Spatial Patterns of Satellite-Retrieved PM2.5 and Long-Term Exposure Assessment of China from 1998 to 2016

Abstract
:1. Introduction
2. Materials and Methods
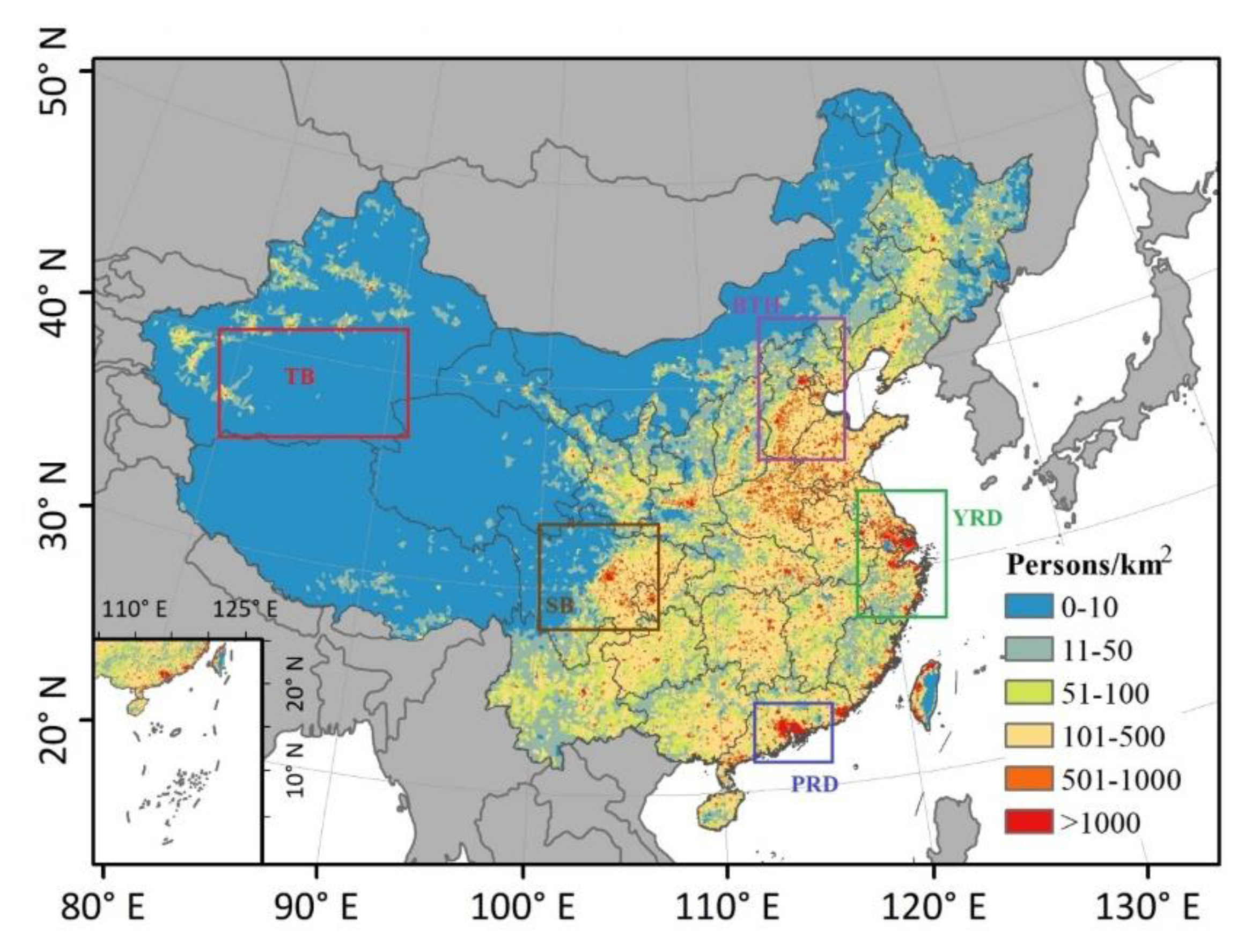
2.1. Study Area
2.2. Data
2.2.1. Satellite-Retrieved PM2.5
2.2.2. Population Data
2.3. Methods
2.3.1. Standard Deviational Ellipse Analysis
2.3.2. Exposure Assessment
2.3.3. Health Risks and Economic Benefits Evaluation
3. Results
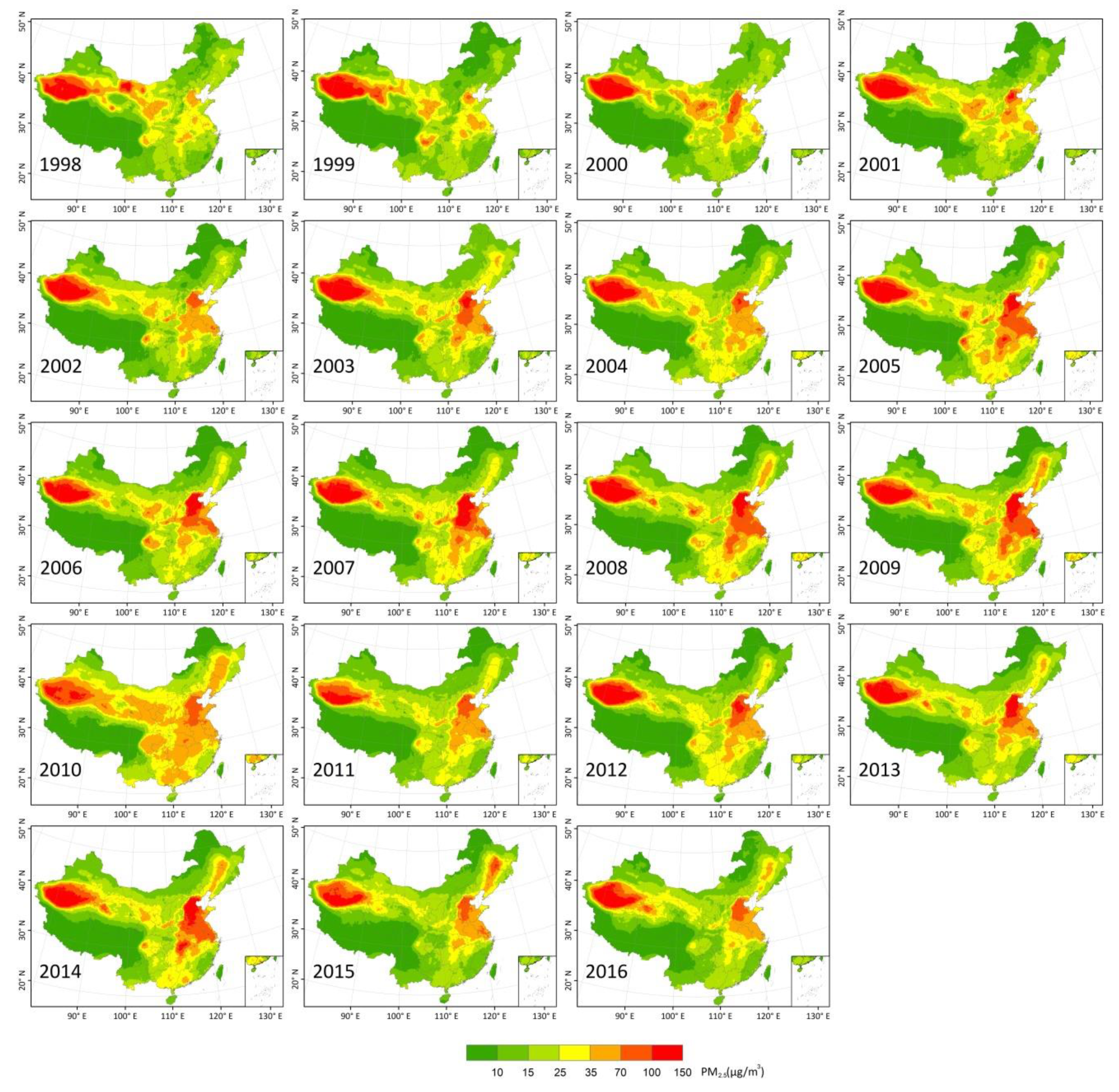
3.1. Spatioemporal Patterns and Variations in PM2.5
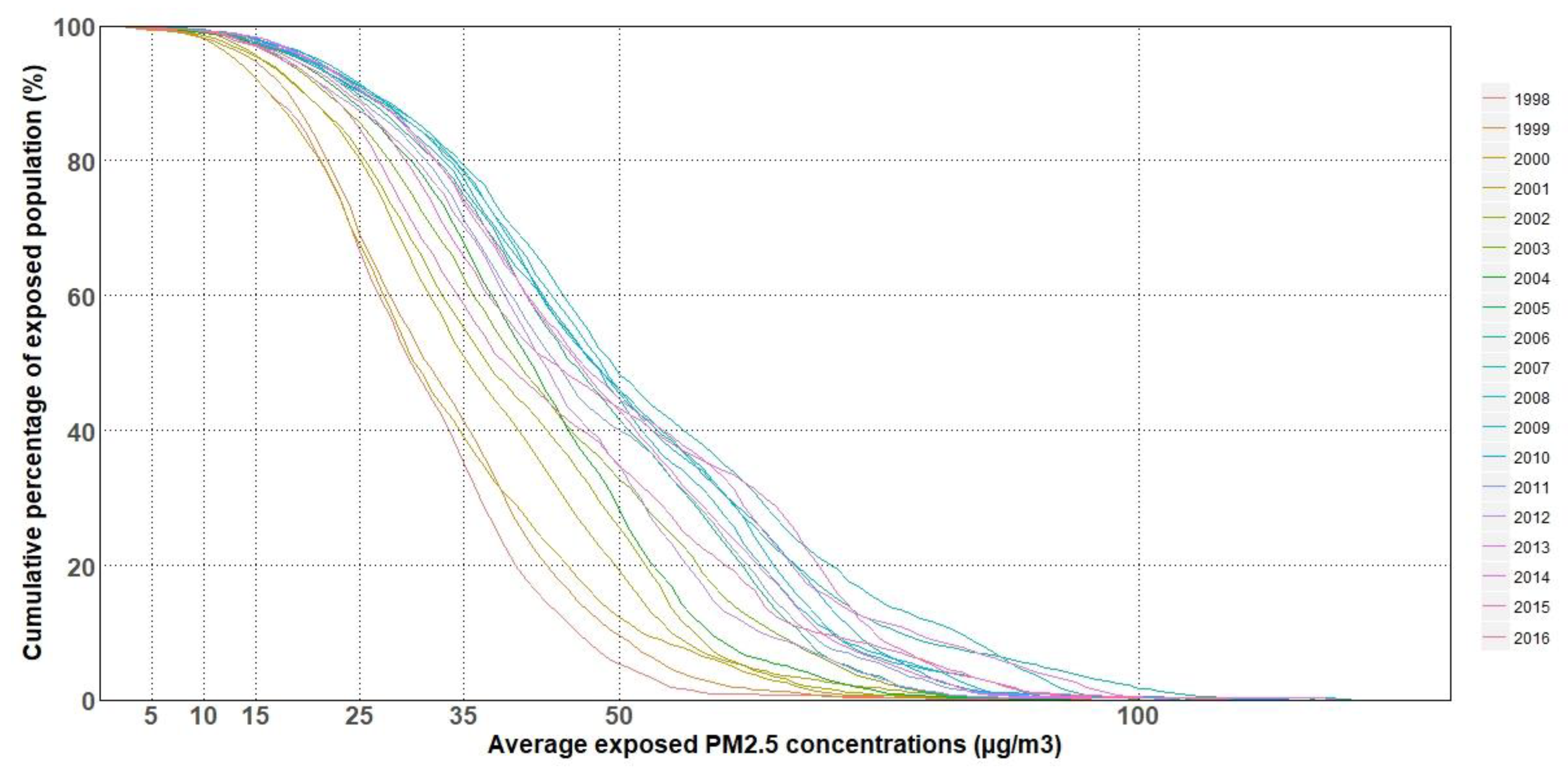
3.2. PM2.5 Exposure Assessment
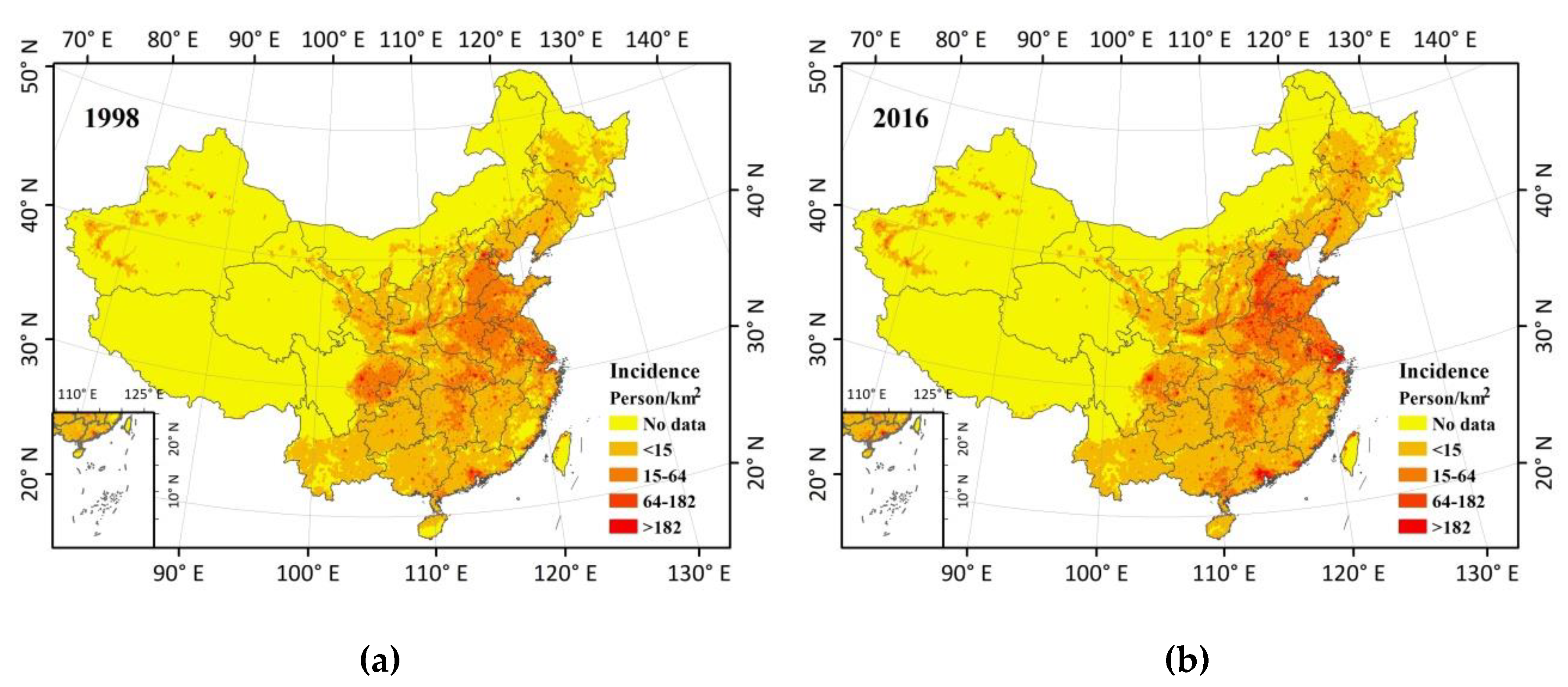
3.3. Health Impact Due to PM2.5 Pollution
4. Discussion
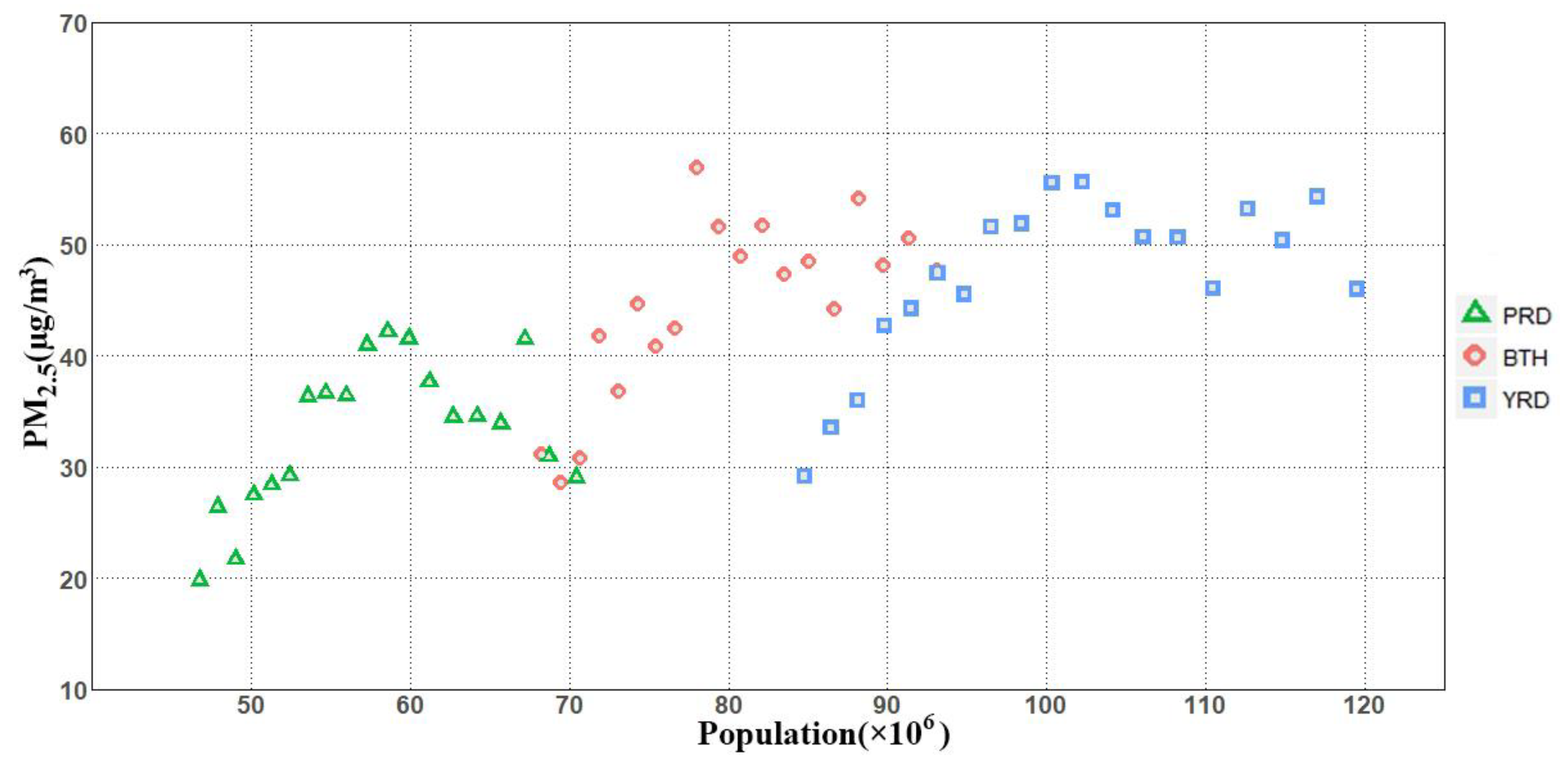
4.1. Correlation between Exposed Population and PM2.5
4.2. Estimating Health Benefits on Air Pollution Prevention and Control Action Plan
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G., Jr.; Speizer, F.E. An association between air pollution and mortality in six US cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef]
- Pope III, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Pope, C.A., III; Thurston, G.; Calle, E.E.; et al. Extended Follow-Up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality (No. 140); Health Effects Institute: Boston, MA, USA, 2009. [Google Scholar]
