Children’s Independent Mobility: Current Knowledge, Future Directions, and Public Health Implications


Abstract
1. Introduction
2. Children’s Independent Mobility—Indicators and Measurements
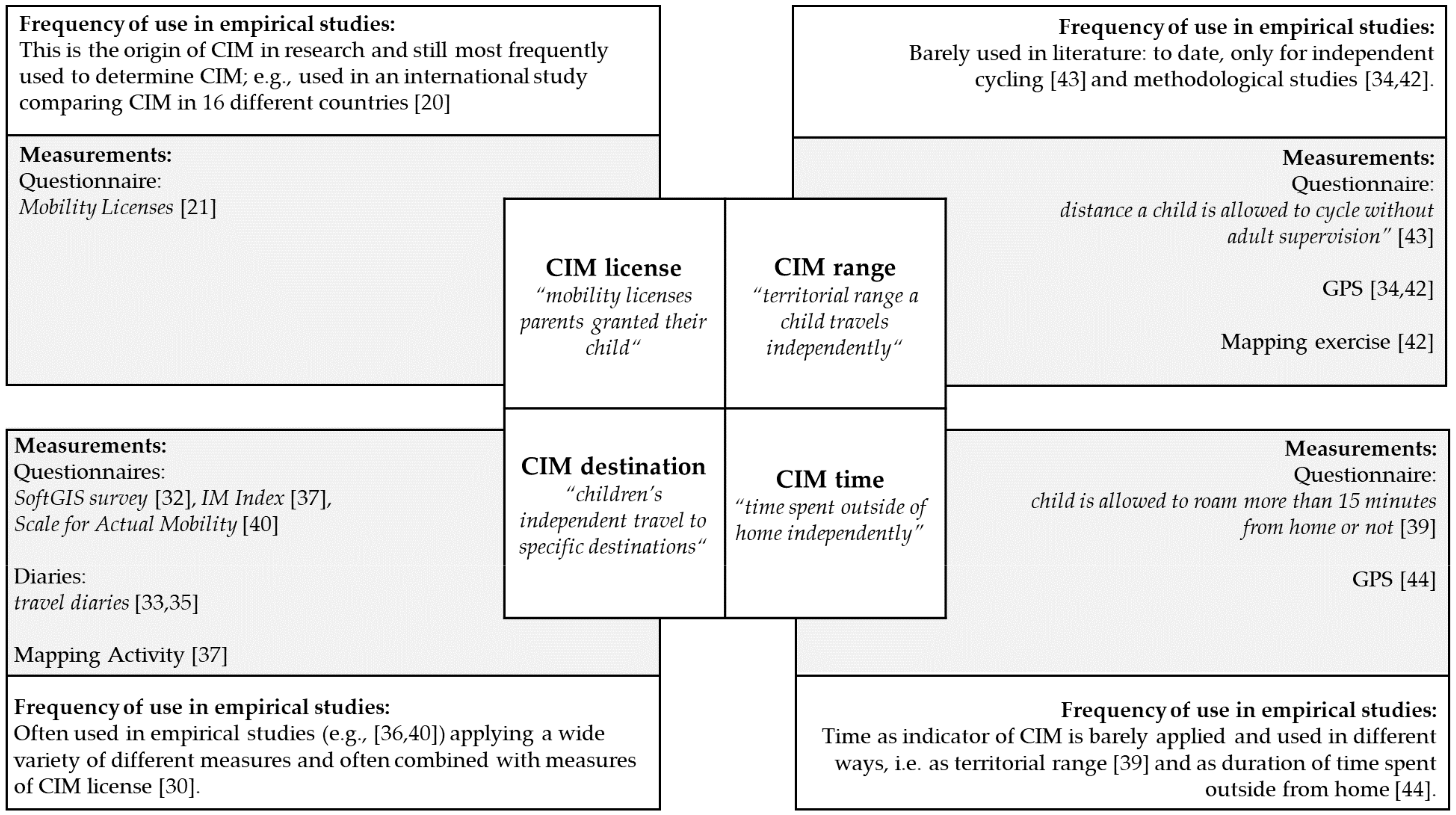
2.1. Indicators of CIM
2.2. Measurements of CIM and Their Application in Empirical Studies
3. Children’s Independent Mobility as Health-Related Behavior
4. Prevalence and Trends in Children’s Independent Mobility
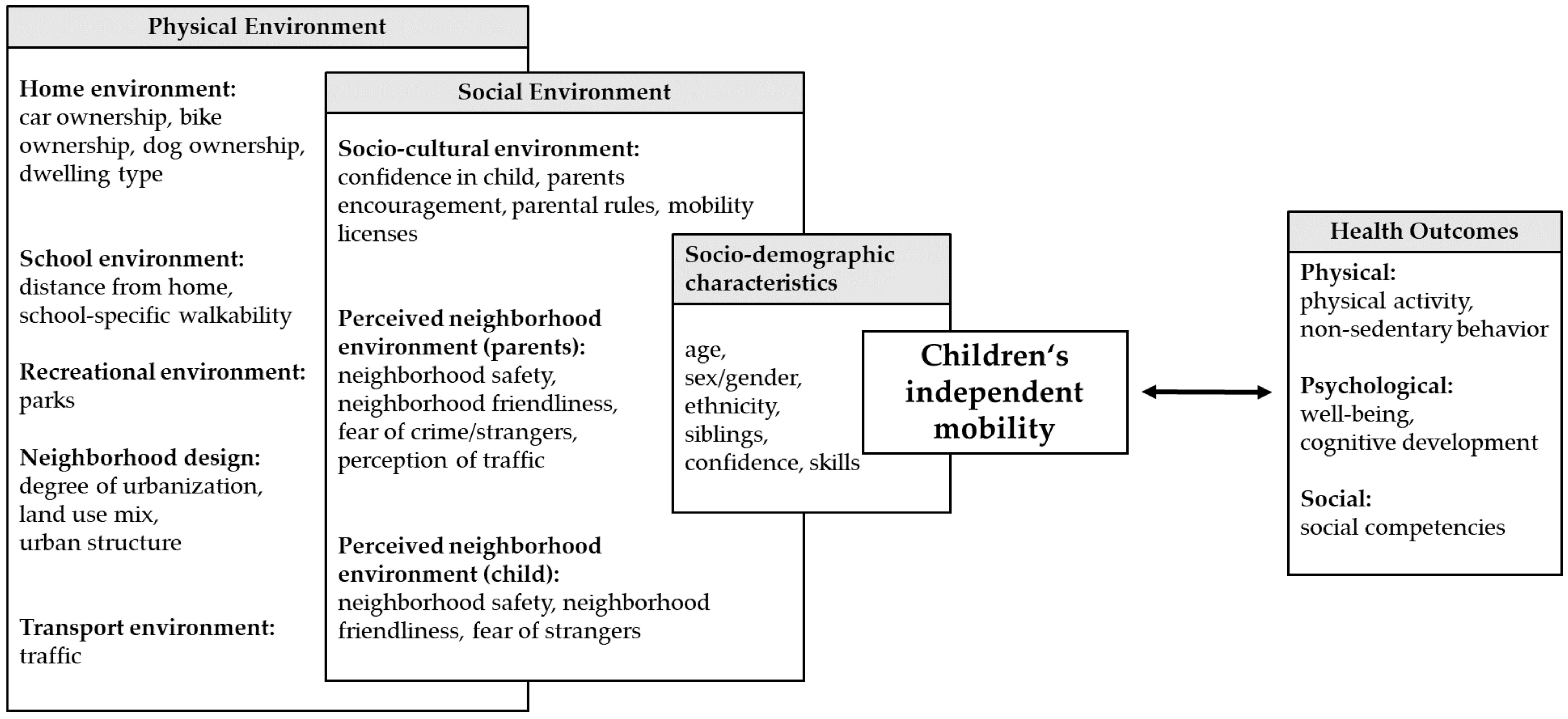
5. Socio-Ecological Correlates of Children’s Independent Mobility
6. Future Directions and Practical Implications
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Global Recommondation on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Schmidt, S.C.E.; Henn, A.; Albrecht, C.; Woll, A. Physical Activity of German Children and Adolescents 2003-2012: The MoMo-Study. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef]
- Cooper, A.R.; Andersen, L.B.; Wedderkopp, N.; Page, A.S.; Froberg, K. Physical activity levels of children who walk, cycle, or are driven to school. Am. J. Prev. Med. 2005, 29, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Marques, E.A.; Pizarro, A.I.; Mota, J.; Santos, M.P. Independent mobility and its relationship with moderate-to-vigorous physical activity in middle-school Portuguese boys and girls. J. Phys. Act. Health 2014, 11, 1640–1643. [Google Scholar] [CrossRef] [PubMed]
- Kyttä, M.; Hirvonen, J.; Rudner, J.; Pirjola, I.; Laatikainen, T. The last free-range children? Children’s independent mobility in Finland in the 1990s and 2010s. J. Transp. Geogr. 2015, 47, 1–12. [Google Scholar] [CrossRef]
- Shaw, B.; Watson, B.; Frauendienst, B.; Redecker, A.; Jones, T.; Hillman, M. Children’s Independent Mobility: A Comparative Study in England and Germany (1971–2010); Policy Studies Institute: London, UK, 2013. [Google Scholar]
- Schoeppe, S.; Tranter, P.; Duncan, M.J.; Curtis, C.; Carver, A.; Malone, K. Australian children’s independent mobility levels: Secondary analyses of cross-sectional data between 1991 and 2012. Child. Geogr. 2015, 14, 408–421. [Google Scholar] [CrossRef]
- Barker, J.; Kraftl, P.; Horton, J.; Tucker, F. The Road Less Travelled—New Directions in Children’s and Young People’s Mobility. Mobilities 2009, 4, 1–10. [Google Scholar] [CrossRef]
- Blinkert, B. Quality of the City for Children: Chaos and Order. Child. Youth Environ. 2004, 14, 99–112. [Google Scholar]
- Funk, W. Mobilität von Kinder und Jugendlichen. Langfristige Trends der Änderung Ihres Verkehrsverhaltens. Materialien aus dem Insitut für Empirische Soziologie an der Friedrich-Alexander-Universität Erlangen-Nürnberg; IfeS: Nürnberg, Germany, 2008. [Google Scholar]
- Fyhri, A.; Hjorthol, R.; Mackett, R.L.; Fotel, T.N.; Kyttä, M. Children’s active travel and independent mobility in four countries: Development, social contributing trends and measures. Transp. Policy 2011, 18, 703–710. [Google Scholar] [CrossRef]
