1. Introduction
Exposure to arsenic has been epidemiologically linked to myriad health conditions including cardiovascular disease, diabetes, and cancer [
1]. Exposure to inorganic arsenic most commonly occurs through ingesting contaminated water sources and arsenic biotransformations in the liver increase the presence of highly toxic methylated arsenic metabolites [
2,
3,
4]. Methylated arsenicals increase reactive oxygen species (ROS) to a greater extent than inorganic arsenic, thus, arsenic methylation may be associated with increased disease prevalence [
3].
Arsenic is a widespread environmental contaminant commonly found in air, water, soil, and sediments. Arsenic levels in soil range from 1 to 40 mg/kg, and arsenic levels in air range from 0.007 to 28 ng/m
3 in rural areas to 3–200 ng/m
3 in urban areas [
5,
6]. Untreated waters can reach several hundred to several thousand ppb arsenic, and the World Health Organization (WHO) recommends a maximum contaminant level (MCL) for arsenic in drinking water of 10 ppb [
6]. Arsenic can be inhaled, ingested, or absorbed through the skin. The American Conference of Governmental Hygienists recommend a Biological Exposure Index (BEI) level of 35 μM for total urine arsenic [
7].
Arsenic has been classified as a strong carcinogen [
8], and is estimated to contribute to as much as 21.4% of all causes of mortality in highly exposed regions of the world [
9]. Chronic exposure to arsenic has been associated with elevated risk of cardiovascular disease (CVD) endpoints including ischemic heart disease incidence and mortality in several American Indian populations with water sources measured up to 21 ppb arsenic [
10] and among populations in Bangladesh, over half of which consume ground water that substantially exceeds 50 ppb arsenic [
9]. Increased rates of cerebrovascular disease prevalence have been observed among residents of Taiwan with water sources that can exceed 300 ppb arsenic [
11], and increased severity of atherosclerosis was observed among subjects in rural Taiwan with median arsenic concentrations in drinking water between 700 and 930 ppb [
12]. Additionally, a recent meta-analysis demonstrated a positive association between arsenic exposure and hypertension among 11 cross-sectional studies of subjects with various levels of arsenic exposure [
13].
Arsenic exposure is also associated with a diagnosis of metabolic syndrome, a risk factor for CVD. Metabolic syndrome is defined as the presence of at least three out of five components including elevated fasting glucose, hypertension, elevated triglycerides, large waist circumference, and low HDL cholesterol [
14]. Inorganic arsenic exposure was associated with a clinical diagnosis of metabolic syndrome, elevated plasma glucose, and elevated blood lipids among residents in an industrial region of Taiwan exposed to arsenic both occupationally and through water sources measured up to 16 ppb [
15]. Importantly, inflammation and oxidative stress are significant mechanisms linking metabolic syndrome and cardiovascular disease [
16]. Furthermore, both arsenic exposure and arsenic methylation are associated with oxidative stress and the generation of ROS [
2,
17,
18], thus, there is a plausible mechanistic link between arsenic and metabolic syndrome.