- World Health Organization. World Health Statistics 2018: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Saucy, A.; Röösli, M.; Künzli, N.; Tsai, M.-Y.; Sieber, C.; Olaniyan, T.; Baatjies, R.; Jeebhay, M.; Davey, M.; Flückiger, B.; et al. Land Use Regression Modelling of Outdoor NO2 and PM2.5 Concentrations in three Low Income Areas in the Western Cape Province, South Africa. Int. J. Environ. Res. Public Health 2018, 15, 1452. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Serre, M.L.; van Donkelaar, A.; Martin, R.V.; Burnett, R.T.; Jerrett, M. Comparison of geostatistical interpolation and remote sensing techniques for estimating long-term exposure to ambient PM2.5 concentrations across the continental United States. Environ. Health Perspect. 2012, 120, 1727. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Chen, D.; Li, R.; Chen, Z.; Cai, J.; He, B.; Gao, B.; Cheng, N.; Huang, Y. Understanding the Influence of Crop Residue Burning on PM2.5 and PM10 Concentrations in China from 2013 to 2017 Using MODIS Data. Int. J. Environ. Res. Public Health 2018, 15, 1504. [Google Scholar] [CrossRef]
- Engel-Cox, J.A.; Holloman, C.H.; Coutant, B.W.; Hoff, R.M. Qualitative and quantitative evaluation of MODIS satellite sensor data for regional and urban scale air quality. Atmos. Environ. 2004, 38, 2495–2509. [Google Scholar] [CrossRef]
- Wang, J.; Christopher, S.A. Intercomparison between satellite-derived aerosol optical thickness and PM2.5 mass: Implications for air quality studies. Geophys. Res. Lett. 2003, 30. [Google Scholar] [CrossRef]
