An Ecological Study on the Spatially Varying Relationship between County-Level Suicide Rates and Altitude in the United States

Abstract
:1. Introduction
2. Materials and Methods
2.1. Suicide Rates
2.2. Mean County Altitude Data
2.3. Independent Variables
2.4. Statistical Analyses
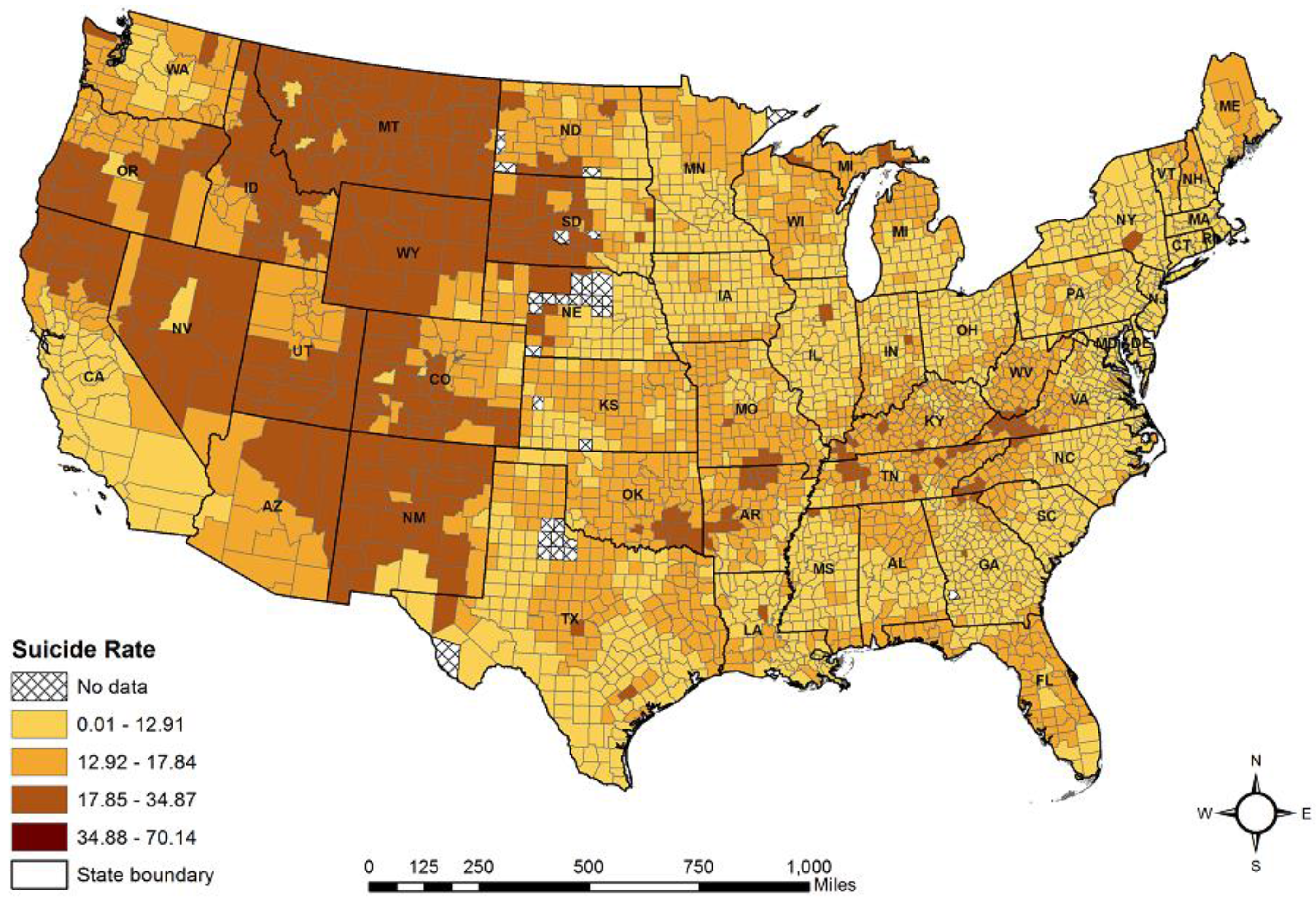
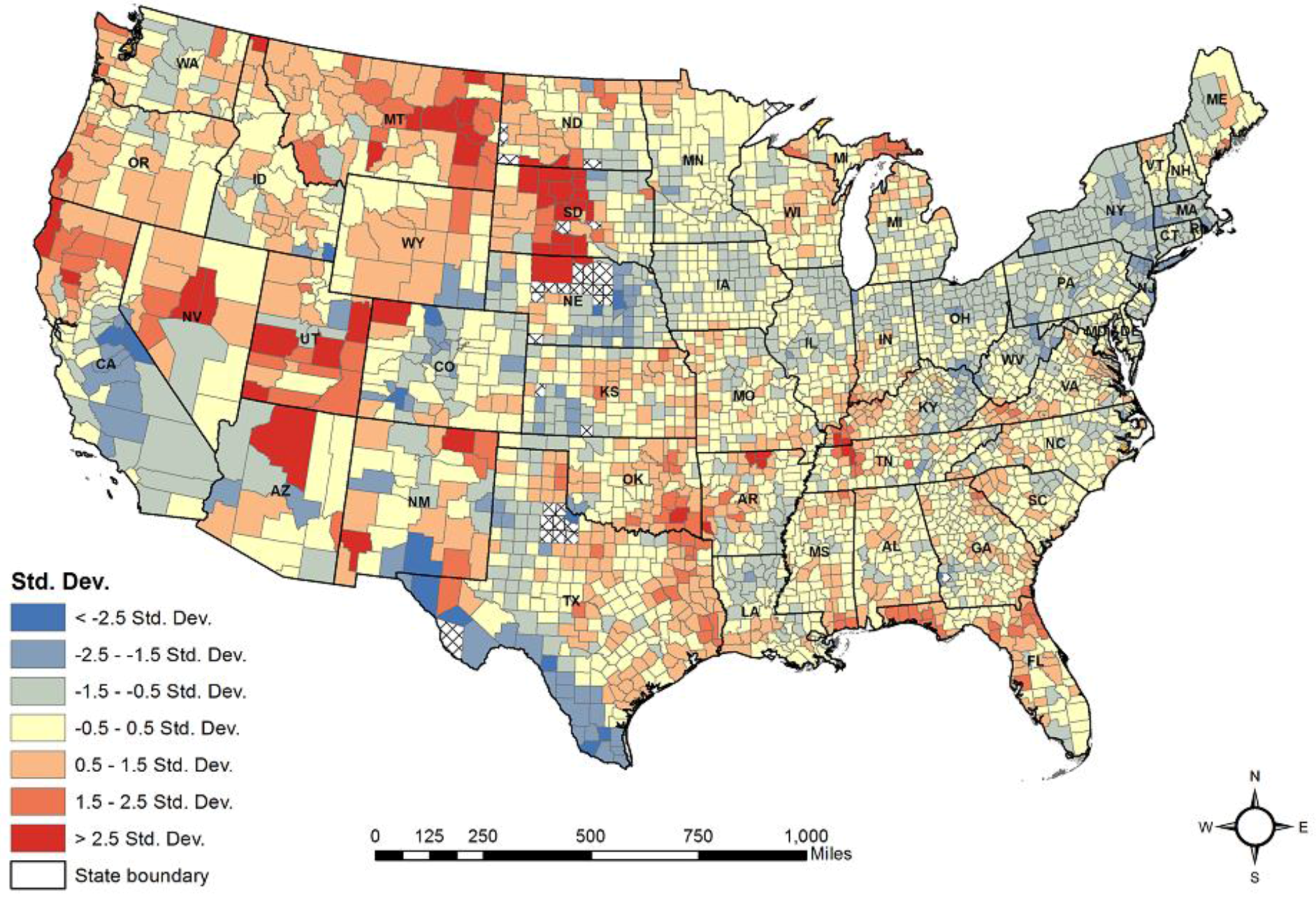
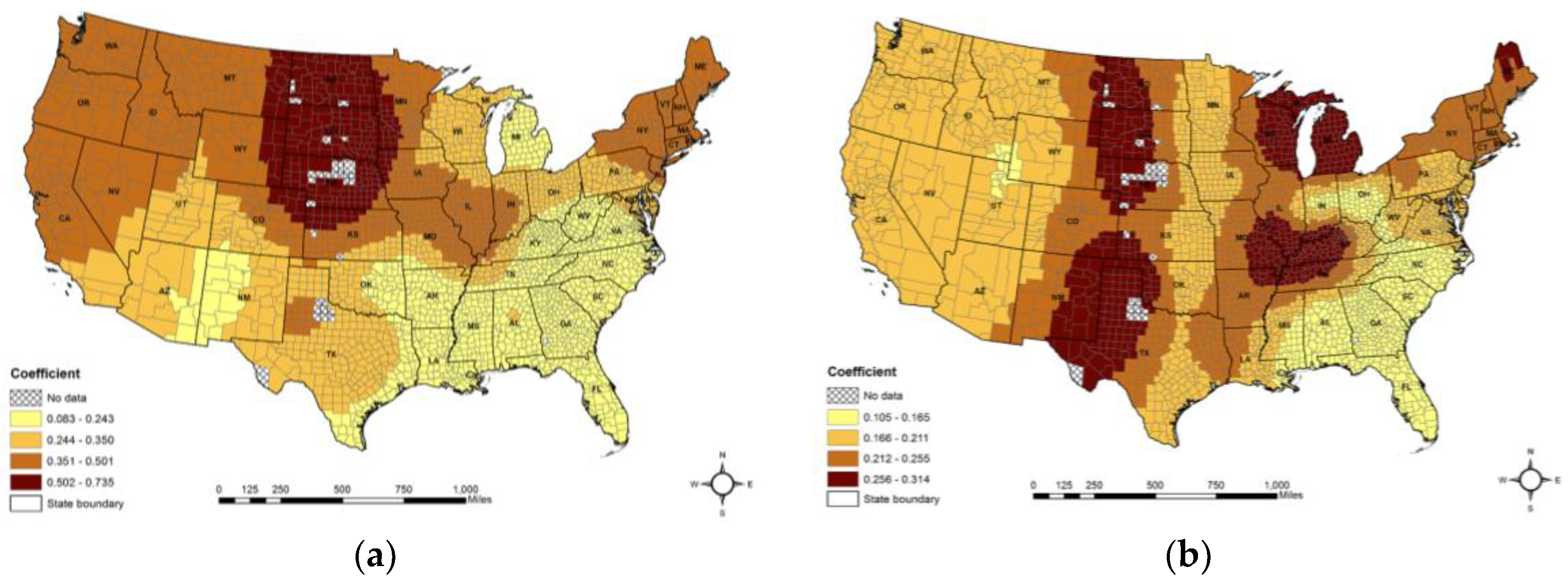
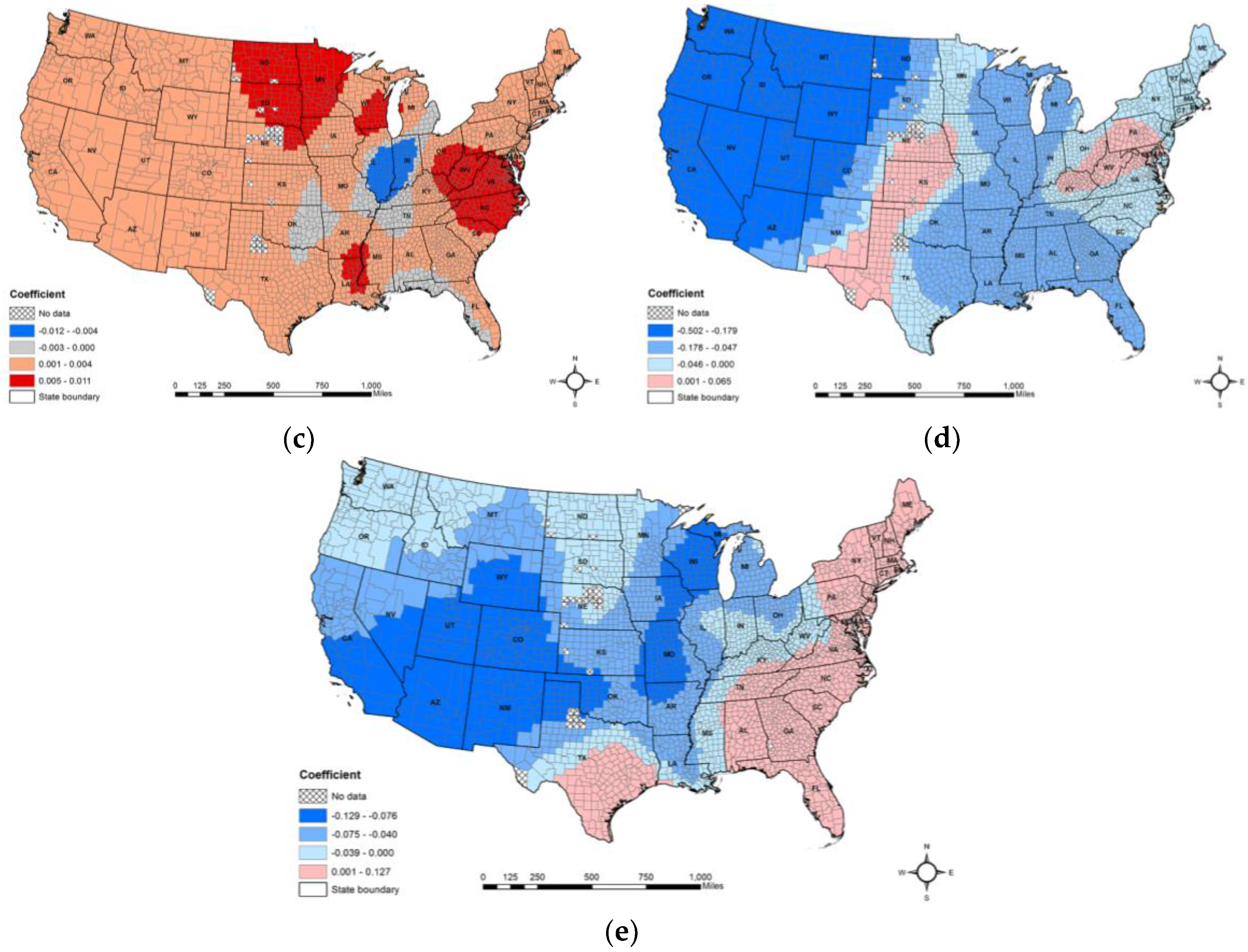
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, 2011–2030. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- World Health Organization (WHO). Suicide Data. 2017. Available online: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ (accessed on 7 September 2017).
