Satisfaction of Physicians Working in Polish Hospitals—A Cross-Sectional Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Questionnaire
- 1.
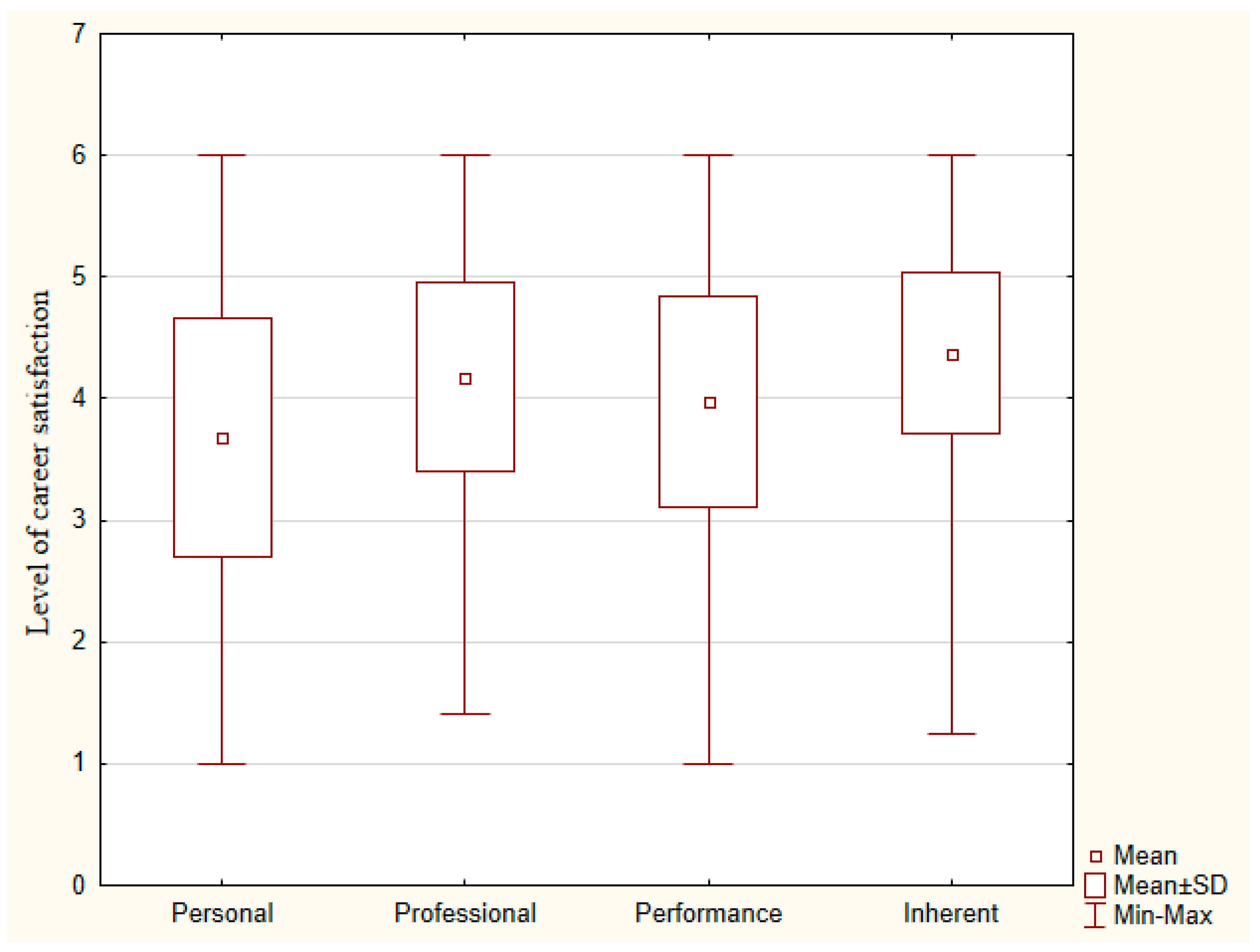
- Personal dimension (basic needs) refers to the abilities to keep work responsibilities separate from personal life, to sustain satisfying activities in the community, to control work schedule, and the way that the medical practice is managed [15].