- Hoff, R.M.; Christopher, S.A. Remote Sensing of Particulate Pollution from Space: Have We Reached the Promised Land? J. Air Waste Manag. Assoc. 2009, 59, 645–675. [Google Scholar] [CrossRef]
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Boys, B.L. Use of satellite observations for long-term exposure assessment of global concentrations of fine particulate matter. Environ. Health Perspect. 2015, 123, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Christakos, G.; Yang, X.; He, J. Spatiotemporal characterization and mapping of PM2.5 concentrations in southern Jiangsu Province, China. Environ. Pollut. 2018, 234, 794–803. [Google Scholar] [CrossRef]
- Du, Y.; Sun, T.; Peng, J.; Fang, K.; Liu, Y.; Yang, Y.; Wang, Y. Direct and spillover effects of urbanization on PM2.5 concentrations in China’s top three urban agglomerations. J. Clean Prod. 2018, 190, 72–83. [Google Scholar] [CrossRef]
- Peng, J.; Chen, S.; Lü, H.; Liu, Y.; Wu, J. Spatiotemporal patterns of remotely sensed PM2.5 concentration in China from 1999 to 2011. Remote Sens. Environ. 2016, 174, 109–121. [Google Scholar] [CrossRef]
- Shi, Y.; Matsunaga, T.; Yamaguchi, Y.; Li, Z.; Gu, X.; Chen, X. Long-term trends and spatial patterns of satellite-retrieved PM2.5 concentrations in South and Southeast Asia from 1999 to 2014. Sci. Total Environ. 2018, 615, 177–186. [Google Scholar] [CrossRef]