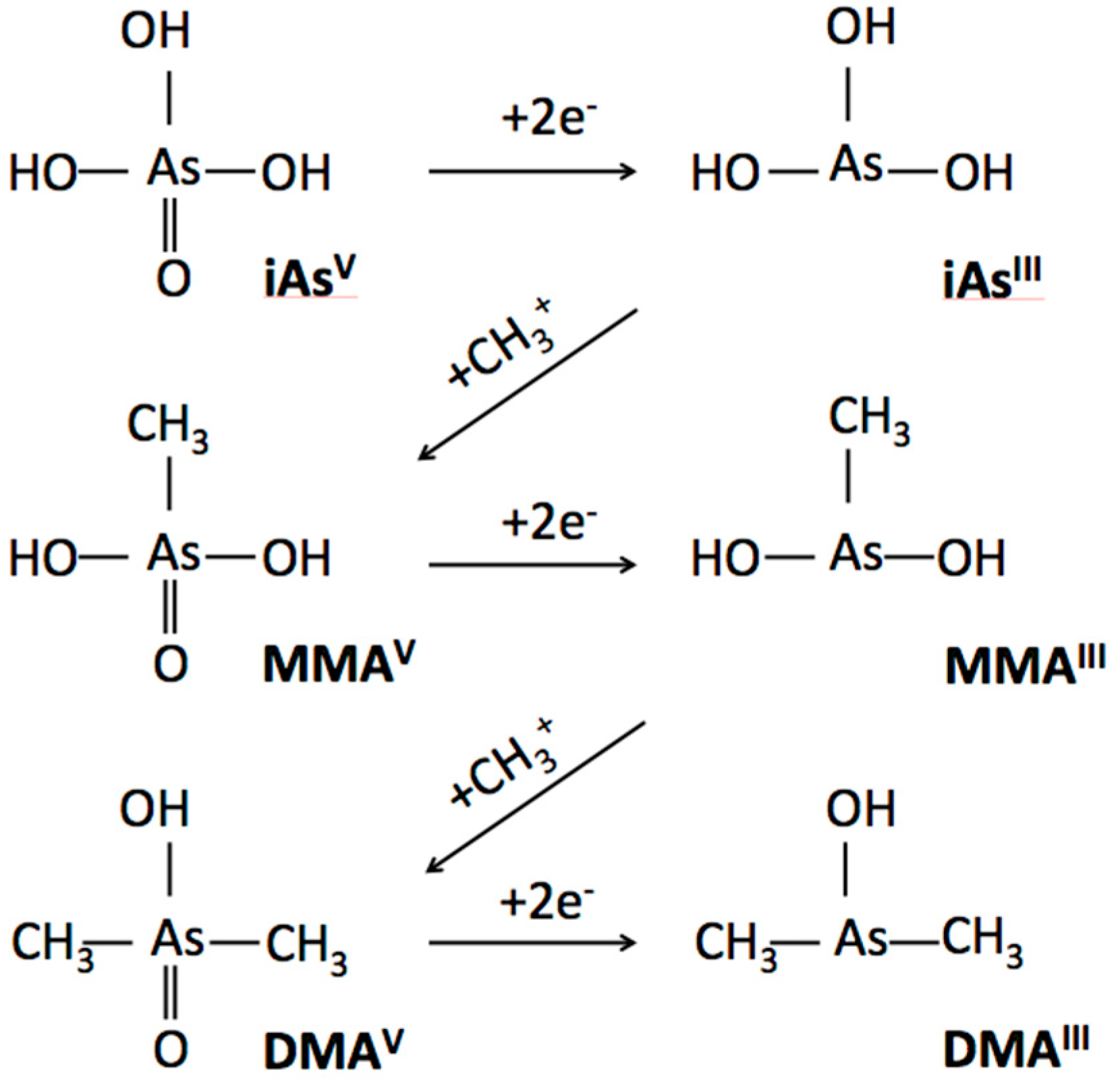
Arsenic methylation capacity is a recognized risk factor for arsenic toxicity, and may contribute to CVD susceptibility. Inorganic arsenic (iAs) undergoes biotransformation in which iAs is methylated to monomethylarsonic acid (MMA(V)). MMA(V) is then reduced to monomethylarsonous acid (MMA(III)), which is methylated to dimethylarsinic acid (DMA(V)). DMA(V) is then reduced to dimethylarsinous acid (DMA(III)). Methylated arsenic species, especially those in the trivalent form, are significantly more toxic than inorganic arsenic compounds [
2,
3,
5]. Arsenic methylation capacity is measured as the proportion of methylated arsenicals in urine or as a ratio of MMA:iAs (termed primary methylation index or PMI) and ratio of DMA:MMA (termed secondary methylation index or SMI). Arsenic methylation facilitates urinary excretion, yet also increases the bioavailability of toxic methylated arsenicals [
3]. Interestingly, methylation capacity is not highly associated with inorganic arsenic exposure [
19], but is influenced by genetics, gender, age, and BMI [
20,
21].