- Francis, J.; Martin, K.; Wood, L.; Foster, S. ‘I’ll be driving you to school for the rest of your life’: A qualitative study of parents’ fear of stranger danger. J. Environ. Psychol. 2017, 53, 112–120. [Google Scholar] [CrossRef]
- Bennetts, S.K.; Cooklin, A.R.; Crawford, S.; D’Esposito, F.; Hackworth, N.J.; Green, J.; Matthews, J.; Strazdins, L.; Zubrick, S.R.; Nicholson, J.M. What Influences Parents’ Fear about Children’s Independent Mobility? Evidence from a State-Wide Survey of Australian Parents. Am. J. Health Promot. 2018, 32, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.B.; Bennetts, S.K.; Hackworth, N.J.; Green, J.; Graesser, H.; Cooldin, A.R.; Matthews, J.; Strazdins, L.; Zubrick, S.R.; D’Esposito, F.; et al. Worries, ‘weirdos’, neighborhoods and knowing people: A qualitative study with children and parents regarding children’s independent mobility. Health Place 2017, 45, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Fyhri, A.; Hjorthol, R. Children’s independent mobility to school, friends and leisure activities. J. Transp. Geogr. 2009, 17, 377–384. [Google Scholar] [CrossRef]
- Schmidt, W. Kindheit und Sportzugang im Wandel: Konsequenzen für die Bewegungsförderung. Sportunterricht 1993, 42, 24–32. [Google Scholar]
- Broberg, A.; Kyttä, M.; Fagerholm, N. Child-friendly urban structures: Bullerby revisited. J. Environ. Psychol. 2013, 35, 110–120. [Google Scholar] [CrossRef]
- Buliung, R.N.; Larsen, K.; Faulkner, G.; Ross, T. Children’s independent mobility in the City of Toronto, Canada. Travel Behav. Soc. 2017, 9, 58–69. [Google Scholar] [CrossRef]
- Shaw, B.; Bicket, M.; Elliott, B.; Fagan-Watson, B.; Mocca, E.; Hillman, M. Children’s Independent Mobility: An International Comparison and Recommendation for Action; Policy Studies Institute: London, UK, 2015. [Google Scholar]
- Hillman, M.; Adams, J.; Whitelegg, J. One False Move: A Study of Children’s Independent Mobility; Policy Studies Institute: London, UK, 1990. [Google Scholar]
- Tranter, P.; Whitelegg, J. Children’s travel behaviours in Canberra: Car dependent lifestyles in a low density city. J. Transp. Geogr. 1994, 4, 265–273. [Google Scholar] [CrossRef]
- Page, A.S.; Cooper, A.R.; Griew, P.; Davis, L.; Hillsdon, M. Independent mobility in relation to weekday and weekend physical activity in children aged 10–11 years: The PEACH Project. