Inmates with Harmful Substance Use Increase Both Exercise and Nicotine Use Under Incarceration

 ,
,
Abstract
:1. Introduction
- What is the prevalence of exercise and nicotine use among inmates with and without harmful substance use?
- How do exercise and nicotine use change over time?
- Which variables, including individual and system-related, are associated with increased exercise frequency during incarceration?
2. Materials and Methods
2.1. Setting
2.2. Study Design
2.3. Measures
2.3.1. Six-Month Pre-Incarceration Variables
2.3.2. During Incarceration Variables
2.4. Analysis
3. Results
3.1. Sample Description
3.2. Prevalence of Exercise and Nicotine Use
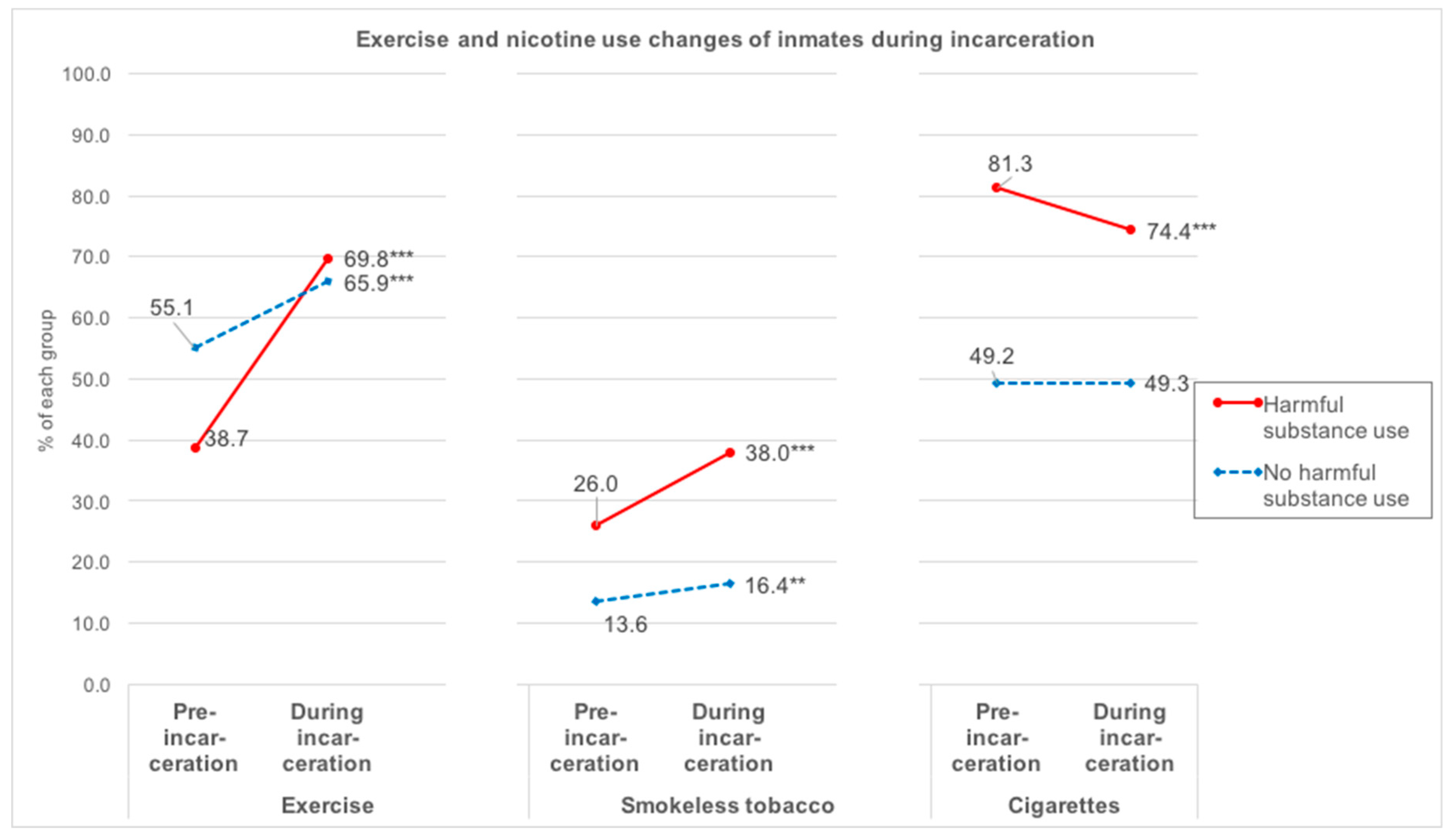
3.3. Changes in Exercise and Nicotine Use during Incarceration
3.4. Factors Related to Increased Exercise Frequency
4. Discussion
4.1. Limitations and Strengths
4.2. Clinical Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| NorMA | Norwegian Offender Mental Health and Addiction Study |
| AUDIT | Alcohol Use Disorders Identification Test |
| DUDIT | Drug Use Disorders Identification Test |
| SCL10 | Hopkins Symptom Checklist 10 |
| OMT | Opioid Maintenance Treatment |
References
- Caspersen, C.; Powell, K.; Christenson, G. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- World Health Organization. F10—F19: Mental and Behavioural Disorders Due to Psychoactive Substance Use; WHO: Geneva, Switzerland, 1992. [Google Scholar]
- Wang, D.; Wang, Y.; Wang, Y.; Li, R.; Zhou, C. Impact of physical exercise on substance use disorders: A meta-analysis. PLoS ONE 2014, 9, e110728. [Google Scholar] [CrossRef] [PubMed]
- Linke, S.E.; Ussher, M. Exercise-based treatments for substance use disorders: Evidence, theory, and practicality. Am. J. Drug Alcohol Abus. 2015, 41, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Zschucke, E.; Heinz, A.; Strohle, A. Exercise and physical activity in the therapy of substance use disorders. Sci. World J. 2012. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, J.; Wadeson, H.K.; VanHeest, J.L. Exercise as an adjunct treatment for opiate agonist treatment: Review of the current research and implementation strategies. Subst Abus. 2012, 33, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Correia, C.J.; Benson, T.A.; Carey, K.B. Decreased substance use following increases in alternative behaviors: A preliminary investigation. Addict. Behav. 2005, 30, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Simonton, A.J.; Young, C.C.; Brown, R.A. Physical Activity Preferences and Attitudes of Individuals with Substance Use Disorders: A Review of the Literature. Issues Ment. Health Nurs. 2018, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Directorate of Health. Fysisk aktivitet og psykisk helse—Et tipshefte for helsepersonell om tilrettelegging og planlegging av fysisk aktivitet for mennesker med psykiske lidelser og problemer. In Tipshefte; Directorate of Health, Ed.; Directorate of Health: Oslo, Norway, 2010; p. 16. [Google Scholar]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [PubMed]