Incomplete arsenic methylation is characterized by a pattern of higher urine proportion MMA, lower urine proportion DMA, increased PMI, and decreased SMI, whereas more complete arsenic methylation is characterized by a pattern of lower urine proportion MMA, higher urine proportion DMA, decreased PMI and increased SMI. Although only a limited number of studies have investigated the impact of arsenic methylation on cardiovascular disease or metabolic syndrome, the available evidence suggests that complete methylation may be a contributing factor [
22]. Importantly, this association has not been investigated in a relatively low arsenic-exposed population. Indeed, reports of adverse health outcomes associated with arsenic exposure and arsenic methylation have originated from regions where arsenic concentrations are unregulated or significantly under-regulated and thus exceed current safety guidelines. In contrast, we assessed the relationship between arsenic methylation and pre-clinical biomarkers of cardiovascular disease in a general sample of the U.S. where despite widespread compliance with current treatment standards for arsenic in food and water, appreciable concentrations of arsenic are still detectable in the blood and urine of U.S. residents [
23,
24,
25,
26].
The present study uses U.S. NHANES 2013–2014 data to investigate the association between urine %iAs, %MMA, %DMA, and indices of primary methylation (PMI) and secondary methylation (SMI), with respect to a clinical diagnosis of metabolic syndrome.
4. Discussion
Ours is the first study to investigate the association between arsenic methylation and metabolic syndrome in a population with relatively low arsenic exposure. We report no association between arsenic methylation and metabolic syndrome after adjusting for relevant covariates in the majority of a population relying on water with arsenic levels regulated at 10 ppb. However, we can not rule out the possibility of an association between increased arsenic methylation and increased odds of metabolic syndrome among a small subsample of women with normal BMI, and among women with obese BMI.
4.1. Oxidative Stress & Inflammation
Metabolic syndrome is associated with a clustering of abnormalities that lead to increased cardiovascular risk. Inflammation is an important cellular mechanism that links metabolic syndrome to cardiovascular disease [
16]. For example, obesity (a central component of metabolic syndrome) is associated with overexpression of tumor necrosis factor α (TNF-α), a cell signaling protein involved in systematic inflammation [
36], and high fat intake contributes to increased oxidative stress and nuclear factor (NF-κB) activation, a proinflammatory signaling pathway [
37]. Additionally, the inflammatory marker C-reactive protein (CRP) statistically enhances the relationship between metabolic syndrome and coronary heart disease events [
38]. Furthermore, oxidative stress is believed to contribute to metabolic syndrome [
39], hyperglycemia [
40], dyslipidemia [
41], and obesity [
42].
Oxidative stress has also been convincingly linked with exposure to arsenic. Indeed, exposure to inorganic arsenic and its metabolites can generate ROS and free radicals, hydroxyl radicals, nitric oxide, and superoxide anion in a variety of cell lines [
2,
18]. Additionally, a human study conducted among a highly arsenic exposed population in China reported that arsenic-exposed subjects demonstrated higher oxidative stress compared to control subjects (measured as increased serum levels of lipid peroxide) [
17]. Importantly the same study reported a significant correlation between oxidative stress and methylated arsenic metabolites [
17].
Thus, there is evidence for an association between arsenic and oxidative stress, as well as evidence of a link between oxidative stress and metabolic syndrome. This association, however, may be limited to populations exposed to high levels of arsenic. Indeed, our main finding of no association between arsenic methylation and metabolic syndrome contrasts with past investigations conducted among populations with higher overall arsenic exposure. For example, in regions of Taiwan with exposure to industrial arsenic as well as water sources measured up to 16 ppb, Wang et al., (2007) reported a positive association between total arsenic and metabolic syndrome [
15] and Chen et al., (2012) reported that low primary methylation (low %MMA) was associated with a higher risk for metabolic syndrome in a population exposed to median arsenic concentrations of 700–930 ppb [
22]. Although a minority of findings suggest that incomplete methylation (high urinary proportion of MMA) is a stronger contributor to cardiovascular disease [
43] and hypertension [
44], this may result from differences in the valence state of measured arsenicals. For example, studies demonstrating elevated toxicity of complete methylation have included trivalent and pentavalent species in calculations of urinary arsenic proportion, whereas studies reporting the opposite trend measured only the less toxic pentavalent species [
43] or failed to specify the valence states of measured arsenicals [
44]. In the present study, we report that in general, increased arsenic methylation is not associated with increased odds of metabolic syndrome, with the possible exception of specific subgroups.