- 2.
- Professional dimension (basic needs) refers to the physician’s relationship with administrators, nurses, level of remuneration, and the authority to have her/his clinical decisions carried out [15].
- 3.
- Performance dimension (high-order needs) refers to the ability to access resources to treat patients, success in meeting patients’ needs, capacity to keep up with medical advances, and her/his role in organizing programs for patients [15].
- 4.
- Inherent dimension (basic needs) refers to the doctor‒patient relationship, the diversity of patients that are seen, interaction with other physicians, and career advancement, which taps into the need for interesting and challenging work as a source of motivation [15].
2.3. Statistical Analysis
3. Results
3.1. Career Satisfaction of Physicians
3.2. Factors Associated with Higher Levels of Career Satisfaction
4. Discussion
4.1. Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Roelen, C.; Koopmans, P.; Groothoff, J. Which work factors determine job satisfaction? Work 2008, 30, 433–439. [Google Scholar] [PubMed]
- Wallace, J.E.; Lemaire, J.B.; Ghali, W.A. Physician wellness: A missing quality indicator. Lancet 2009, 374, 1714–1721. [Google Scholar] [CrossRef]
- Gyorffy, Z.; Girasek, E. Burnout among Hungarian physicians. Who are the most at risk? Orvosi Hetil. 2015, 156, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Escribà-Agüir, V.; Artazcoz, L.; Pérez-Hoyos, S. Effect of psychosocial work environment and job satisfaction on burnout syndrome among specialist physicians. Gac. Sanit. 2008, 22, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, M.W.; Chen, P.G.; Van Busum, K.R.; Aunon, F.; Pham, C.; Caloyeras, J.; Mattke, S.; Pitchforth, E.; Quigley, D.D.; Brook, R.H.; et al. Factors Affecting Physician Professional Satisfaction and Their Implications for Patient Care, Health Systems, and Health Policy. Rand Health Q. 2014, 3, 1. [Google Scholar] [PubMed]
- Van Beuzekom, M.; Akerboom, S.; Boer, F.; Dahan, A. Influence of latent risk factors on job satisfaction, job stress and intention to leave in anaesthesia teams: A cross-sectional survey. Eur. J. Anaesth. 2013, 30, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Scheepers, R.A.; Boerebach, B.C.; Arah, O.A.; Heineman, M.J.; Lombarts, K.M. A Systematic Review of the Impact of Physicians’ Occupational Well-Being on the Quality of Patient Care. Int. J. Behav. Med. 2015, 22, 683–698. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.; Skinner, A. Outcomes of physician job satisfaction: A narrative review, implications, and directions for future research. Health Care Manag. Rev. 2003, 28, 119–140. [Google Scholar] [CrossRef]
- Bovier, P.; Perneger, T. Predictors of work satisfaction among physicians. Eur. J. Public Health 2003, 13, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Workplace Health Promotion. A Special Issue of International Journal of Environmental Research and Public Health (ISSN 1660-4601). 2018. Available online: https://www.mdpi.com/journal/ijerph/special_issues/workplace_health (accessed on 12 November 2018).
- De Oliveira Vasconcelos, F.P.; De Souza, M.R.; Elias, P.E.; D’Ávila Viana, A.L. Physicians’ job satisfaction and motivation in a public academic hospital. Hum. Resour. Health 2016, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Emerging Issues in Occupational Safety and Health. A special issue of International Journal of Environmental Research and Public Health (ISSN 1660-4601). Available online: https://www.mdpi.com/journal/ijerph/special_issues/occupational_safety (accessed on 12 November 2018).
