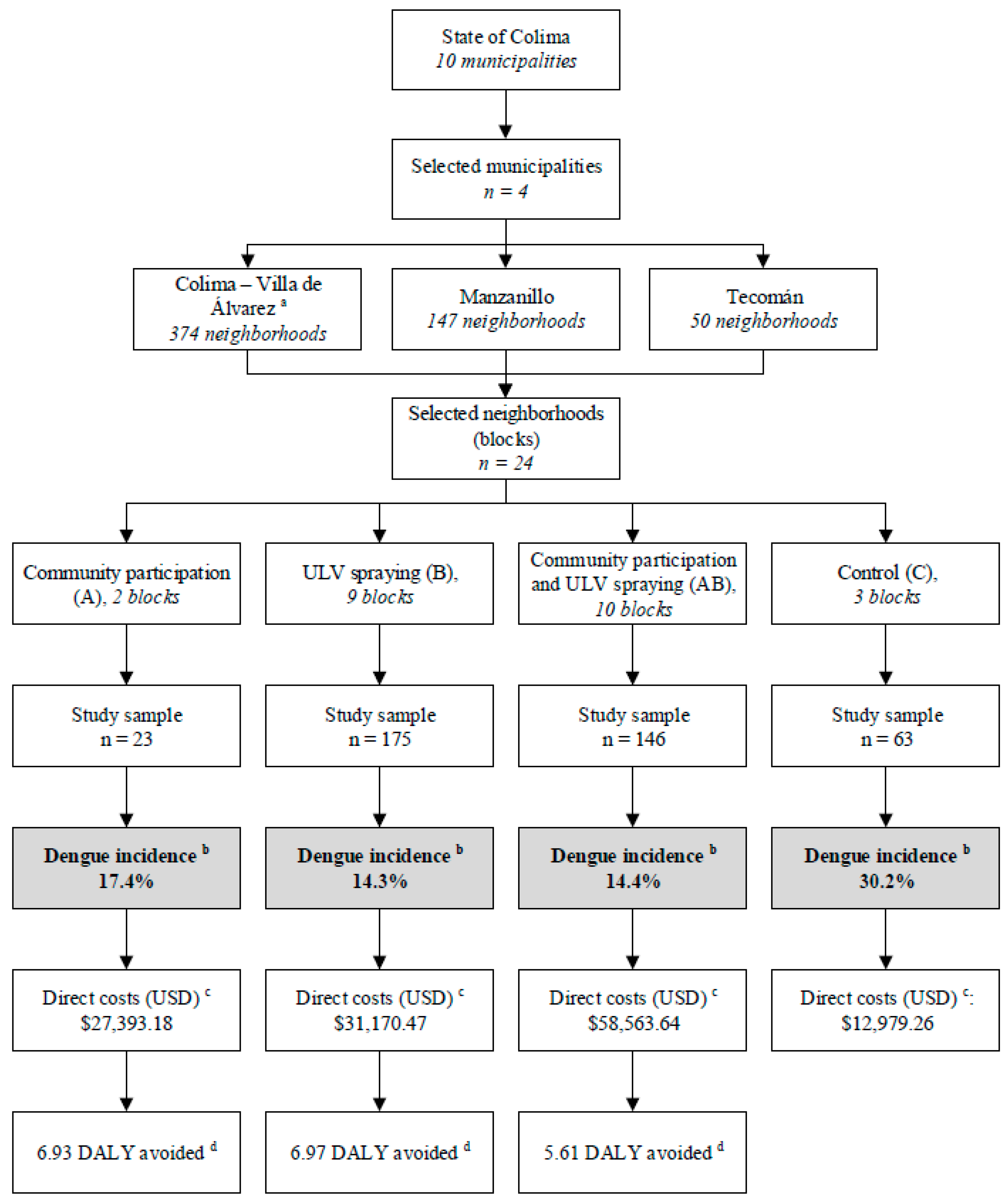
2. Methods
2.1. Direct Costs
2.2. Efficacy
2.3. Disability-Adjusted Life Years (DALYs)
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Da Rocha Taranto, M.F.; Pessanha, J.E.; dos Santos, M.; dos Santos Pereira Andrade, A.C.; Camargos, V.N.; Alves, S.N.; Di Lorenzo Oliveira, C.; Taranto, A.G.; dos Santos, L.L.; de Magalhaes, J.C.; et al. Dengue outbreaks in Divinopolis, south-eastern Brazil and the geographic and climatic distribution of Aedes albopictus and Aedes aegypti in 2011–2012. Trop. Med. Int. Health 2015, 20, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Murray, N.E.; Quam, M.B.; Wilder-Smith, A. Epidemiology of dengue: Past, present and future prospects. Clin. Epidemiol. 2013, 5, 299–309. [Google Scholar] [PubMed]
- Screaton, G.; Mongkolsapaya, J.; Yacoub, S.; Roberts, C. New insights into the immunopathology and control of dengue virus infection. Nat. Rev. Immunol. 2015, 15, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Narro-Robles, J.; Gomez-Dantes, H. Dengue in Mexico: A priority problem of public health. Salud Publica Mex. 1995, 37, S12–S20. [Google Scholar] [PubMed]
- Guzman, M.G.; Halstead, S.B.; Artsob, H.; Buchy, P.; Farrar, J.; Gubler, D.J.; Hunsperger, E.; Kroeger, A.; Margolis, H.S.; Martinez, E.; et al. Dengue: A continuing global threat. Nat. Rev. Microbiol. 2010, 8, S7–S16. [Google Scholar] [CrossRef] [PubMed]
- Anez, G.; Balza, R.; Valero, N.; Larreal, Y. Economic impact of dengue and dengue hemorrhagic fever in the State of Zulia, Venezuela, 1997–2003. Rev. Panam. Salud Publica 2006, 19, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Espinoza-Gomez, F.; Hernandez-Suarez, C.M.; Rendon-Ramirez, R.; Carrillo-Alvarez, M.L.; Flores-Gonzalez, J.C. Transmisión interepidémica del dengue en la ciudad de Colima, México. Salud Publica Mex. 2003, 45, 365–370. [Google Scholar] [CrossRef] [PubMed]
- De la Cruz, R.M. La Participación Comunitaria en la Prevención del Dengue; Universidad de Colima: Colima, Mexico, 2013; pp. 52–53. ISBN 978-607-8356-03-4. [Google Scholar]
- Mexican Federal Government. NORMA Oficial Mexicana NOM-032-SSA2-2002, Para la Vigilancia Epidemiológica, Prevención y Control de Enfermedades Transmitidas por Vector; Mexican Federal Government: Mexico DF, Mexico, 2002.