4.2. Increased Toxicity of Methylated Species
Following ingestion and tissue distribution, a series of biotransformations in the liver reduce arsenate (iAs(V)) to arsenite (iAs(III)) and arsenic methyltransferase enzymes mediate the sequential addition of methyl ions from
S-adenosylmethionine, alternated with arsenic species’ reductions [
45]. Thus, ingested inorganic arsenic is sequentially converted to its mono- and di- methylated forms and removed through the urinary system (
Figure 1).
Once considered a detoxification reaction, a growing body of evidence demonstrates that arsenic methylation significantly increases toxicity and that trivalent species are more toxic than pentavalent species [
2,
3,
5,
46]. Individual variability in arsenic biotransformation is measured as the proportion of each arsenic species in urine, or by calculating PMI and SMI. Variation in urine metabolites have been associated with a variety of arsenic-related diseases [
43,
47] and may reflect differential bioavailability of arsenicals across individuals [
48].
4.3. Arsenic Distribution Patterns
Other notable findings from the present study are the similarities in arsenic methylation patterns in our sample of the U.S. compared to regions with higher exposure, as well as similarities with respect to individual variation in methylation capacity [
19]. Urinary proportions of arsenic species found in the present study are consistent with reports that most individuals have 10–30%iAs, 10–20%MMA, and 60–80%DMA, regardless of their arsenic exposure level [
19]. Our sample had 9.68% (±6.70), 11.69% (±9.94), and 78.63% (±9.94) urinary iAs, MMA, and DMA, respectively. The average total urinary arsenic in the U.S. NHANES 2013–2014 population was 15.67 μg/L, considerably lower than the total urinary arsenic reported in the aforementioned studies of pre and post-clinical CVD outcomes, where total mean urinary arsenic has ranged from 53.6 μg/L among women from southwest U.S. and northwest Mexico [
49] to 580 μg/L among a northern Chile population [
19]. Relative consistency in average arsenic methylation capacity among different populations irrespective of arsenic exposure was also reported by Hopenhayn-Rich et al., (1996), who detected only subtle (2–3%) differences in mean urine proportion of MMA and DMA between populations exposed to inorganic arsenic at levels differing by 500 ppb [
19].
In contrast to the relative consistency of arsenic methylation patterns between study populations, considerable variability has been reported in methylation capacity between individuals in the same population [
35]. For example, subjects in San Pedro ranged from approximately 40% to over 90% urinary DMA and from 7% to 40% urinary MMA [
19]. In the present study, urine percent MMA ranged from below detection limits to 34.22%, and urine percent DMA ranged from 41.16% to 98.74%.
4.4. Gender & BMI
Past studies suggest that variability in methylation capacity is due, in part to variations in genetic polymorphisms, as well as age, BMI, and gender [
20,
21]. Our results also demonstrate an effect of gender and BMI on arsenic metabolism. In the present study, we report that increased arsenic methylation may be associated with increased odds of metabolic disorder in gender and BMI stratified samples of the U.S. NHANES population adjusted for relevant covariates.
Our finding that gender modifies the effect of arsenic methylation on the odds of metabolic syndrome is supported by previous research conducted by Lindberg et al., (2008) who reported that women in Bangladesh had higher methylation efficiency than men during childbearing ages (20 to 60 years) [
19]. Similarly, European women between the ages of 20 and 60 had an increased rate of arsenic methylation [
21]. The authors of these studies speculate that sex hormones are partially responsible for increased rates of methylation in women, as it is specific to women of childbearing age [
20,
21]. This is a plausible explanation for some of the observed differences in metabolic syndrome outcomes based on gender in the present study, as 79% of women in our sample were between the ages of 20–60.
The present study also demonstrated a significant effect of BMI on arsenic methylation. Subjects with obese BMI expressed a pattern of increased arsenic methylation: significantly lower %iAs and %MMA, and significantly higher %DMA and SMI compared to subjects with normal BMI. Since increased arsenic methylation is generally associated with increased disease status, we expected to see a significant association between arsenic methylation and metabolic syndrome in obese subjects. Contrary to our expectations, we report no significant association between increased arsenic methylation and metabolic syndrome in over 98% of our sample population. We did, however, detect a positive association between increased arsenic methylation and metabolic syndrome in a small subpopulation represented by women with normal BMI.