- McMurray, J.E.; Williams, E.; Schwartz, M.D.; Douglas, J.; Van Kirk, J.; Konrad, T.R.; Gerrity, M.; Bigby, J.A.; Linzer, M. Physician job satisfaction: Developing a model using qualitative data. SGIM Career Satisfaction Study Group. J. Gen. Intern Med. 1997, 12, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Maslow, A.H. Motivation and Personality; Harper & Row: New York, NY, USA, 1970. [Google Scholar]
- Lepnurm, R.; Danielson, D.; Dobson, R.; Keegan, D. Cornerstones of career satisfaction in medicine. Can. J. Psychiatry 2006, 51, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Peña-Sánchez, J.N.; Delgado, A.; Lucena-Muñoz, J.J.; Morales-Asencio, J.M. Adapting and Validating in Spanish the 4CornerSAT Questionnaire to Measure Career Satisfaction of Specialized care Physicians. Andalusia, Spain. Revista Espanola de Salud Publica 2013, 87, 181–189. [Google Scholar] [CrossRef] [PubMed]
- OECD Report 2017. Health at a Glance 2017: OECD Indicators; OECD Publishing: Paris, France, 2017; Available online: http://dx.doi.org/10.1787/health_glance-2017-en (accessed on 1 September 2018).
- Dubas-Jakóbczyk, K.; Domagała, A.; Mikos, M. Impact of the doctor deficit on hospital management in Poland: A mixed-method study. Int. J. Health Plan. Manag. 2018. [Google Scholar] [CrossRef] [PubMed]
- Domagała, A.; Klich, J. Planning of Polish physician workforce—Systemic inconsistencies, challenges and possible ways forward. Health Policy 2018, 122, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Statistical Bulletin. 2017. Available online: https://www.csioz.gov.pl/statystyka/biuletyn-statystyczny/www.csioz.gov.pl (accessed on 1 October 2018).
- Lewtak, K.; Poznańska, A.; Wysocki, M.J. Predyktory satysfakcji zawodowej lekarzy podstawowej opieki zdrowotnej. Problemy Higieny i Epidemiologii 2012, 93, 558–567. [Google Scholar]
- Putz, J. (Ed.) Analiza Satysfakcji Zawodowej Lekarzy Rodzinnych [w] Procesy przekształceń w ochronie Zdrowia—Bariery i Możliwości; Instytut Przedsiębiorczości i Samorządności: Warszawa, Poland, 2002. [Google Scholar]
- Gaszyńska, E.; Stankiewicz-Rudnicki, M.; Szatko, F.; Wieczorek, A.; Gaszyński, T. Life satisfaction and work-related satisfaction among anaesthesiologists in Poland. Sci. World J. 2014, 2014, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tobiasz-Adamczyk, B.; Brzyski, P. Bilans satysfakcji z pracy zawodowej lekarzy w wieku emerytalnym. Relacja pomiędzy satysfakcją z pracy zawodowej a ogólną jakością życia. Gerontologia Polska 2006, 14, 77–83. [Google Scholar]
- Tartas, M.; Walkiewicz, M.; Majkowicz, M.; Budzinski, W. Psychological factors determining success in a medical career: A 10-year longitudinal study. Med. Teach. 2011, 33, e163–e172. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D.A.; Christian, L.M.; Smyth, J.D. Internet, Phone, Mail, and Mixed-Mode Surveys: The Tailored Design Method, 4th ed.; ProQuest, & ProQuest Ebook Central, Wiley: Hoboken, NJ, USA, 2014. [Google Scholar]
- Price, J.H. Show me the money. Medical director’s responses to a mail survey. Am. J. Manag. Care 2000, 6, 1257–1259. [Google Scholar] [PubMed]