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Cordovil, R.; Lopes, F.; Neto, C. Children’s (in)dependent mobility in Portugal. J. Sci. Med. Sport 2015, 18, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Carver, A.; Panter, J.R.; Jones, A.P.; van Sluijs, E.M. Independent mobility on the journey to school: A joint cross-sectional and prospective exploration of social and physical environmental influences. J. Transp. Health 2014, 1, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Cervantes, L.; D’Haese, S.; Izquierdo-Gomez, R.; Padilla-Moledo, C.; Fernandez-Santos, J.R.; Cardon, G.; Veiga, O.L. Physical activity coparticipation and independent mobility as correlates of objectively measured nonschool physical activity in different school grades: The UP&DOWN study. J. Phys. Act. Health 2016, 13, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Duncan, M.J.; Badland, H.M.; Oliver, M.; Browne, M. Associations between children’s independent mobility and physical activity. BMC Public Health 2014, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Prezza, M.; Pilloni, S.; Morabito, C.; Sersante, C.; Alparone, F.R.; Giuliani, M.V. The influence of psychosocial and environmental factors on children’s independent mobility and relationship to peer frequentation. J. Community Appl. Soc. 2001, 11, 435–450. [Google Scholar] [CrossRef]
- Sharmin, S.; Kamruzzaman, M. Association between the built environment and children’s independent mobility: A meta-analytic review. J. Transp. Geogr. 2017, 61, 104–117. [Google Scholar] [CrossRef]
- Villanueva, K.; Giles-Corti, B.; Bulsara, M.; Trapp, G.; Timperio, A.; McCormack, G.; Van Niel, K. Does the walkability of neighbourhoods affect children’s independent mobility, independent of parental, socio-cultural and individual factors? Child. Geogr. 2014, 12, 393–411. [Google Scholar] [CrossRef]
- Larouche, R.; Eryuzlu, S.; Livock, H.; Leduc, G.; Faulkner, G.; Trudeau, F.; Tremblay, M.S. Test-retest reliability and convergent validity of measures of children’s travel behaviours and independent mobility. J. Transp. Health 2017, 6, 105–118. [Google Scholar] [CrossRef]
- Broberg, A.; Salminen, S.; Kyttä, M. Physical environmental characteristics promoting independent and active transport to children’s meaningful places. Appl. Geogr. 2013, 38, 43–52. [Google Scholar] [CrossRef]
- Oliver, M.; Witten, K.; Kearns, R.A.; Mavoa, S.; Badland, H.M.; Carroll, P.; Drumheller, C.; Tavae, N.; Asiasiga, L.; Jelley, S.; et al. Kids in the city study: Research design and methodology. BMC Public Health 2011, 11, 587. [Google Scholar] [CrossRef] [PubMed]
- Mavoa, S.; Oliver, M.; Witten, K.; Badland, H.M. Linking GPS and travel diary data using sequence alignment in a study of children’s independent mobility. Int. J. Health Geogr. 2011, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M. Environment and parental factors as determinants of mode for children’s leisure travel. J. Environ. Psychol. 2006, 26, 156–169. [Google Scholar] [CrossRef]
- Chaudhury, M.; Hinckson, E.; Badland, H.; Oliver, M. Children’s independence and affordances experienced in the context of public open spaces: A study of diverse inner-city and suburban neighbourhoods in Auckland, New Zealand. Child. Geogr. 2017, 1–15. [Google Scholar] [CrossRef]