We were interested in which clinical symptoms characterized metabolic syndrome in subjects who had metabolic syndrome and normal BMI. Among these 16 women, we found that 13 had elevated fasting glucose, 11 had elevated triglycerides, 14 had elevated blood pressure, and 12 had low HDL cholesterol. The most common combination of symptoms were elevated blood pressure and elevated glucose in combination with low HDL cholesterol (n = 7) or elevated triglycerides (n = 6). Despite the small sample size, ours is the first study to report the possibility of BMI as an effect modifier in the association between arsenic methylation and metabolic syndrome. We suggest that future studies investigate this possibility in a larger sample size.
4.5. Selection of Adjustment Factors
It is worth noting that we adjusted for covariates similar to those used in other studies assessing the relationship between arsenic exposure or arsenic methylation and various aspects of metabolic syndrome. These varied somewhat based on the specific research question, but generally included age, gender, BMI, smoking status, alcohol use, diabetes, waist to hip ratio, serum lipid levels, urine creatinine, and urine arsenobetaine [
10]. In the present study, we adjusted for age, poverty status, smoking status, and race, and stratified by gender and BMI category. These covariates are used in comparable studies with biological relevance verified in the literature [
50]. Additionally, we report no significant effect of controlling for urine creatinine, total arsenic, or eliminating diabetic subjects. We did, however, determine that limiting our analysis to subjects above detection limits for MMA eliminated the statistical significance between incomplete arsenic methylation and metabolic syndrome in overweight subjects. This suggests that the apparent protective effect of overweight BMI was not a true effect, but rather, was due to exposure misclassification as a large number of subjects in the overweight BMI group had undetectable arsenic levels. Although we used a commonly accepted practice by assigning a value of the LLOD/√2 to subjects below detection limits, this erroneously resulted in an apparent protective effect of overweight BMI, which we deemed implausible. Sensitivity analysis revealed that this was likely an artifact of our statistical method, and not a true effect.
We also probed our model by controlling for arsenobetaine and found that in women with obese BMI, the role of arsenic methylation on metabolic syndrome was masked by the effect of seafood consumption. By re-evaluating our final model after controlling for seafood consumption (i.e., adjusting for arsenobetaine), we detected a significant association between increased arsenic methylation (SMI) and metabolic syndrome in obese women. Navas-Acien et al., (2011) report that seafood is a significant determinant of urine concentrations of total arsenic and arsenic species [
51]. Arsenobetaine is an organic form of arsenic present in high levels in seafood that is excreted unchanged via the kidneys. Navas-Acien et al., (2011) also suggest eliminating subjects who have consumed seafood in the last 24-h from statistical analyses as a further safeguard from misclassifying arsenic exposure [
51]. In the present study, statistically controlling for arsenobetaine altered the statistical significance of our results among female subjects with obese BMI, whereas controlling for arsenobetaine did not alter the statistical significance of our results in women with normal or overweight BMI. We suggest that future studies should assess the possibility that the effect of seafood consumption on arsenic methylation varies as a function of BMI.