- VanGeest, J.B.; Johnson, T.P.; Welch, V.L. Methodologies for improving response rates in surveys of physicians: A systematic review. Eval. Health Prof. 2007, 30, 303–321. [Google Scholar] [CrossRef] [PubMed]
- Flanigan, T.S.; McFarlane, E.; Cook, S. Conducting survey research among physicians and other medical professionals: A review of current literature. ASA Proc. Sect. Surv. Res. Methods 2008, 36, 4136–4147. [Google Scholar]
- Lepnurm, R.; Dobson, R.; Backman, A.; Keegan, D. Factors explaining career satisfaction among psychiatrists and surgeons in Canada. Can. J. Psychiatry 2006, 51, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Peña-Sánchez, J.N.; Domagała, A.; Górkiewicz, M.; Targowska, M.; Oleszczyk, M. Adapting a tool in Poland for the measurement of the physicians’ career satisfaction. Problemy Medycyny Rodzinnej Family Medicine 2011, 12, 58–65. [Google Scholar]
- Peña-Sánchez, J.N.; Lepnurm, R.; Morales-Asencio, J.M.; Delgado, A.; Domagała, A.; Górkiewicz, M. Factors identified with higher levels of career satisfaction of physicians in Andalusia, Spain. Health Psychol. Res. 2014, 2, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Domagała, A.; Bała, M.M.; Peña-Sánchez, J.N.; Storman, D.; Świerz, M.; Kaczmarczyk, M.; Storman, M. Satisfaction of physicians working in hospitals within the European Union—State of the evidence based on systematic review. Eur. J. Public Health 2018. [Google Scholar] [CrossRef]
- National Chamber of Physicians (NCP). Doctor’s Opinions about Their Professional Job, Protests and Digitalization of Healthcare System. 2018. Available online: https://www.nil.org.pl/__data/assets/pdf_file/0006/128724/Opinie-o-pracy-zawodowej,-protescie-lekarzy-i-cyfryzacji-w-ochronie-zdrowia-raposrt-OSAI-NIL.pdf (accessed on 7 September 2018).
- National Chamber of Physicians (NCP). Short version of the report Doctor’s Opinions about Their Professional Job, Protests and Digitalization of Healthcare System. 2018. Available online: https://www.nil.org.pl/__data/assets/pdf_file/0019/129106/OSAI_sondaze-2018_raport_skrocony.pdf (accessed on 7 September 2018).
- Gyorffy, Z.; Girasek, E. Workload, work satisfaction and burnout among Hungarian female residents. Results of representative, online survey. Orvosi Hetil. 2014, 55, 1831–1840. [Google Scholar] [CrossRef] [PubMed]
- Healthgrouper. Special Report on Job Satisfaction of Doctors in Bulgaria. 2012. Available online: http://healthgrouper.com/documents/4417/Physicians-job-satisfaction-Bulgaria-2012.pdf (accessed on 7 September 2018). (In Bulgarian).
- Kairys, J.; Zebiene, E.; Sapoka, V.; Zokas, I. Satisfaction with organizational aspects of health care provision among Lithuanian physicians. Cent. Eur. J. Public Health 2008, 16, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Mrduljas-Dujic, N.; Kuzmanic, M.; Kardum, G.; Rumboldt, M. Job satisfaction among medical doctors in one of the countries in transition: Experience from Croatia. Coll. Antropol. 2010, 34, 813–818. [Google Scholar] [PubMed]
- Wendt, C. Mapping European healthcare systems: A comparative analysis of financing, service provision and access to healthcare. J. Eur. Soc. Policy 2009, 19, 432–445. [Google Scholar] [CrossRef]