- Thylstrup, B.; Clausen, T.; Hesse, M. Cardiovascular disease among people with drug use disorders. Int. J. Public Health 2015, 60, 659–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clausen, T.; Waal, H.; Thoresen, M.; Gossop, M. Mortality among opiate users: Opioid maintenance therapy, age and causes of death. Addiction 2009, 104, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.; Li, L.; Min, J.; Huang, D.; Urada, D.; Liu, L.; Hser, Y.I.; Nosyk, B. Mortality among individuals accessing pharmacological treatment for opioid dependence in California, 2006–2010. Addiction 2015, 110, 996–1005. [Google Scholar] [CrossRef] [PubMed]
- Chesher, N.J.; Bousman, C.A.; Gale, M.; Norman, S.B.; Twamley, E.W.; Heaton, R.K.; Everall, I.P.; Judd, P.A. Chronic illness histories of adults entering treatment for co-occurring substance abuse and other mental health disorders. Am. J. Addict. 2012, 21, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Caviness, C.M.; Bird, J.L.; Anderson, B.J.; Abrantes, A.M.; Stein, M.D. Minimum recommended physical activity, and perceived barriers and benefits of exercise in methadone maintained persons. J. Subst. Abus. Treat. 2013, 44, 457–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, A.; Skurtveit, S.; Clausen, T. Many correlates of poor quality of life among substance users entering treatment are not addiction-specific. Health Qual. Life Outcomes 2016, 14, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lester, C.; Hamilton-Kirkwood, L.; Jones, N.K. Health indicators in a prison population: Asking prisoners. Health Educ. J. 2003, 62, 341–349. [Google Scholar] [CrossRef]
- Fischer, J.; Butt, C.; Dawes, H.; Foster, C.; Neale, J.; Plugge, E.; Wheeler, C.; Wright, N. Fitness levels and physical activity among class A drug users entering prison. Br. J. Sports Med. 2012, 46, 1142–1144. [Google Scholar] [CrossRef] [PubMed]
- Fazel, S.; Yoon, I.A.; Hayes, A.J. Substance use disorders in prisoners: An updated systematic review and meta-regression analysis in recently incarcerated men and women. Addiction 2017, 112, 1725–1739. [Google Scholar] [CrossRef] [PubMed]
- Buckaloo, B.J.; Krug, K.S.; Nelson, K.B. Exercise and the Low-Security Inmate:Changes in Depression, Stress, and Anxiety. Prison. J. 2009, 89, 328–343. [Google Scholar] [CrossRef]
- Cooper, C.; Berwick, S. Factors affecting psychological well-being of three groups of suicide-prone prisoners. Curr. Psychol. 2001, 20, 169–182. [Google Scholar] [CrossRef]
- Martos-García, D.; Devís-Devís, J.; Sparkes, A.C. Sport and physical activity in a high security Spanish prison: An ethnographic study of multiple meanings. Sport Educ. Soc. 2009, 14, 77–96. [Google Scholar] [CrossRef]