- Villanueva, K.; Giles-Corti, B.; Bulsara, M.; Timperio, A.; McCormack, G.; Beesley, B.; Trapp, G.; Middleton, N. Where Do Children Travel to and What Local Opportunities Are Available? The Relationship between Neighborhood Destinations and Children’s Independent Mobility. Environ. Behav. 2012, 45, 679–705. [Google Scholar] [CrossRef]
- Christian, H.E.; Klinker, C.D.; Villanueva, K.; Knuiman, M.W.; Foster, S.A.; Zubrick, S.R.; Divitini, M.; Wood, L.; Giles-Corti, B. The Effect of the Social and Physical Environment on Children’s Independent Mobility to Neighborhood Destinations. J. Phys. Act. Health 2015, 12 (Suppl. 1), S84–S93. [Google Scholar] [CrossRef] [PubMed]
- Veitch, J.; Carver, A.; Hume, C.; Crawford, D.; Timperio, A.; Ball, K.; Salmon, J. Are independent mobility and territorial range associated with park visitation among youth? Int. J. Behav. Nutr. Phys. Act. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Kyttä, M. The extent of children’s independent mobility and the number of actualized affordances as criteria for child-friendly environments. J. Environ. Psychol. 2004, 24, 179–198. [Google Scholar] [CrossRef]
- Bates, B.; Stone, M.R. Measures of outdoor play and independent mobility in children and youth: A methodological review. J. Sci. Med. Sport 2015, 18, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Badland, H.M.; Oliver, M.; Duncan, M.J.; Schantz, P. Measuring children’s independent mobility: Comparing objective and self-report approaches. Child. Geogr. 2011, 9, 263–271. [Google Scholar] [CrossRef]
- Ghekiere, A.; Deforche, B.; Carver, A.; Mertens, L.; de Geus, B.; Clarys, P.; Cardon, G.; De Bourdeaudhuij, I.; Van Cauwenberg, J. Insights into children’s independent mobility for transportation cycling-Which socio-ecological factors matter? J. Sci. Med. Sport 2017, 20, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.; Parker, K.; Witten, K.; Mavoa, S.; Badland, H.M.; Donovan, P.; Chaudhury, M.; Kearns, R. Children’s Out-of-School Independently Mobile Trips, Active Travel, and Physical Activity: A Cross-Sectional Examination from the Kids in the City Study. J. Phys. Act. Health 2016, 13, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Alparone, F.R.; Pacilli, M.G. On children’s independent mobility: The interplay of demographic, environmental, and psychosocial factors. Child. Geogr. 2012, 10, 109–122. [Google Scholar] [CrossRef]
- Mikkelsen, M.R.; Christensen, P. Is Children’s Independent Mobility Really Independent? A Study of Children’s Mobility Combining Ethnography and GPS/Mobile Phone Technologies. Mobilities 2009, 4, 37–58. [Google Scholar] [CrossRef]