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Hsu, N.C.; Kahn, R.A.; Levy, R.C.; Lyapustin, A.; Sayer, A.M.; Winker, D.M. Global Estimates of Fine Particulate Matter using a Combined Geophysical-Statistical Method with Information from Satellites, Models, and Monitors. Environ. Sci. Technol. 2016, 50, 3762–3772. [Google Scholar] [CrossRef] [PubMed]
- Kim, O.J.; Kim, S.Y.; Kim, H. Association between Long-Term Exposure to Particulate Matter Air Pollution and Mortality in a South Korean National Cohort: Comparison across Different Exposure Assessment Approaches. Int. J. Environ. Res. Public Health 2017, 14, 1103. [Google Scholar] [CrossRef]
- Pascal, M.; Falq, G.; Wagner, V.; Chatignoux, E.; Corso, M.; Blanchard, M.; Host, S.; Pascal, L.; Larrieu, S. Short-term impacts of particulate matter (PM10, PM10–2.5, PM2.5) on mortality in nine French cities. Atmos. Environ. 2014, 95, 175–184. [Google Scholar] [CrossRef]
- Li, M.; Wu, Y.; Tian, Y.-H.; Cao, Y.-Y.; Song, J.; Huang, Z.; Wang, X.-W.; Hu, Y.-H. Association Between PM2.5 and Daily Hospital Admissions for Heart Failure: A Time-Series Analysis in Beijing. Int. J. Environ. Res. Public Health 2018, 15, 2217. [Google Scholar] [CrossRef]
- De Marco, A.; Amoatey, P.; Khaniabadi, Y.O.; Sicard, P.; Hopke, P.K. Mortality and morbidity for cardiopulmonary diseases attributed to PM2.5 exposure in the metropolis of Rome, Italy. Eur. J. Intern. Med. 2018, 57, 49–57. [Google Scholar] [CrossRef]