- Janus, K.; Amelung, V.E.; Baker, L.C.; Gaitanides, M.; Schwartz, F.W.; Rundall, T.G. Job satisfaction and motivation among physicians in academic medical centers: Insights from a cross-national study. J. Health Politics Policy Law 2008, 33, 1133–1167. [Google Scholar] [CrossRef] [PubMed]
- Rosta, J.; Nylenna, M.; Aasland, O.G. Job satisfaction among hospital doctors in Norway and Germany. A comparative study on national samples. Scand. J. Public Health 2009, 37, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Groneberg, D.A. Distress among physicians in hospitals—An investigation in Baden-Wurttemberg, Germany. Deutsche Medizinische Wochenschrift 2013, 138, 2401–2406. [Google Scholar] [PubMed]
- Mache, S.; Vitzthum, K.; Klapp, B.F.; Groneberg, D.A. Improving quality of medical treatment and care: Are surgeons’ working conditions and job satisfaction associated to patient satisfaction? Langenbecks Arch. Surg. 2012, 397, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Ommen, O.; Driller, E.; Kohler, T.; Kowalski, C.; Ernstmann, N.; Neumann, M.; Steffen, P.; Pfaff, H. The relationship between social capital in hospitals and physician job satisfaction. BMC Health Serv. Res. 2009, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Mache, S.; Vitzthum, K.; Nienhaus, A.; Klapp, B.F.; Groneberg, D.A. Physicians’ working conditions and job satisfaction: Does hospital ownership in Germany make a difference? BMC Health Serv. Res. 2009, 9, 148. [Google Scholar] [CrossRef] [PubMed]
- Mascia, D.; Morandi, F.; Cicchetti, A. Hospital restructuring and physician job satisfaction: An empirical study. Health Policy 2014, 114, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Michinov, E.; Olivier-Chiron, E.; Rusch, E.; Chiron, B. Influence of transactive memory on perceived performance, job satisfaction and identification in anaesthesia teams. Br. J. Anaesth. 2008, 100, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Schmit Jongbloed, L.J.; Schönrock-Adema, J.; Borleffs, J.C.; Stewart, R.E.; Cohen-Schotanus, J. The influence of achievement before, during and after medical school on physician job satisfaction. Adv. Health Sci. Educ. Theory Pract. 2014, 19, 581–595. [Google Scholar] [CrossRef] [PubMed]
- Domagała, A.; Bała, M.M.; Storman, D.; Peña-Sánchez, J.N.; Świerz, M.; Kaczmarczyk, M.; Storman, M. Factors associated with satisfaction of hospital physicians: A systematic review on European data. Int. J. Environ. Res. Public Health 2018, 15, 2546. [Google Scholar] [CrossRef] [PubMed]
- Aalto, A.M.; Heponiemi, T.; Vaananen, A.; Bergbom, B.; Sinervo, T.; Elovainio, M. Is working in culturally diverse working environment associated with physicians’ work-related well-being? A cross-sectional survey study among Finnish physicians. Health Policy 2014, 17, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N. Is there a gender gap in Italian radiology? A cross-sectional study. Eur. J. Radiol. 2013, 82, e502–e507. [Google Scholar] [CrossRef] [PubMed]