- Bhosale, J.; Duncan, S.; Stewart, T.; Chaix, B.; Kestens, Y.; Schofield, G. Measuring children’s independent mobility: Comparing interactive mapping with destination access and licence to roam. Child. Geogr. 2017, 15, 678–689. [Google Scholar] [CrossRef]
- Chaix, B.; Kestens, Y.; Perchoux, C.; Karusisi, N.; Merlo, J.; Labadi, K. An interactive mapping tool to assess individual mobility patterns in neighborhood studies. Am. J. Prev. Med. 2012, 43, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Duncan, M.J.; Badland, H.; Oliver, M.; Curtis, C. Associations of children’s independent mobility and active travel with physical activity, sedentary behaviour and weight status: A systematic review. J. Sci. Med. Sport 2013, 16, 312–319. [Google Scholar] [CrossRef] [PubMed]
- De Meester, F.; Van Dyck, D.; De Bourdeaudhuij, I.; Cardon, G. Parental perceived neighborhood attributes: Associations with active transport and physical activity among 10–12 year old children and the mediating role of independent mobility. BMC Public Health 2014, 14, 631. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.R.; Faulkner, G.E.J.; Mitra, R.; Buliung, R.N. The freedom to explore: Examining the influence of independent mobility on weekday, weekend and after-school physical activity behaviour in children living in urban and inner-suburban neighbourhoods of varying socioeconomic status. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Saunders, T.J.; Faulkner, G.; Colley, R.; Tremblay, M. Associations between active school transport and physical activity, body composition, and cardiovascular fitness: A systematic review of 68 studies. J. Phys. Act. Health 2014, 11, 206–227. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Gorber, S.C.; et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Viikari, J.; Valimaki, I.; Wanne, O.; Raitakari, O. Physical activity from childhood to adulthood: A 21-year tracking study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Rissotto, A.; Tonucci, F. Freedom of Movement and Environmental Knowledge in Elementary School Children. J. Environ. Psychol. 2002, 22, 65–77. [Google Scholar] [CrossRef]
- Mackett, R.; Brown, B.; Gong, Y.; Kitazawa, K.; Paskins, J. Children’s Independent Movement in the Local Environment. Built Environ. 2007, 33, 454–468. [Google Scholar] [CrossRef]
- Leung, K.Y.K.; Loo, B.P.Y. Association of children’s mobility and wellbeing: A case study in Hong Kong. Travel Behav. Soc. 2017, 9, 95–104. [Google Scholar] [CrossRef]
- Prezza, M.; Pacilli, M.G. Current fear of crime, sense of community and loneliness in Italian adolescents: The role of autonomous mobility and play during childhood. J. Community Psychol. 2007, 35, 151–170. [Google Scholar] [CrossRef]
- Ahmadi, E.; Taniguchi, G. Influential Factors on Children′s Spatial Knowledge and Mobility in Home–School Travel A Case Study in the City of Tehran. J. Asian Archit. Build. 2007, 6, 275–282. [Google Scholar] [CrossRef]