- Diaz-Quinonez, J.A.; Escobar-Escamilla, N.; Ortiz-Alcantara, J.; Vazquez-Pichardo, M.; de la Luz Torres-Rodriguez, M.; Nunez-Leon, A.; Torres-Longoria, B.; Lopez-Martinez, I.; Ruiz-Matus, C.; Kuri-Morales, P.; et al. Identification of Asian genotype of chikungunya virus isolated in Mexico. Virus Genes 2016, 52, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Quinonez, J.A.; Lopez-Martinez, I.; Torres-Longoria, B.; Vazquez-Pichardo, M.; Cruz-Ramirez, E.; Ramirez-Gonzalez, J.E.; Ruiz-Matus, C.; Kuri-Morales, P. Evidence of the presence of the Zika virus in Mexico since early 2015. Virus Genes 2016, 52, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Sanchez, L.; Perez, D.; Carbonell, N.; Lefevre, P.; Vanlerberghe, V.; Van der Stuyft, P. A community empowerment strategy embedded in a routine dengue vector control programme: A cluster randomised controlled trial. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, L.; Perez, D.; Cruz, G.; Castro, M.; Kouri, G.; Shkedy, Z.; Vanlerberghe, V.; Van der Stuyft, P. Intersectoral coordination, community empowerment and dengue prevention: Six years of controlled interventions in Playa Municipality, Havana, Cuba. Trop. Med. Int. Health TM IH 2009, 14, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, L.; Perez, D.; Perez, T.; Sosa, T.; Cruz, G.; Kouri, G.; Boelaert, M.; Van der Stuyft, P. Intersectoral coordination in Aedes aegypti control. A pilot project in Havana City, Cuba. Trop. Med. Int. Health TM IH 2005, 10, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Phuanukoonnon, S.; Brough, M.; Bryan, J.H. Folk knowledge about dengue mosquitoes and contributions of health belief model in dengue control promotion in Northeast Thailand. Acta Trop. 2006, 99, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Espinoza-Gomez, F.; Hernandez-Suarez, C.M.; Coll-Cardenas, R. Educational campaign versus malathion spraying for the control of Aedes aegypti in Colima, Mexico. J. Epidemiol. Community Health 2002, 56, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Liu, T.; Song, T.; Lin, L.; Xiao, J.; Lin, J.; He, J.; Zhong, H.; Hu, W.; Deng, A.; et al. Community involvement in dengue outbreak control: An integrated rigorous intervention strategy. PLoS Negl. Trop. Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Chow, J.; Shahid-Salles, S.A. Intervention cost-effectiveness: overview of main messages. In Disease Control Priorities in Developing Countries, 2nd ed.; Jamison, D.T., Breman, J.G., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA; Oxford University Press: New York, NY, USA, 2006; Chapter 2. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11784/ (accessed on 29 May 2017).