- Heponiemi, T.; Aalto, A.M.; Puttonen, S.; Vänskä, J.; Elovainio, M. Work-related stress, job resources, and well-being among psychiatrists and other medical specialists in Finland. Psychiatr. Serv. 2014, 65, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.R.M.; Smets, E.M.A.; Oort, F.J.; de Haes, H.C.J. Stress, satisfaction and burnout among Dutch medical specialists. CMAJ Can. Med. Assoc. J. 2003, 68, 271–275. [Google Scholar]
- Kellerman, S.E.; Herold, J. Physician response to surveys. A review of the literature. Am J Prev Med. 2001, 20, 61–67. [Google Scholar] [CrossRef]
- Pedrazza, M.; Berlanda, S.; Trifiletti, E.; Bressan, F. Exploring physicians’ dissatisfaction and work-related stress: Development of the PhyDis Scale. Front. Psychol. 2016, 7, 1238. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, R.L. Physician job satisfaction as a public health issue. Isr. J. Health Policy Res. 2015, 1, 51. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Type of Hospital | |||||
|---|---|---|---|---|---|
| General | Specialist | University | |||
| Variable | n = 282 | n = 325 | n = 396 | ALL (n = 1.003) | p Value |
| Age, years, mean (SD) | 46.6 (10.84) | 41.9 (11.80) | 42.34 (11.96) | 43.4 (11.76) | <0.001 A |
| Female, n (%) | 137 (49%) | 159 (49%) | 189 (48%) | 485 (48%) | 0.95 B |
| Marital status (in a relationship), n (%) | 213 (76%) | 242 (74%) | 306 (77%) | 761 (76%) | 0.67 B |
| Have children, n (%) | 208 (74%) | 208 (64%) | 264 (67%) | 680 (68%) | 0.03 B |
| Specialist, n (%) | 230 (82%) | 190 (58%) | 259 (65%) | 679 (68%) | <0.001 B |
| Work experience, years, median (q1–q3) | 20.5 (10–28) | 12 (5–27) | 15 (6–26) | 15 (6–27) | <0.001 C |
| Additional shift-work duties, n (%) | 228 (81%) | 262 (81%) | 285 (72%) | 775 (77%) | 0.005 B |
| Number of working hours in hospital per week, mean (SD) | 46.5 (19.11) | 50.7 (13.61) | 45.0 (14.5) | 47.3 (15.86) | <0.001 A |
| Total number of working hours per week, mean (SD) | 63.7 (16.06) | 62.4 (15.44) | 56.0 (17.86) | 60.3 (16.94) | <0.001 A |
| Type of employment, n (%) | |||||
| Job agreement | 112 (40.2%) | 240 (74.3%) | 310 (78.5%) | 662 (66.3%) | |
| Contract | 146 (52.3%) | 54 (16.7%) | 72 (18.2%) | 272 (27.3%) | <0.001 A |
| Mix | 21 (7.5%) | 29 (8.9%) | 13 (3.3%) | 63 (6.4%) | |
| n (%) | Personal | Professional | Performance | Inherent | Overall | |
|---|---|---|---|---|---|---|
| Type of Hospital | ||||||
| General | 282 (28.1) | 3.7 (0.91) | 4.3 (0.65) ** | 3.9 (0.81) * | 4.3 (0.6) | 4.1 (0.60) * |
| Specialist | 325 (32.4) | 3.7 (0.93) | 4.3 (0.77) ** | 4.1 (0.87) * | 4.4 (0.66) | 4.1 (0.69) * |
| University | 396 (39.5) | 3.6 (1.07) | 4.0 (0.81) ** | 4.0 (0.88) * | 4.4 (0.71) | 4.0 (0.74) * |
| Hospital Category | ||||||
| Public | 834 (83.2) | 3.7 (1) | 4.1 (0.8) * | 4 (0.87) * | 4.4 (0.68) | 4.1 (0.71) |
| Private | 169 (16.8) | 3.7 (0.93) | 4.4 (0.61) * | 3.8 (0.82) * | 4.3 (0.57) | 4.1 (0.58) |
| Total | 1003 (100) | 3.7 (0.98) | 4.2 (0.77) | 4.0 (0.86) | 4.4 (0.66) | 4.1 (0.67) |
| Personal Dimension | Professional Dimension | Performance Dimension | Inherent Dimension | Overall Satisfaction | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | AOR 95% CI | OR (95% CI) | AOR 95% CI | OR (95% CI) | AOR 95% CI | OR (95% CI) | AOR 95% CI | OR (95% CI) | AOR 95% CI | |
| Type of Hospital | ||||||||||
| General (ref.) | 1 | 1 | 1 | 1 | 1 | 1 | ||||