4.6. Policy Implications
An important implication of our study is the relevance of public water testing and treatment. The current U.S. standard was reduced from 50 ppb to 10 ppb by the U.S. EPA’s 2001 Revised Arsenic Rule. In a recent study, Welch et al., (2017) report that arsenic levels in the general U.S. population have declined over a 12-year period in accordance with the Revised Arsenic Rule [
52]. Although the current MCL fails to consider cardiovascular outcomes, diabetes, and preclinical indictors of CVD that may be associated with arsenic exposures below 10 ppb, the present study suggests that an MCL of 10 ppb arsenic is adequate to prevent arsenic exposure from contributing to metabolic syndrome in the general U.S. population. However, not all waters are subject to EPA standards, potentially placing an unequal health burden on regions with naturally higher arsenic concentrations and greater reliance on unregulated water sources. Approximately 12% of the U.S. population is served by domestic wells that are not regulated by the EPA, and 11–19% of private wells are estimated to contain arsenic in excess of 10 ppb [
52,
53]. For example, rural areas of the U.S. with a higher proportion of un-piped water report much higher concentrations of groundwater arsenic. A survey of 102 homes using domestic wells in rural areas of Nevada averaged 356 μg/L arsenic pre-treatment and 87 μg/L arsenic following reverse osmosis treatment [
54], and arsenic concentrations were measured between 10 and 61 ppb on rural Reservation lands in Arizona [
10]. Even populations using piped water on Reservation lands are at risk of consuming high concentrations of arsenic. Indeed, health-related violations relating to one or more substance above the MCL were reported among 46% of public water systems on Reservations, compared to just 7% among public water systems in the remainder of the U.S. [
55]. Furthermore, socio-economically disadvantaged communities in the U.S. may face disproportionate arsenic exposure. For example, Balazs et al., (2012) report that community water systems serving a higher proportion of minority residents with low socioeconomic status in the San Joaquin Valley have higher drinking water levels and greater odds of non-compliance with current arsenic standards [
56]. Unfortunately, despite the real and significant risk to rural and Native American populations, rural areas represent a small fraction of the total U.S. population and based on de-identification practices in the U.S. NHANES data, it is not possible to determine what proportion of our sample, if any, was represented by subjects living on Reservation lands. We suggest that future studies in the U.S. focus on marginalized populations who may be at greater risk of arsenic exposure due to non-compliance or lack of regulation.
Looking beyond the U.S., global drinking water arsenic regulations range from 6 ppb in Sweden to 50 ppb in Bangladesh, though there are vast disparities in regional infrastructures that support water testing, reporting, and remediation for arsenic. For example, despite regulations, a 2009 survey of 15,000 randomized households in Bangladesh estimated that 22 million people consume water exceeding 50 ppb and 5.6 million people consume water exceeding 200 ppb arsenic [
57]. However, there is no reliable estimate of the global scope of arsenic exposure due to delayed health effects, poor reporting, and low levels of awareness in some regions [
6]. It is also worth noting that industrial exposures may significantly contribute to arsenic body burden. For instance, Vimercati et al., (2017) report that urinary arsenic concentrations were higher among southern Italian residents who lived close to industrial plants [
58]. Therefore we suggest the need for future studies comparing the effectiveness of policy enforcing an MCL of 10 ppb arsenic on preclinical biomarkers of CVD in a model that establishes causality, as well as a need for comprehensive biomonitoring studies that consider all exposure routes.
Important limitations in the present study include reliance on secondary data and the use of self-reported data for several measures (e.g., diabetes, smoking status, and the use of medication). All biological data was collected by U.S. NHANES personnel, and therefore we did not have access to data on methylated arsenicals speciated by valence state. Additionally, as our sample originated from two different subsamples, we were unable to use the U.S. NHANES weighting factors and are thus unable to apply our findings to the entire U.S. population. Finally, our study design allows for an interpretation of correlation but not causation. Despite these limitations, this is the first study to examine urinary arsenic methylation with respect to metabolic disorder in the U.S. We also acknowledge that our stratified sample sizes were small, and these outcomes should be assessed in a larger population.
5. Conclusions
In summary, in a country where arsenic levels are regulated at 10 ppb in public drinking water, we report no significant association between arsenic methylation capacity and metabolic syndrome in the majority of our sample, however, we can not rule out the possibility of a positive association between increased arsenic methylation capacity and metabolic syndrome in women with normal BMI. Our sample represents a relatively low exposure population, and the association between arsenic methylation with metabolic syndrome should be assessed in regions of the world that lack the infrastructure for water testing and treatment and in regions of the U.S. that have a greater risk of arsenic exposure, such as American Indian Reservations, rural communities relying on untreated waters from private domestic wells, and regions with community water systems serving minority or low income populations. We emphasize the need for studies that highlight the impact of policy enforcement on urinary arsenic and health outcomes, as well as additional studies that consider the contribution of gender, BMI, and other factors that may modify the association of arsenic methylation to pre- and post-clinical cardiovascular disease status in a model that establishes causality.




{kind=link}