- Toledo Romani, M.E.; Vanlerberghe, V.; Perez, D.; Lefevre, P.; Ceballos, E.; Bandera, D.; Baly Gil, A.; Van der Stuyft, P. Achieving sustainability of community-based dengue control in Santiago de Cuba. Soc. Sci. Med. 2007, 64, 976–988. [Google Scholar] [CrossRef] [PubMed]
- Poupardin, R.; Riaz, M.A.; Jones, C.M.; Chandor-Proust, A.; Reynaud, S.; David, J.P. Do pollutants affect insecticide-driven gene selection in mosquitoes? Experimental evidence from transcriptomics. Aquat. Toxicol. 2012, 114–115, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Ranson, H.; N’Guessan, R.; Lines, J.; Moiroux, N.; Nkuni, Z.; Corbel, V. Pyrethroid resistance in African anopheline mosquitoes: What are the implications for malaria control? Trends Parasitol. 2011, 27, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Nkya, T.E.; Akhouayri, I.; Kisinza, W.; David, J.P. Impact of environment on mosquito response to pyrethroid insecticides: Facts, evidences and prospects. Insect Biochem. Mol. Biol. 2013, 43, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Stiller-Winkler, R.; Hadnagy, W.; Leng, G.; Straube, E.; Idel, H. Immunological parameters in humans exposed to pesticides in the agricultural environment. Toxicol. Lett. 1999, 107, 219–224. [Google Scholar] [CrossRef]
- Dewailly, E.; Forde, M.; Robertson, L.; Kaddar, N.; Laouan Sidi, E.A.; Cote, S.; Gaudreau, E.; Drescher, O.; Ayotte, P. Evaluation of pyrethroid exposures in pregnant women from 10 Caribbean countries. Environ. Int. 2014, 63, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Champer, J.; Reeves, R.; Oh, S.Y.; Liu, C.; Liu, J.; Clark, A.G.; Messer, W. Novel CRISPR/Cas9 gene drive constructs reveal insights into mechanisms of resistance allele formation and drive efficiency in genetically diverse populations. PLoS Genet. 2017, 13. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Item | Intervention Phases | Cost ($) | ||||
|---|---|---|---|---|---|---|
| P/C | I | E | Co. | Unit | Total | |
| Community participation (A) | ||||||
| Instructors (hours) | 170 | 480 | 200 | 240 | 4.94 | 5381.51 |
| Students (hours) | - | 480 | 100 | 240 | 1.25 | 1030.52 |
| Community leaders (hours) | - | 240 | - | - | 3.59 | 3447.04 |
| Support staff (months) | 0.5 | 2 | 1 | - | 1077.20 | 3770.20 |
| Printed materials (units) | 66 | 360 | 140 | - | 0.45 | 254.04 |
| Computers rent (hours) | 100 | 160 | 50 | 40 | 0.90 | 314.18 |
| Headquarters rent (months) | 2 | 2 | 2 | 2 | 538.60 | 4308.80 |
| Food/Transportation allowance (day) | 25 | 40 | 10 | 35 | 26.93 | 8886.89 |
| Total | 27,393.18 | |||||
| ULV spraying (B) | ||||||
| Coordinators (hours) | 20 | 200 | 50 | - | 4.94 | 7271.10 |
| Technical staff (hours) | 40 | 320 | - | - | 1.25 | 705.48 |