- Florence, C.; Haegerich, T.; Simon, T.; Zhou, C.; Luo, F. Estimated lifetime medical and work-loss costs of emergency department–treated nonfatal injuries—United States, 2013. Morb. Mortal. Wkly. Rep. 2015, 64, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- Shepard, D.S.; Gurewich, D.; Lwin, A.K.; Reed, G.A., Jr.; Silverman, M.M. Suicide and suicidal attempts in the United States: Costs and policy implications. Suicide Lift Threat Behav. 2016, 46, 352–362. [Google Scholar] [CrossRef] [PubMed]
- The National Institute of Mental Health (NIMH). Suicide. 2017. Available online: https://www.nimh.nih.gov/health/statistics/suicide/index.shtml (accessed on 7 September 2017).
- Daly, M.C.; Wilson, D.J.; Johnson, N.J. Relative status and well-being: Evidence from U.S. Suicide deaths. Rev. Econ. Stat. 2007, 95, 1480–1500. [Google Scholar] [CrossRef]
- Dumais, A.; Lesage, A.D.; Alda, M.; Rouleau, G.; Dumont, M.; Chawky, N.; Roy, M.; Mann, J.J.; Benkelfat, C.; Turecki, G. Risk factors for suicide completion in major depression: A case-control study of impulsive and aggressive behaviors in men. Am. J. Psychiatry 2005, 162, 2116–2124. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.R. Smoking and suicide: A brief overview. Drug Alcohol Depend. 2008, 98, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Poorolajal, J.; Darvishi, N. Smoking and Suicide: A Meta-Analysis. PLoS ONE 2016, 11, e0156348. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.E.; Oquendo, M.A.; Stanley, B. Religion and Suicide Risk: A Systematic Review. Arch. Suicide Res. 2016, 20, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M. Increasing rural–urban gradients in US suicide mortality, 1970–1997. Am. J. Public Health 2002, 92, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Stack, S. Suicide: A 15-year review of the sociological literature part I: Cultural and economic factors. Suicide Life Threat Behav. 2000, 30, 145–162. [Google Scholar] [PubMed]
- Deisenhammer, E.A.; Kemmler, G.; Parson, P. Association of meteorological factors with suicide. Acta Psychiatr. Scand. 2003, 108, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Young, S. Elevated incidence of suicide in people living at altitude, smokers and patients with chronic obstructive pulmonary disease and asthma: Possible role of hypoxia causing decreased serotonin synthesis. J. Psychiatry Neurosci. 2013, 38, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.Z.; Li, L.; Song, Y.F.; Zhou, Y.X.; Shen, S.Q.; Ou, C.Q. The impact of ambient air pollution on suicide mortality: A case-crossover study in Guangzhou, China. Environ. Health 2016, 15, 90. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.; Cheng, D.; Clark, S.; Camargo, C.A., Jr. Positive association between altitude and suicide in 2584 US counties. High Alt. Med. Biol. 2011, 12, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Park, J.M.; Finn, C.T.; Deliberto, T.L.; Dour, H.J.; Banaji, M.R. Measuring the suicidal mind: Implicit cognition predicts suicidal behavior. Psychol. Sci. 2010, 21, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Strandheim, A.; Bjerkeset, O.; Gunnell, D.; Bjørnelv, S.; Holmen, T.L.; Bentzen, N. Risk factors for suicidal thoughts in adolescence-a prospective cohort study: The Young-HUNT study. BMJ Open 2014, 4, e005867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdeen, Z.; Brunstein-Klomek, A.; Nakash, O.; Shibli, N.; Nagar, M.; Agha, H.; Hallaq, S.; Kanat-Maymon, Y.; Juerges, H.; Levav, I.; et al. The Association between Political Violence and the Connection between Bullying and Suicidality among Palestinian Youth. Suicide Life Threat Behav. 2017. [Google Scholar] [CrossRef] [PubMed]
- Harper, S.; Charters, T.J.; Strumpf, E.C.; Galea, S.; Nandi, A. Economic downturns and suicide mortality in the USA, 1980–2010: Observational study. Int. J. Epidemiol. 2015, 44, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Norstrom, T.; Gronqvist, H. The Great Recession, unemployment and suicide. J. Epidemiol. Community Health 2015, 69, 110–116. [Google Scholar] [CrossRef] [PubMed]
- U.S. Centers for Disease Control Prevention (U.S. CDC). Fatal Injury Reports, National, Regional and State, 1981–2015. Atlanta, CDC, Webbased Injury Statistics Query and Reporting System (WISQARS). 2017. Available online: https://webappa.cdc.gov/sasweb/ncipc/mortrate.html (accessed on 7 September 2017).