- Firth, C.L.; Drach, L.; Maher, J.E.; Peters, C.S. Lack of Healthier Food Alternatives Can Compromise Inmate Health. Am. J. Public Health 2015, 105, e4–e5. [Google Scholar] [CrossRef] [PubMed]
- Fazel, S.; Baillargeon, J. The health of prisoners. Lancet 2010, 377, 956–965. [Google Scholar] [CrossRef]
- Sari, S.; Muller, A.E.; Roessler, K.K. Exercising alcohol patients don’t lack motivation but struggle with structures, emotions and social context—A qualitative dropout study. BMC Fam. Pract. 2017, 18, 45. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, C.; di Cagno, A.; Fiorilli, G.; Giombini, A.; Fagnani, F.; Borrione, P.; Marchetti, M.; Pigozzi, F. Benefits of selected physical exercise programs in detention: A randomized controlled study. Int. J. Environ. Res. Public Health 2013, 10, 5683–5696. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.; Specian, V.L.; Tracy, N.C.; DeMello, J.J. The Effects of Moderate Physical Activity on Offenders in a Rehabilitative Program. J. Correct. Educ. 2006, 57, 276–285. [Google Scholar]
- Cashin, A.; Potter, E.; Stevens, W.; Davidson, K.; Muldoon, D. Fit for prison: Special population health and fitness programme evaluation. Int. J. Prison. Health 2008, 4, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Perez-Moreno, F.; Camara-Sanchez, M.; Tremblay, J.F.; Riera-Rubio, V.J.; Gil-Paisan, L.; Lucia, A. Benefits of exercise training in Spanish prison inmates. Int. J. Sports Med. 2007, 28, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, C.; di Cagno, A.; Fiorilli, G.; Giombini, A.; Borrione, P.; Baralla, F.; Marchetti, M.; Pigozzi, F. Participation in a 9-month selected physical exercise programme enhances psychological well-being in a prison population. Crim. Behav. Ment. Health CBMH 2015, 25, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Genovese, J.; Libbus, M.; Poole, M. Organized Aerobic Exercise and Depression in Male County Jail Inmates. J. Correct. Health Care 1995, 2, 5–16. [Google Scholar] [CrossRef]
- Wagner, M.; McBride, R.; Crouse, S. The effects of weight-training exercise on aggression variables in adult male inmates. Prison. J. 1999, 79. [Google Scholar] [CrossRef]
- Olaitan, S.A.; Shmaila, H.; Sikiru, L.; Lawal, I.U. Correlates of Selected Indices of Physical Fitness And Duration of Incarceration among Inmates in Some Selected Nigeria Prisons. Ethiop. J. Health Sci. 2010, 20, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Mannocci, A.; Mipatrini, D.; D’Egidio, V.; Rizzo, J.; Meggiolaro, S.; Firenze, A.; Boccia, G.; Santangelo, O.E.; Villari, P.; La Torre, G.; et al. Health related quality of life and physical activity in prison: A multicenter observational study in Italy. Eur. J. Public Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, M.K.; Nianogo, R.A.; Arah, O.A. Weight gain during incarceration: Systematic review and meta-analysis. Obes. Rev. 2018, 19, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Herbert, K.; Plugge, E.; Foster, C.; Doll, H. Prevalence of risk factors for non-communicable diseases in prison populations worldwide: A systematic review. Lancet 2012, 379, 1975–1982. [Google Scholar] [CrossRef]