- Janssen, I. Hyper-parenting is negatively associated with physical activity among 7–12 year olds. Prev. Med. 2015, 73, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Mammen, G.; Faulkner, G. Physical activity and the prevention of depression: A systematic review of prospective studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.; Mackett, R.; Gong, Y.; Kitazawa, K.; Paskins, J. Gender differences in children’s pathways to independent mobility. Child. Geogr. 2008, 6, 385–401. [Google Scholar] [CrossRef]
- Bhosale, J.; Duncan, S.; Schofield, G. Intergenerational change in children’s independent mobility and active transport in New Zealand children and parents. J. Transp. Geogr. 2017, 7, 247–255. [Google Scholar] [CrossRef]
- Kok, G.; Gottlieb, N.H.; Commers, M.; Smerecnik, C. The ecological approach in health promotion programs: A decade later. Am. J. Health Promot. 2008, 22, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Golden, S.D.; Earp, J.A. Social ecological approaches to individuals and their contexts: Twenty years of health education & behavior health promotion interventions. Health Educ. Behav. 2012, 39, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological Models of Health Behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 4 ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; John Wiley & Sons: San Francisco, CA, USA, 2008; pp. 465–485. [Google Scholar]
- Janssen, I.; Ferrao, T.; King, N. Individual, family, and neighborhood correlates of independent mobility among 7 to 11-year-olds. Prev. Med. Rep. 2016, 3, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, M.K.; McDonald, N.C. Association between Neighborhood Social Environment and Children’s Independent Mobility. J. Phys. Act. Health 2016, 13, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Marzi, I.; Demetriou, Y.; Reimers, A.K. Social and physical environmental correlates of independent mobility in children: A systematic review taking sex/gender differences into account. Int. J. Health Geogr. 2018, 17, 24. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Sallis, J.F.; Dzewaltowski, D.A.; Owen, N. Toward a better understanding of the influences on physical activity: The role of determinants, correlates, causal variables, mediators, moderators, and confounders. Am. J. Prev. Med. 2002, 23, 5–14. [Google Scholar] [CrossRef]
- Qiu, L.; Zhu, X. Impact of Housing and Community Environment on Childern’s Independent Mobility: A Systematic Literature Review. Int. J. Contemp. Archit. New ARCH 2017, 4, 50–61. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- Mitra, R.; Faulkner, G.E.J.; Buliung, R.N.; Stone, M.R. Do parental perceptions of the neighbourhood environment influence children’s independent mobility? Evidence from Toronto, Canada. Urban Stud. 2014, 51, 3401–3419. [Google Scholar] [CrossRef]