- Lester, D. Variation in suicide and homicide rates by latitude and longitude in the United States, Canada, and Australia. Am. J. Psychiatry 1985, 142, 523–524. [Google Scholar] [PubMed]
- Chang, S.S.; Sterne, J.A.; Wheeler, B.W.; Lu, T.H.; Lin, J.J.; Gunnell, D. Geography of suicide in Taiwan: Spatial patterning and socioeconomic correlates. Health Place 2011, 17, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Mickelson, J.B.; Brenner, B.E.; Haws, C.A.; Yurgelun-Todd, D.A.; Renshaw, P.F. Altitude, gun ownership, rural areas, and suicide. Am. J. Psychiatry 2011, 168, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Trgovac, A.B.; Kedron, P.J.; Bagchi-Sen, S. Geographic variation in male suicide rates in the United States. Appl. Geogr. 2015, 62, 201–209. [Google Scholar] [CrossRef]
- Bearman, P.S. The social structure of suicide. Sociol. Forum 1991, 6, 501–524. [Google Scholar] [CrossRef]
- Durkheim, E.; Simpson, G. Suicide: A Study in Sociology; Routledge & Kegan Paul: London, UK, 1952. [Google Scholar]
- Anestis, M.D.; Houtsma, C. The Association between Gun Ownership and Statewide Overall Suicide Rates. Suicide Life Threat Behav. 2017. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.; Hemenway, D. Guns and suicide in the United States. N. Engl. J. Med. 2008, 359, 989–991. [Google Scholar] [CrossRef] [PubMed]
- Siegel, M.; Rothman, E.F. Firearm Ownership and Suicide Rates among US Men and Women, 1981–2013. Am. J. Public Health 2016, 106, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- Guger, C.; Krausert, S.; Domej, W.; Edlinger, G.; Tannheimer, M. EEG, ECG and oxygen concentration changes from sea level to a simulated altitude of 4000 m and back to sea level. Neurosci. Lett. 2008, 442, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Katz, I.R. Is there a hypoxic affective syndrome? Psychosomatics 1982, 23, 846–853. [Google Scholar] [CrossRef]
- Shukitt-Hale, B.; Banderet, L.E.; Lieberman, H.R. Elevation-dependent symptom, mood, and performance changes produced by exposure to hypobaric hypoxia. Int. J. Aviat. Psychol. 1998, 8, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Kious, B.M.; Kondo, D.G.; Renshaw, P.F. Living High and Feeling Low: Altitude, Suicide, and Depression. Harv. Rev. Psychiatry 2018, 26, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Reno, E.; Brown, T.L.; Betz, M.E.; Allen, M.H.; Hoffecker, L.; Reitinger, J.; Roach, R.; Honigman, B. Suicide and high altitude: An integrative review. High Alt. Med. Biol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Choi, N.; Lee, Y.J.; An, H.; Kim, N.; Yoon, H.K.; Lee, H.-J. High altitude remains associated with elevated suicide rates after adjusting for socioeconomic status: A study from South Korea. Psychiatry Investig. 2014, 11, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Prado, E.; Simbaña, K.; Gómez, L.; Henriquez-Trujillo, A.R.; Cornejo-Leon, F.; Vasconez, E.; Castillo, D.; Viscor, G. The disease burden of suicide in Ecuador, a 15 years’ geodemographic cross-sectional study (2001–2015). BMC Psychiatry 2017, 17, 342. [Google Scholar] [CrossRef] [PubMed]
- Selek, S. Altitude, immigration and suicide rates: A study from Turkey. Psychiatry Investig. 2013, 10, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Oka, M.; Kubota, T.; Tsubaki, H.; Yamauchi, K. Analysis of impact of geographic characteristics on suicide rate and visualization of result with Geographic Information System. Psychiatry Clin. Neurosci. 2015, 69, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, M.; Yamanaka, G.; Nakajima, S.; Suwa, K.; Matsuda, A.; Nakaoka, T.; Okumiya, K.; Matsubayashi, K.; Otsuka, K. Association between high altitude and depression in the Himalayas and the Andes. Nihon Ronen Igakkai Zasshi 2013, 50, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Haws, C.A.; Gray, D.D.; Yurgelun-Todd, D.A.; Moskos, M.; Meyer, L.J.; Renshaw, P.F. The possible effect of altitude on regional variation in suicide rates. Med. Hypotheses 2009, 73, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Goovaerts, P. Geostatistical analysis of health data: State-of-the-art and perspectives. Geostat. Environ. Appl. 2008, 15, 3–22. [Google Scholar]