- Spaulding, A.C.; Eldridge, G.D.; Chico, C.E.; Morisseau, N.; Drobeniuc, A.; Fils-Aime, R.; Day, C.; Hopkins, R.; Jin, X.; Chen, J.; et al. Smoking in Correctional Settings Worldwide: Prevalence, Bans, and Interventions. Epidemiol. Rev. 2018, 40, 82–95. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, J.J.; Bock, B.; Roberts, M.B.; Stein, L.A.; Friedmann, P.D.; Martin, S.A.; Clarke, J.G. Cigarette smoking as an expression of independence and freedom among inmates in a tobacco-free prison in the United States. Nicotine Tob. Res. 2014, 16, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Bukten, A.; Riksheim, M.; Skurtveit, S.; Kunøe, N.; Lobmaier, P.; Lund, I.O.; Clausen, T. Substance Use and Health Status Among Incarcerated Individuals in Norway: Results from the Norwegian Offender Mental Health and Addiction Study; University of Oslo: Oslo, Norway, 2016. [Google Scholar]
- ICPR. International Centre of Prison Studies. Available online: http://www.prisonstudies.org/ (accessed on 5 February 2018).
- NCS. About the Norwegian Correctional Service. Available online: http://www.kriminalomsorgen.no/information-in-english.265199.no.html (accessed on 7 February 2018).
- Dore, G. Health-Related Quality of Life in Prisoners. In Handbook of Disease Burdens and Quality of Life Measures; Preedy, V.R., Watson, R.R., Eds.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Kristoffersen, R. Relapse Study in the Correctional Services of the Nordic Countries: Key Results and Perspectives. EuroVista 2013, 2, 9. [Google Scholar]
- Cramer, V. The Prevalence of Mental Disorders among Convicted Inmates in Norwegian Prisons; Southeastern Regional Health Authority: Oslo, Norway, 2014.
- Friestad, C.; Hansen, I.L.S. Levekår Blant Innsatte (Living Condtions among Inmates); Fafo Institute for Labour and Social Research: Oslo, Norway, 2014. [Google Scholar]
- Nesset, M.B.; Rustad, A.B.; Kjelsberg, E.; Almvik, R.; Bjorngaard, J.H. Health care help seeking behaviour among prisoners in Norway. BMC Health Serv. Res. 2011, 11, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bukten, A.; Lund, I.O.; Rognli, E.B.; Stavseth, M.R.; Lobmaier, P.; Skurtveit, S.; Clausen, T.; Kunoe, N. The Norwegian Offender Mental Health and Addiction Study—Design and Implementation of a National Survey and Prospective Cohort Study. Subst. Abus. 2015, 9, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Health Care, 2nd ed.; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- ROP. Guide for Beregning av Poengsum AUDIT (“AUDIT Scoring Instructions”). Available online: https://rop.no/globalassets/snakkomrus/utskrifter/audit/audit-scoringsguide.pdf (accessed on 11 June 2018).