- Tillberg Mattsson, K. Children’s (in)dependent mobility and parents’ chauffeuring in the town and the countryside. Tijdschr. Econ. Soc. Geogr. 2002, 93, 443–453. [Google Scholar] [CrossRef]
- Reimers, A.K.; Wagner, M.; Alvanides, S.; Steinmayr, A.; Reiner, M.; Schmidt, S.; Woll, A. Proximity to Sports Facilities and Sports Participation for Adolescents in Germany. PLoS ONE 2014, 9, e93059. [Google Scholar] [CrossRef] [PubMed]
- Prezza, M.; Alparone, F.R.; Renzi, D.; Pietrobono, A. Social participation and independent mobility in children: The effects of two implementations of “we go to school alone”. J. Prev. Interv. Community 2010, 38, 8–25. [Google Scholar] [CrossRef] [PubMed]
- Chillón, P.; Evenson, K.R.; Vaughn, A.; Ward, D.S. A systematic review of interventions for promoting active transportation to school. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Christian, H.E.; Villanueva, K.; Klinker, C.D.; Knuiman, M.W.; Divitini, M.; Giles-Corti, B. The effect of siblings and family dog ownership on children’s independent mobility to neighbourhood destinations. Aust. N. Z. J. Public Health 2016, 40, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Barkley, J.E.; Lepp, A.; Salehi-Esfahani, S. College Students’ Mobile Telephone Use Is Positively Associated With Sedentary Behavior. Am. J. Lifestyle Med. 2015, 10, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Country | 1971 (%) | 1990 (%) | 2010 (%) | Relative Differences in CIM (1990–2010) (%) |
|---|---|---|---|---|
| Germany 1 [7] | 93 | 76 | −18 | |
| England 1 [7] | 86 | 35 | 25 | −29 |
| Finland 2 [6] | 85 | 65 | −24 | |
| Australia 3 [8] | 68 | 31 | −54 | |
| New Zealand 4 [63] | 98 | 91 | −7 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marzi, I.; Reimers, A.K. Children’s Independent Mobility: Current Knowledge, Future Directions, and Public Health Implications. Int. J. Environ. Res. Public Health 2018, 15, 2441. https://doi.org/10.3390/ijerph15112441
Marzi I, Reimers AK. Children’s Independent Mobility: Current Knowledge, Future Directions, and Public Health Implications. International Journal of Environmental Research and Public Health. 2018; 15(11):2441. https://doi.org/10.3390/ijerph15112441
Chicago/Turabian StyleMarzi, Isabel, and Anne Kerstin Reimers. 2018. "Children’s Independent Mobility: Current Knowledge, Future Directions, and Public Health Implications" International Journal of Environmental Research and Public Health 15, no. 11: 2441. https://doi.org/10.3390/ijerph15112441
APA StyleMarzi, I., & Reimers, A. K. (2018). Children’s Independent Mobility: Current Knowledge, Future Directions, and Public Health Implications. International Journal of Environmental Research and Public Health, 15(11), 2441. https://doi.org/10.3390/ijerph15112441