- Leung, Y. Discovery of Spatial Relationships in Spatial Data. In Knowledge Discovery in Spatial Data; Springer: Berlin, Germany, 2010; pp. 223–276. [Google Scholar]
- Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships; Wiley: Hoboken, NJ, USA, 2002. [Google Scholar]
- Chan, T.C.; Chiang, P.H.; Su, M.D.; Wang, H.W.; Liu, M.S. Geographic disparity in chronic obstructive pulmonary disease (COPD) mortality rates among the Taiwan population. PLoS ONE 2014, 9, e98170. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Wen, T.H. Using geographically weighted regression (GWR) to explore spatial varying relationships of immature mosquitoes and human densities with the incidence of dengue. Int. J. Environ. Res. Public Health. 2011, 8, 2798–2815. [Google Scholar] [CrossRef] [PubMed]
- Shoff, C.; Yang, T.C. Spatially varying predictors of teenage birth rates among counties in the United States. Demogr. Res. 2012, 27, 377–418. [Google Scholar] [CrossRef] [PubMed]
- Tu, J.; Tu, W.; Tedders, S.H. Spatial variations in the associations of term birth weight with ambient air pollution in Georgia, USA. Environ. Int. 2016, 92, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Helbich, M.; Leitner, M.; Kapusta, N.D. Geospatial examination of lithium in drinking water and suicide mortality. Int. J. Helath Geogr. 2012, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Cheng, D.C.; Mendenhall, T.I.; Barry, B. Suicide rates strongly correlate with altitude. Acad. Emerg. Med. 2005, 12 (Suppl. 1), 141. [Google Scholar] [CrossRef]
- Huber, R.; Coon, H.; Kim, N.; Renshaw, P.F.; Kondo, D.G. Altitude is a Risk Factor for Completed Suicide in Bipolar Disorder. Med. Hypotheses 2014, 82, 377–381. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics (NCHS). WISQARS Fatal Injury Mortality Reports, 1999–2007; National Center for Inquiry Prevention and Control: Atlanta, GA, USA, 2011.
- U.S. Geological Survey (USGS). 100-Meter Resolution Elevation of the Conterminous United States. 2012. Available online: https://catalog.data.gov/dataset/100-meter-resolution-color-sliced-elevation-of-the-conterminous-united-states-direct-download (accessed on 10 September 2017).
- ESRI. ArcGIS 10.3.1. 2015. Available online: http://desktop.arcgis.com/en/arcmap/10.3/main/get-started/whats-new-in-arcgis-1031.htm (accessed on 7 October 2017).
- The U.S. Census Bureau. Geography: Cartographic Boundary Shapefiles—Counties. 2017. Available online: https://www.census.gov/geo/maps-data/data/cbf/cbf_counties.html (accessed on 8 September 2017).
- Ha, H. Geographic variation in Mentally Unhealthy Days: Air pollution and altitude perspectives. High Alt. Med. Biol. 2017, 18, 258–266. [Google Scholar] [CrossRef] [PubMed]
- The U.S. Census Bureau. Population and Housing Unit Estimates. 2017. Available online: https://www.census.gov/programs-surveys/popest.html (accessed on 8 September 2017).
- U.S. Centers for Disease Control Prevention (U.S. CDC). SMART: BRFSS City and County Data and Documentation. 2017. Available online: https://www.cdc.gov/brfss/smart/Smart_data.htm (accessed on 7 December 2016).
- Voss, J.D.; Masuoka, P.; Webber, B.J.; Scher, A.I.; Atkinson, R.L. Association of elevation, urbanization and ambient temperature with obesity prevalence in the United States. Int. J. Obes. 2013, 37, 1407–1412. [Google Scholar] [CrossRef] [PubMed]
- The U.S. Census Bureau. The American Community Survey. 2017. Available online: https://www.census.gov/programs-surveys/acs/ (accessed on 8 September 2017).
- Rogerson, P.A. Statistical Methods for Geography, 2nd ed.; Sage: London, UK, 2006. [Google Scholar]
- Mennis, J. Mapping the results of geographically weighted regression. Cartogr. J. 2006, 43, 171–179. [Google Scholar] [CrossRef]
- Hoaglin, D.C.; Welsch, R.E. The hat matrix in regression and ANOVA. Am. Stat. 1978, 32, 17–22. [Google Scholar]
- Nakaya, T.; Charlton, M.; Fotheringham, A.S.; Brunsdon, C. Geographically Weighted Regression Version 4. User’s Manual and Installation Guide. 2009. Available online: http://gwr.maynoothuniversity.ie/wp-content/uploads/2013/04/GWR4_Manual.pdf (accessed on 8 September 2017).