- Berman, A.H.; Palmstierna, T.; Kallmen, H.; Bergman, H. The self-report Drug Use Disorders Identification Test: Extended (DUDIT-E): Reliability, validity, and motivational index. J. Subst. Abus. Treat. 2007, 32, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, G.; Hawthorne, G.; Elliott, P. Imputing cross-sectional missing data: Comparison of common techniques. Aust. N. Z. J. Psychiatry 2005, 39, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Lipman, R.S.; Rickels, K.; Uhlenhuth, E.H.; Covi, L. Hopkins Symptom Checklist (HSCL): A self report symptom inventory. Behav. Sci. 1974, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Strand, B.H.; Dalgard, O.S.; Tambs, K.; Rognerud, M. Measuring the mental health status of the Norwegian population: A comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nord. J. Psychiatry 2003, 57, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Natvig Norderhaug, I.; Dybing, E.; Gilljam, H.; Lind, P.O.; Lund, K.E.; Morland, J.; Stegmayr, B.; Hofmann, B.; Orjasaeter Elvsaas, I.K. NIPH Systematic Reviews: Executive Summaries. In Health Effects and Dependency Associated with Snuff Consumption; Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH): Oslo, Norway, 2005. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Bardo, M.T.; Compton, W.M. Does physical activity protect against drug abuse vulnerability? Drug Alcohol Depend. 2015, 153, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Lynch, W.J.; Peterson, A.B.; Sanchez, V.; Abel, J.; Smith, M.A. Exercise as a novel treatment for drug addiction: A neurobiological and stage-dependent hypothesis. Neurosci. Biobehav. Rev. 2013, 37, 1622–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, A.; Clausen, T. Group exercise to improve quality of life among substance use disorder patients. Scand. J. Public Health 2015, 43, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Midlöv, P.; Leijon, M.; Sundquist, J.; Sundquist, K.; Johansson, S.-E. The longitudinal exercise trend among older Swedes aged 53–84 years—A 16-year follow-up study. BMC Public Health 2014, 14, 1327. [Google Scholar] [CrossRef] [PubMed]
- Brenowitz, W.D.; Hubbard, R.A.; Crane, P.K.; Gray, S.L.; Zaslavsky, O.; Larson, E.B. Longitudinal associations between self-rated health and performance-based physical function in a population-based cohort of older adults. PLoS ONE 2014, 9, e111761. [Google Scholar] [CrossRef] [PubMed]
- De Viggiani, N. A new approach to prison public health? Challenging and advancing the agenda for prison health. Crit. Public Health 2006, 16, 307–316. [Google Scholar] [CrossRef]
- Gordon, B.R.; McDowell, C.P.; Hallgren, M.; Meyer, J.D.; Lyons, M.; Herring, M.P. Association of Efficacy of Resistance Exercise Training With Depressive Symptoms: Meta-analysis and Meta-regression Analysis of Randomized Clinical Trials. JAMA Psychiatry 2018, 75, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Berg, J.J.; Roberts, M.B.; Bock, B.C.; Martin, R.A.; Stein, L.A.; Parker, D.R.; McGovern, A.R.; Shuford, S.H.; Clarke, J.G. Changes in Depression and Stress after Release from a Tobacco-Free Prison in the United States. Int. J. Environ. Res. Public Health 2016, 13, 114. [Google Scholar] [CrossRef] [PubMed]