- Khaniabadi, Y.O.; Sicard, P.; Takdastan, A.; Hopke, P.K.; Taiwo, A.M.; Khaniabadi, F.O.; De Marco, A.; Daryanoosh, M. Mortality and morbidity due to ambient air pollution in Iran. Clin. Epidemiol. Glob. Health 2018, in press. [Google Scholar] [CrossRef]
- Cohen, A.J. Urban Air Pollution, in Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors; Ezzati, M., Lopez, A.D., Murray, C.J.L., Eds.; World Health Organization: Geneva, Switzerland, 2004; pp. 1353, 1433. [Google Scholar]
- Ostro, B.; World Health Organization. Outdoor Air Pollution: Assessing the Environmental Burden of Disease at National and Local Levels; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Daryanoosh, M.; Goudarzi, G.; Rashidi, R.; Keishams, F.; Hopke, P.K.; Mohammadi, M.J.; Nourmoradi, H.; Sicard, P.; Takdastan, A.; Vosoughi, M.; et al. Risk of morbidity attributed to ambient PM10 in the western cities of Iran. Toxin Rev. 2017. [Google Scholar] [CrossRef]
- Burnett, R.T.; Pope, C.A., III; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Sacks, J.D.; Lloyd, J.M.; Zhu, Y.; Anderton, J.; Jang, C.J.; Hubbell, B.; Fann, N. The Environmental Benefits Mapping and Analysis Program—Community Edition (BenMAP-CE): A tool to estimate the health and economic benefits of reducing air pollution. Environ. Model. Softw. 2018, 104, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Mehra, S. Estimating the Impact of a Select Criteria Pollutant (PM2.5) on Childhood Asthma in Florida. Ph.D. Thesis, University of South Florida, Tampa, FL, USA, 2017. [Google Scholar]