- Fontanella, C.A.; Hiance-Steelesmith, D.L.; Phillips, G.S.; Bridge, J.A.; Lester, N.; Sweeney, H.A.; Campo, J.V. Widening rural-urban disparities in youth suicides, United States, 1996–2010. JAMA Pediatr. 2015, 169, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.K. A review of the literature on rural suicide: Risk and protective factors, incidence, and prevention. Crisis 2006, 27, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Ha, H. The Conversation. The Curious Relationship between Altitude and Suicide. 2017. Available online: https://theconversation.com/the-curious-relationship-between-altitude-and-suicide-85716 (accessed on 5 November 2017).
- Betz, M.E.; Valley, M.A.; Lowenstein, S.R.; Hedegaard, H.; Thomas, D.; Stallones, L.; Honigman, B. Elevated suicide rates at high altitude: Sociodemographic and health issues may be to blame. Suicide Life Threat Behav. 2011, 41, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Tøllefsen, I.M.; Hem, E.; Ekeberg, Ø. The reliability of suicide statistics: A systematic review. BMC Psychiatry 2012, 12, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Páez, A.; Farber, S.; Wheeler, D. A simulation-based study of geographically weighted regression as a method for investigating spatially varying relationships. Environ. Plan. A 2011, 43, 2992–3010. [Google Scholar] [CrossRef]
- Wheeler, D.; Tiefelsdorf, M. Multicollinearity and correlation among local regression coefficients in geographically weighted regression. J. Geogr. Syst. 2005, 7, 161–187. [Google Scholar] [CrossRef]
- Fotheringham, A.S.; Oshan, T.M. Geographically weighted regression and multicollinearity: Dispelling the myth. J. Geogr. Syst. 2016, 18, 303–329. [Google Scholar] [CrossRef]
- MacNab, Y.; Dean, C.B. Spatio-temporal modelling of rates for the construction of disease maps. Stat. Med. 2002, 21, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Meliker, J.R.; Sloan, C.D. Spatio-temporal epidemiology: Principles and opportunities. Spat. Spatio-temp. Epudemiol. 2011, 2, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fotheringham, A.S.; Crespo, R.; Yao, J. Geographical and Temporal Weighted Regression (GTWR). Geogr. Anal. 2015, 47, 431–452. [Google Scholar] [CrossRef]
- Huang, B.; Wu, B.; Barry, M. Geographically and temporally weighted regression for modeling spatio-temporal variation in house prices. Int. J. Geogr. Inf. Sci. 2010, 24, 383–401. [Google Scholar] [CrossRef]
- Jessen, G.; Steffensen, P.; Jensen, B. Seasons and meteorological factors in suicidal behaviour. Arch. Suicide Res. 1998, 4, 263–280. [Google Scholar] [CrossRef]
- Deisenhammer, E.A. Weather and suicide: The present state of knowledge on the association of meteorological factors with suicidal behaviour. Acta Psychiatr. Scand. 2003, 108, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Gunnell, D.; Wheeler, B.; Chang, S.S.; Thomas, B.; Sterne, J.A.; Dorling, D. Changes in the geography of suicide in young men: England and Wales 1981–2005. J. Epidemiol. Community Health 2012, 66, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Santana, P.; Costa, C.; Cardoso, G.; Loureiro, A.; Ferrão, J. Suicide in Portugal: Spatial determinants in a context of economic crisis. Health Place 2015, 35, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Abellan, J.J.; Richardson, S.; Best, N. Use of space–time models to investigate the stability of patterns of disease. Environ. Health Perspect. 2008, 116, 1111. [Google Scholar] [CrossRef] [PubMed]
- Blangiardo, M.; Cameletti, M.; Baio, G.; Rue, H. Spatial and spatio-temporal models with R-INLA. Spat. Spatio-temp. Epidemiol. 2013, 7, 39–55. [Google Scholar] [CrossRef]
- Helbich, M.; Plener, P.L.; Hartung, S.; Blüml, V. Spatiotemporal Suicide Risk in Germany: A Longitudinal Study 2007–11. Sci. Rep. 2017, 7, 7673. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health behavior and clinical care variables |
|
| Social and economic variables |
|
| Physical environmental variables |
|