- Meek, R.; Lewis, G. The role of sport in promoting prisoner health. Int. J. Prison. Health 2012, 8, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Pope, H.G., Jr.; Kanayama, G.; Athey, A.; Ryan, E.; Hudson, J.I.; Baggish, A. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: Current best estimates. Am. J. Addict. 2014, 23, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Garner, O.; Iardino, A.; Ramirez, A.; Yakoby, M. Cardiomyopathy induced by anabolic-androgenic steroid abuse. BMJ Case Rep. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Baggish, A.L.; Weiner, R.B.; Kanayama, G.; Hudson, J.I.; Lu, M.T.; Hoffmann, U.; Pope, H.G., Jr. Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use. Circulation 2017, 135, 1991–2002. [Google Scholar] [CrossRef] [PubMed]
- Smit, D.L.; de Ronde, W. Outpatient clinic for users of anabolic androgenic steroids: An overview. Neth. J. Med. 2018, 76, 167. [Google Scholar] [PubMed]
- Lundholm, L.; Kall, K.; Wallin, S.; Thiblin, I. Use of anabolic androgenic steroids in substance abusers arrested for crime. Drug Alcohol Depend. 2010, 111, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Klötz, F.; Petersson, A.; Hoffman, O.; Thiblin, I. The significance of anabolic androgenic steroids in a Swedish prison population. Compr. Psychiatry 2010, 51, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Sagoe, D.; Molde, H.; Andreassen, C.S.; Torsheim, T.; Pallesen, S. The global epidemiology of anabolic-androgenic steroid use: A meta-analysis and meta-regression analysis. Ann. Epidemiol. 2014, 24, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Makris, E.; Gourgoulianis, K.I.; Hatzoglou, C. Prisoners and cigarettes or ‘imprisoned in cigarettes’? What helps prisoners quit smoking? BMC Public Health 2012, 12, 508. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Bowles, H.R.; FitzGerald, S.J.; Morrow, J.R., Jr.; Jackson, A.W.; Blair, S.N. Construct validity of self-reported historical physical activity. Am. J. Epidemiol. 2004, 160, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Timperio, A.; Salmon, J.; Crawford, D. Validity and reliability of a physical activity recall instrument among overweight and non-overweight men and women. J. Sci. Med. Sport 2003, 6, 477–491. [Google Scholar] [CrossRef]
- Zuazagoitia, A.; Montoya, I.; Grandes, G.; Arietaleanizbeascoa, M.S.; Arce, V.; Martinez, V.; Sanchez, M.; Sanchez, A. Reliability and validity of the 7-day Physical Activity Recall interview in a Spanish population. Eur. J. Sport Sci. 2014, 14 (Suppl. 1), S361–S368. [Google Scholar] [CrossRef] [PubMed]
- Schulte, M.; Hser, Y. Substance Use and Associated Health Conditions throughout the Lifespan. Public Health Rev. 2014, 35, 17. [Google Scholar] [CrossRef]
- Degenhardt, L.; Whiteford, H.A.; Ferrari, A.J.; Baxter, A.J.; Charlson, F.J.; Hall, W.D.; Freedman, G.; Burstein, R.; Johns, N.; Engell, R.E.; et al. Global burden of disease attributable to illicit drug use and dependence: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1564–1574. [Google Scholar] [CrossRef]
- Martinez-Merino, N.; Martín-González, N.; Usabiaga, O.; Martos-Garcia, D. Physical activity practiced by incarcerated women: A systematic review. Health Care Women Int. 2017, 38, 1152–1169. [Google Scholar] [CrossRef] [PubMed]
- Nøkleby, H. Use of doping agents and symptoms of eating disorders among male and female patients in drug addiction treatment. Nord. Stud. Alcohol Drugs 2013, 30, 331–346. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Harmful Substance Use, n = 1073 | No Harmful Substance Use, n = 391 | Test Statistic | n Missing |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Women | 65 (6.1) | 29 (7.4) | X2(1) = 0.88 | 0 |
| Age (mean, SD) | 32.8 (10.1) | 39.7 (12.8) | z = −9.04 *** | 123 |
| Nordic-born | 833 (79.3) | 203 (54.9) | X2(1) = 80.56 ** | 44 |
| Secondary school or more | 616 (58.1) | 287 (74.5) | X2(1) = 34.52 *** | 18 |