- Stewart, D.R.; Saunders, E.; Perea, R.A.; Fitzgerald, R.; Campbell, D.E.; Stockwell, W.R. Linking Air Quality and Human Health Effects Models: An Application to the Los Angeles Air Basin. Environ. Health Insights 2017, 11, 1178630217737551. [Google Scholar] [CrossRef]
- Carvour, M.L.; Hughes, A.E.; Fann, N.; Haley, R.W. Estimating the Health and Economic Impacts of Changes in Local Air Quality. Am. J. Public Health. 2018, 108, S151–S157. [Google Scholar] [CrossRef]
- Chen, L.; Shi, M.; Li, S.; Bai, Z.; Wang, Z. Combined use of land use regression and BenMAP for estimating public health benefits of reducing PM2.5 in Tianjin, China. Atmos. Environ. 2017, 152, 16–23. [Google Scholar] [CrossRef]
- Gopalakrishnan, V.; Hirabayashi, S.; Ziv, G.; Bakshi, B.R. Air quality and human health impacts of grasslands and shrublands in the United States. Atmos. Environ. 2018, 182, 193–199. [Google Scholar] [CrossRef]
- Lefever, D.W. Measuring geographic concentration by means of the standard deviational ellipse. Am. J. Sociol. 1926, 32, 88–94. [Google Scholar] [CrossRef]
- Wang, B.; Shi, W.; Miao, Z. Confidence analysis of standard deviational ellipse and its extension into higher dimensional euclidean space. PLoS ONE 2015, 10, e0118537. [Google Scholar] [CrossRef]