| Community leaders (hours) | - | 440 | - | - | 0.90 | 394.97 |
| ULV equipment and pesticide (hours) | - | 480 | - | - | 26.93 | 12,926.39 |
| Pick-up vehicle (day) | - | 15 | - | - | 134.65 | 2356.37 |
| Headquarter rent (month) | 2 | 4 | 2 | - | 538.60 | 5026.93 |
| Food/Transportation allowance (day) | 10 | 15 | 10 | - | 35.91 | 2513.46 |
| Total | 31,170.47 | |||||
| Community participation and ULV spraying (AB) | ||||||
| Total | 58,563.64 | |||||
| Control (C) | ||||||
| Coordinators (hours) | 20 | 200 | 50 | - | 4.94 | 7271.10 |
| Technical staff (hours) | 40 | 320 | - | - | 1.25 | 681.24 |
| Headquarter rent (month) | 2 | 4 | 2 | - | 538.60 | 5026.93 |
| Total | 12,979.26 | |||||
| Group | Cases Tested/Positives | Incidence a | Incidence Treated by C b | Efficiency c | Effectiveness d |
|---|---|---|---|---|---|
| A | 23/4 | 17.4% (12.6–24) | 0.58 | 0.423 | 6.93 |
| B | 175/25 | 14.3% (9.3–19.3) | 0.47 | 0.526 | 6.97 |
| AB | 146/20 | 14.4% (9.4–19.2) | 0.48 | 0.523 | 5.61 |
| C | 63/19 | 30.2% (20–40) | 1.00 | 0 | 0 |
| Group | Costs ($) per DALY a |
|---|---|
| A | 3952.84 |
| B | 4472.09 |
| AB | 10,439.15 |
| C | - |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendoza-Cano, O.; Hernandez-Suarez, C.M.; Trujillo, X.; Ochoa Diaz-Lopez, H.; Lugo-Radillo, A.; Espinoza-Gomez, F.; De la Cruz-Ruiz, M.; Sánchez-Piña, R.A.; Murillo-Zamora, E. Cost-Effectiveness of the Strategies to Reduce the Incidence of Dengue in Colima, México. Int. J. Environ. Res. Public Health 2017, 14, 890. https://doi.org/10.3390/ijerph14080890
Mendoza-Cano O, Hernandez-Suarez CM, Trujillo X, Ochoa Diaz-Lopez H, Lugo-Radillo A, Espinoza-Gomez F, De la Cruz-Ruiz M, Sánchez-Piña RA, Murillo-Zamora E. Cost-Effectiveness of the Strategies to Reduce the Incidence of Dengue in Colima, México. International Journal of Environmental Research and Public Health. 2017; 14(8):890. https://doi.org/10.3390/ijerph14080890
Chicago/Turabian StyleMendoza-Cano, Oliver, Carlos Moisés Hernandez-Suarez, Xochitl Trujillo, Héctor Ochoa Diaz-Lopez, Agustin Lugo-Radillo, Francisco Espinoza-Gomez, Miriam De la Cruz-Ruiz, Ramón Alberto Sánchez-Piña, and Efrén Murillo-Zamora. 2017. "Cost-Effectiveness of the Strategies to Reduce the Incidence of Dengue in Colima, México" International Journal of Environmental Research and Public Health 14, no. 8: 890. https://doi.org/10.3390/ijerph14080890
APA StyleMendoza-Cano, O., Hernandez-Suarez, C. M., Trujillo, X., Ochoa Diaz-Lopez, H., Lugo-Radillo, A., Espinoza-Gomez, F., De la Cruz-Ruiz, M., Sánchez-Piña, R. A., & Murillo-Zamora, E. (2017). Cost-Effectiveness of the Strategies to Reduce the Incidence of Dengue in Colima, México. International Journal of Environmental Research and Public Health, 14(8), 890. https://doi.org/10.3390/ijerph14080890