| Single | 785 (73.8) | 199 (52.1) | X2(1) = 61.20 *** | 18 |
| Working or studying before incarceration | 465 (43.3) | 277 (70.8) | X2(1) = 90.83 *** | 0 |
| Incarceration | ||||
| Months of sentence (median, IQR) | 14.0 (28.0) | 27.0 (42.2) | z = −4.15 *** | 274 |
| Months served (median, IQR) | 5.0 (11.3) | 6.3 (19.3) | z = −2.67 ** | 112 |
| Security level | X2(2) = 4.48 | 12 | ||
| High-security | 614 (57.5) | 215 (55.8) | ||
| Low-security | 420 (39.0) | 149 (38.7) | ||
| Transitional housing | 34 (3.2) | 21 (5.5) | ||
| Health during incarceration | ||||
| SCL10 score (mean, SD) | 1.92 (0.79) | 1.77 (0.75) | t(1164) = −3.28 ** | 320 |
| Self-rated physical health | X2(4) = 9.15 | 21 | ||
| Very poor | 53 (5.0) | 22 (5.7) | ||
| Poor | 108 (10.2) | 51 (13.2) | ||
| Neither poor nor good | 245 (23.2) | 79 (20.5) | ||
| Good | 421 (39.8) | 130 (33.8) | ||
| Very good | 231 (21.8) | 103 (26.8) | ||
| Substance and unprescribed medication use during incarceration | ||||
| Frequency | z = −6.92 *** | 65 | ||
| None | 541 (62.1) | 119 (93.0) | ||
| Once | 60 (6.9) | 4 (3.1) | ||
| 2–3 times | 72 (6.7) | 2 (1.6) | ||
| 4+ times | 198 (22.7) | 3 (2.3) | ||
| Substances used | 351 | |||
| Cannabis | 233 (21.7) | 3 (0.8) | X2(1) = 93.9 6 *** | |
| OMT medicine, e.g., methadone | 168 (15.7) | 2 (0.5) | X2(1) = 62.56 *** | |
| Benzodiazepines or sedatives | 123 (11.5) | 1 (0.3) | X2(1) = 45.40 *** | |
| Meth/amphetamines | 68 (6.3) | 1 (0.3) | X2(1) = 25.83 *** | |
| Synthetic cannabis | 43 (4.0) | 0 (0) | X2(1) = 15.80 * | |
| Methylphenidate a, e.g., Ritalin | 39 (3.6) | 0 (0) | X2(1) = 14.29 *** | |
| Heroin | 29 (2.7) | 1 (0.3) | X2(1) = 8.33 ** | |
| Cocaine | 26 (2.4) | 0 (0) | X2(1) = 9.44 ** | |
| Gamma-hydroxybutyric acid (GHB) | 20 (1.9) | 0 (0) | X2(1) = 7.23 ** | |
| Anabolic steroids | 17 (1.6) | 0 (0) | X2(1) = 6.14 * | |
| Inhalants | 11 (1.0) | 0 (0) | X2(1) = 3.95 * | |
| Ecstasy | 9 (0.8) | 0 (0) | X2(1) = 3.23 | |
| LSD, PCP, or ketamine | 7 (0.7) | 0 (0) | X2(1) = 2.51 | |
| Variables | Model | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| (Constant) | --- | --- | --- | --- |
| Pre-incarceration exercise frequency | 0.247 *** | 0.202 *** | 0.187 *** | 0.180 *** |
| Self-rated physical health | 0.326 *** | 0.297 *** | 0.294 *** | |
| Age | −0.136 ** | −0.146 *** | ||
| Secondary school education or higher | 0.101 ** | |||
| Adjusted R2 | 5.9% | 16.3% | 17.8% | 17.8% |
| Variables | Model | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| (Constant) | --- | --- | --- |
| Pre-incarceration exercise frequency | 0.388 *** | 0.358 *** | 0.355 *** |
| Self-rated physical health | 0.261 *** | 0.274 *** | |
| Nordic birth | 0.140 * | ||
| Adjusted R2 | 14.7% | 21.7% | 23.7% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muller, A.E.; Havnes, I.A.; Rognli, E.B.; Bukten, A. Inmates with Harmful Substance Use Increase Both Exercise and Nicotine Use Under Incarceration. Int. J. Environ. Res. Public Health 2018, 15, 2663. https://doi.org/10.3390/ijerph15122663
Muller AE, Havnes IA, Rognli EB, Bukten A. Inmates with Harmful Substance Use Increase Both Exercise and Nicotine Use Under Incarceration. International Journal of Environmental Research and Public Health. 2018; 15(12):2663. https://doi.org/10.3390/ijerph15122663
Chicago/Turabian StyleMuller, Ashley Elizabeth, Ingrid Amalia Havnes, Eline Borger Rognli, and Anne Bukten. 2018. "Inmates with Harmful Substance Use Increase Both Exercise and Nicotine Use Under Incarceration" International Journal of Environmental Research and Public Health 15, no. 12: 2663. https://doi.org/10.3390/ijerph15122663