| Demographic variables |
|
| Model—With Mean County Altitude and Independent Variables—R-Squared = 0.485 | ||||
|---|---|---|---|---|
| Coefficient | S.E | t-Value | p-Value | |
| Intercept | 5.147 | 1.270 | 4.053 | 0.000 a |
| % smokers | 0.312 | 0.019 | 16.556 | 0.000 a |
| % obesity | 0.005 | 0.017 | 0.298 | 0.766 |
| Primary care physician rate | 0.002 | 0.002 | 1.381 | 0.167 |
| % college education | 0.006 | 0.006 | 1.101 | 0.271 |
| % unemployment | 0.008 | 0.029 | 0.292 | 0.771 |
| % of single-parent households | 0.006 | 0.007 | 0.825 | 0.410 |
| Association rate | −0.053 | 0.009 | −6.142 | 0.000 a |
| % severe housing problems | 0.013 | 0.014 | −0.913 | 0.361 |
| % aged 65 and over | 0.226 | 0.015 | 15.566 | 0.000 a |
| % African American | −0.036 | 0.005 | −7.092 | 0.000 a |
| % female | −0.057 | 0.024 | −2.318 | 0.021 |
| % rural area | 0.002 | 0.002 | 0.865 | 0.387 |
| Mean county altitude | 0.004 | 0.000 | 35.974 | 0.000 a |
| Mean | SD | Range | |
|---|---|---|---|
| Suicide rates (per 100,000 population) | 13.53 | 3.53 | 5.17–70.14 |
| % smokers | 18.39 | 3.71 | 6.90–41.20 |
| % obesity | 30.94 | 4.46 | 10.70–46.60 |
| Primary care physician rate | 55.74 | 34.75 | 0–469.23 |
| % college education | 56.27 | 11.65 | 2.70–100 |
| % unemployment | 6.26 | 2.30 | 1.20–23.70 |
| % single-parent households | 32.47 | 10.32 | 0–100 |
| Association rate | 13.83 | 6.78 | 0–81.30 |
| % severe housing problems | 14.47 | 4.86 | 2.18–71.26 |
| % aged 65 and over | 17.58 | 4.36 | 4.10–52.90 |
| % African American | 12.39 | 14.33 | 0–84.90 |
| Association rate | 13.83 | 6.78 | 0–81.30 |
| % female | 49.91 | 2.27 | 30.10–56.80 |
| % rural area | 58.82 | 31.50 | 0–100 |
| Mean county altitude (m) | 438.42 | 509.71 | −0.37–3473.11 |
| Model—With Mean County Altitude and Potential Covariates—R-Squared = 0.483, AIC Value: 14,432.13 | ||||
|---|---|---|---|---|
| Coefficient | S.E | t-Value | p-Value | |
| Intercept | 2.730 | 0.336 | 8.134 | 0.000 a |
| Mean county altitude | 0.004 | 0.000 | 40.691 | 0.000 a |
| % Smokers | 0.334 | 0.013 | 25.196 | 0.000 a |
| % aged 65 and over | 0.219 | 0.012 | 18.828 | 0.000 a |
| % African American | −0.036 | 0.004 | −10.093 | 0.000 a |
| Association rate | −0.0045 | 0.007 | −6.028 | 0.000 a |
| Model—With Mean County Altitude and Four Predictor Variables—R-Squared: 0.620, AIC Value: 13,593.68 | |||||
|---|---|---|---|---|---|
| Coefficient Range | Percentage of Counties by 95% of t Statistic | ||||
| Min. | Max. | t ≤ −1.96 | −1.96 < t < 1.96 | t ≥ 1.96 | |
| Intercept | −5.68 | 10.41 | 6.62 | 16.75 | 76.63 |
| Mean county altitude | −0.01 | 0.01 | 4.56 | 30.88 | 64.56 |
| % Smokers | 0.08 | 0.74 | 0.04 | 0 | 99.96 |
| % 65 and over | 0.11 | 0.31 | 0 | 0 | 100.00 |
| % African American | −0.50 | 0.07 | 61.95 | 36.75 | 1.30 |
| Association rate | −0.13 | 0.13 | 37.74 | 57.27 | 4.99 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, H.; Tu, W. An Ecological Study on the Spatially Varying Relationship between County-Level Suicide Rates and Altitude in the United States. Int. J. Environ. Res. Public Health 2018, 15, 671. https://doi.org/10.3390/ijerph15040671
Ha H, Tu W. An Ecological Study on the Spatially Varying Relationship between County-Level Suicide Rates and Altitude in the United States. International Journal of Environmental Research and Public Health. 2018; 15(4):671. https://doi.org/10.3390/ijerph15040671
Chicago/Turabian StyleHa, Hoehun, and Wei Tu. 2018. "An Ecological Study on the Spatially Varying Relationship between County-Level Suicide Rates and Altitude in the United States" International Journal of Environmental Research and Public Health 15, no. 4: 671. https://doi.org/10.3390/ijerph15040671
APA StyleHa, H., & Tu, W. (2018). An Ecological Study on the Spatially Varying Relationship between County-Level Suicide Rates and Altitude in the United States. International Journal of Environmental Research and Public Health, 15(4), 671. https://doi.org/10.3390/ijerph15040671