| Specialist | 1.27 (0.76–2.13) | 1.32 (0.88–1.99) | 1.71 (1.08–2.71) | 1.63 (1.02–2.59) | 1.59 (1.01–2.55) | 1.14 (0.77–1.69) | 2.02 (1.05–3.88) | 3.06 (1.49–6.3) | ||
| University | 1.49 (0.92–2.42) | 0.72 (0.47–1.11) | 0.78 (0.48–1.26) | 1.15 (0.72–1.84) | 0.9 (0.55–1.47) | 1.41 (0.97–2.03) | 1.97 (1.04–3.73) | 2.15 (1.06–4.36) | ||
| Gender | ||||||||||
| Male (ref) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |||
| Female | 0.64 (0.43–0.94) | 0.48 (0.32–0.74) | 0.46 (0.32–0.65) | 0.43 (0.29–0.62) | 0.68 (0.48–0.99) | 0.53 (0.36–0.78) | 0.58 (0.43–0.78) | 0.5 (0.36–0.69) | 0.39 (0.24–0.64) | 0.27 (0.16–0.48) |
| Work Experience (years) | 1.02 (1.01–1.04) | 1.03 (1.02–1.05) | 1.02 (1.01–1.04) | 1.01 (0.99–1.02) | 1.02 (1.001–1.03) | 1.03 (1.01–1.05) | ||||
| Marital Status | ||||||||||
| Single (ref.) | 1 | 1 | 1 | 1 | 1 | |||||
| In relationships | 0.95 (0.6–1.49) | 1.52 (0.99–2.33) | 0.90 (0.59–1.35) | 1.27 (0.89–1.80) | 1.24 (0.71–2.16) | |||||
| Having children | ||||||||||
| No (ref) | 1 | 1 | 1 | 1 | 1 | |||||
| Yes | 0.88 (0.59–1.31) | 1.53 (1.05–2.25) | 0.92 (0.63–1.35) | 1.15 (0.83–1.58) | 1.32 (0.8–2.2) | |||||
| Additional work-shift duties | ||||||||||
| No (ref) | 1 | 1 | 1 | 1 | 1 | |||||
| Yes | 0.62 (0.41–0.94) | 1.02 (0.69–1.52) | 1.03 (0.67–1.58) | 1.15 (0.8–1.64) | 0.73 (0.44–1.22) | |||||
| Stage of professional development | ||||||||||
| Before spec. (ref) | 1 | 1 | 1 | 1 | 1 | 1 | ||||
| Specialist | 1.3 (0.86–1.98) | 1.88 (1.26–2.79) | 1.04 (0.69–1.55) | 1.56 (1.12–2.17) | 1.54 (1.1–2.18) | 1.91 (1.1–3.32) | ||||
| Working hours per week | 0.97 (0.96–0.98) | 0.96 (0.95–0.98) | 0.99 (0.98–1.00) | 0.98 (0.97–0.99) | 0.98 (0.97–0.99) | 0.98 (0.97–0.99) | 0.99 (0.98–0.999) | 0.98 (0.97–0.99) | 0.98 (0.96–0.99) | 0.97 (0.95–0.98) |
| Type of employment form | ||||||||||
| Job agreement (ref.) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| Contract | 1.52 (1.01–2.28) | 1.82 (1.18–2.81) | 1.87 (1.31–2.67) | 1.64 (1.08–2.49) | 1.10 (0.73–1.64) | 1.07 (0.77–1.48) | 2.01 (1.25–3.22) | 2.94 (1.7–5.09) | ||
| Mix | 0.85 (0.35–2.04) | 1.36 (0.55–3.37) | 1.03 (0.49–2.17) | 1.19 (0.55–2.58) | 0.79 (0.35–1.8) | 0.86 (0.46–1.64) | 0.7 (0.21–2.33) | 1.11 (0.32–3.83) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domagała, A.; Peña-Sánchez, J.N.; Dubas-Jakóbczyk, K. Satisfaction of Physicians Working in Polish Hospitals—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 2640. https://doi.org/10.3390/ijerph15122640
Domagała A, Peña-Sánchez JN, Dubas-Jakóbczyk K. Satisfaction of Physicians Working in Polish Hospitals—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2018; 15(12):2640. https://doi.org/10.3390/ijerph15122640
Chicago/Turabian StyleDomagała, Alicja, Juan Nicolás Peña-Sánchez, and Katarzyna Dubas-Jakóbczyk. 2018. "Satisfaction of Physicians Working in Polish Hospitals—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 15, no. 12: 2640. https://doi.org/10.3390/ijerph15122640
APA StyleDomagała, A., Peña-Sánchez, J. N., & Dubas-Jakóbczyk, K. (2018). Satisfaction of Physicians Working in Polish Hospitals—A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 15(12), 2640. https://doi.org/10.3390/ijerph15122640