- World Health Organization. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide—Global Update 2005—Summary of Risk Assessment, 2006; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- National Bureau of Statistics. National Bureau of Statistics 2012 China Statistical Yearbook 2012; China Statistics Press: Beijing, China, 2012.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | PM2.5 (µg/m3) | Basis for Selected Level |
|---|---|---|
| Interim Target-1 (IT-1) | 35 | These levels are associated with about a 15% higher long-term mortality risk relative to the AQG level. |
| Interim Target-2 (IT-2) | 25 | In addition to other health benefits, these levels lower the risk of premature mortality by approximately 6% (2%–11%) relative to the IT-1 level. |
| Interim Target-3 (IT-3) | 15 | In addition to other health benefits, these levels reduce mortality risk by approximately 6% (2%–11%) relative to the IT-2 level. |
| Air quality guideline (AQG) | 10 | These are the lowest levels at which total, cardiopulmonary, and lung cancer mortality have been shown to increase with more than 95% confidence in response to long-term exposure to PM2.5. |
| Year | Median Center (°) | Major Axis (km) | Minor Axis (km) | Azimuth (°) | |
|---|---|---|---|---|---|
| Longitude | Latitude | ||||
| 1998 | 102.91 | 37.88 | 1746.5 | 955.3 | 98.7 |
| 1999 | 102.31 | 37.25 | 1750.1 | 941.4 | 102.7 |
| 2000 | 104.66 | 37.14 | 1758.5 | 962.9 | 99.6 |
| 2001 | 103.64 | 36.99 | 1763.0 | 928.7 | 100.9 |
| 2002 | 103.90 | 37.04 | 1784.5 | 951.9 | 99.9 |
| 2003 | 105.70 | 37.07 | 1785.0 | 1019.4 | 95.5 |
| 2004 | 104.58 | 36.54 | 1764.6 | 979.2 | 101.4 |
| 2005 | 106.14 | 36.02 | 1766.3 | 1005.3 | 100.9 |
| 2006 | 105.97 | 36.43 | 1745.6 | 971.1 | 100.1 |
| 2007 | 106.49 | 36.16 | 1747.5 | 979.1 | 100.9 |
| 2008 | 105.70 | 36.36 | 1775.8 | 1016.9 | 99.4 |
| 2009 | 106.30 | 36.40 | 1742.6 | 1010.5 | 98.7 |
| 2010 | 105.21 | 36.61 | 1785.9 | 976.7 | 99.3 |
| 2011 | 105.97 | 36.27 | 1756.6 | 996.7 | 99.2 |
| 2012 | 105.59 | 36.31 | 1768.6 | 1008.7 | 100.1 |
| 2013 | 105.46 | 36.79 | 1763.2 | 983.2 | 98.6 |
| 2014 | 106.10 | 36.48 | 1748.0 | 1028.9 | 98.2 |
| 2015 | 105.63 | 37.48 | 1824.2 | 1011.3 | 94.1 |
| 2016 | 103.31 | 37.60 | 1837.9 | 988.9 | 95.3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, T.; Deng, S.; Li, M. Spatial Patterns of Satellite-Retrieved PM2.5 and Long-Term Exposure Assessment of China from 1998 to 2016. Int. J. Environ. Res. Public Health 2018, 15, 2785. https://doi.org/10.3390/ijerph15122785
Chen T, Deng S, Li M. Spatial Patterns of Satellite-Retrieved PM2.5 and Long-Term Exposure Assessment of China from 1998 to 2016. International Journal of Environmental Research and Public Health. 2018; 15(12):2785. https://doi.org/10.3390/ijerph15122785
Chicago/Turabian StyleChen, Tan, Shulin Deng, and Manchun Li. 2018. "Spatial Patterns of Satellite-Retrieved PM2.5 and Long-Term Exposure Assessment of China from 1998 to 2016" International Journal of Environmental Research and Public Health 15, no. 12: 2785. https://doi.org/10.3390/ijerph15122785