The Relationship between Household Sanitation and Women’s Experience of Menstrual Hygiene: Findings from a Cross-Sectional Survey in Kaduna State, Nigeria

 , , ,
, , ,
Abstract
:1. Introduction
The Present Study
2. Materials and Methods
2.1. Design and Participants
2.2. Study Context
2.3. Survey Measures
2.3.1. Household Questionnaire
2.3.2. Female Questionnaire
2.4. Analyses
2.5. Ethical Approval
3. Results
3.1. Participants and Sample Characteristics
3.2. Relationships between Household Sanitation and Menstrual Management Location
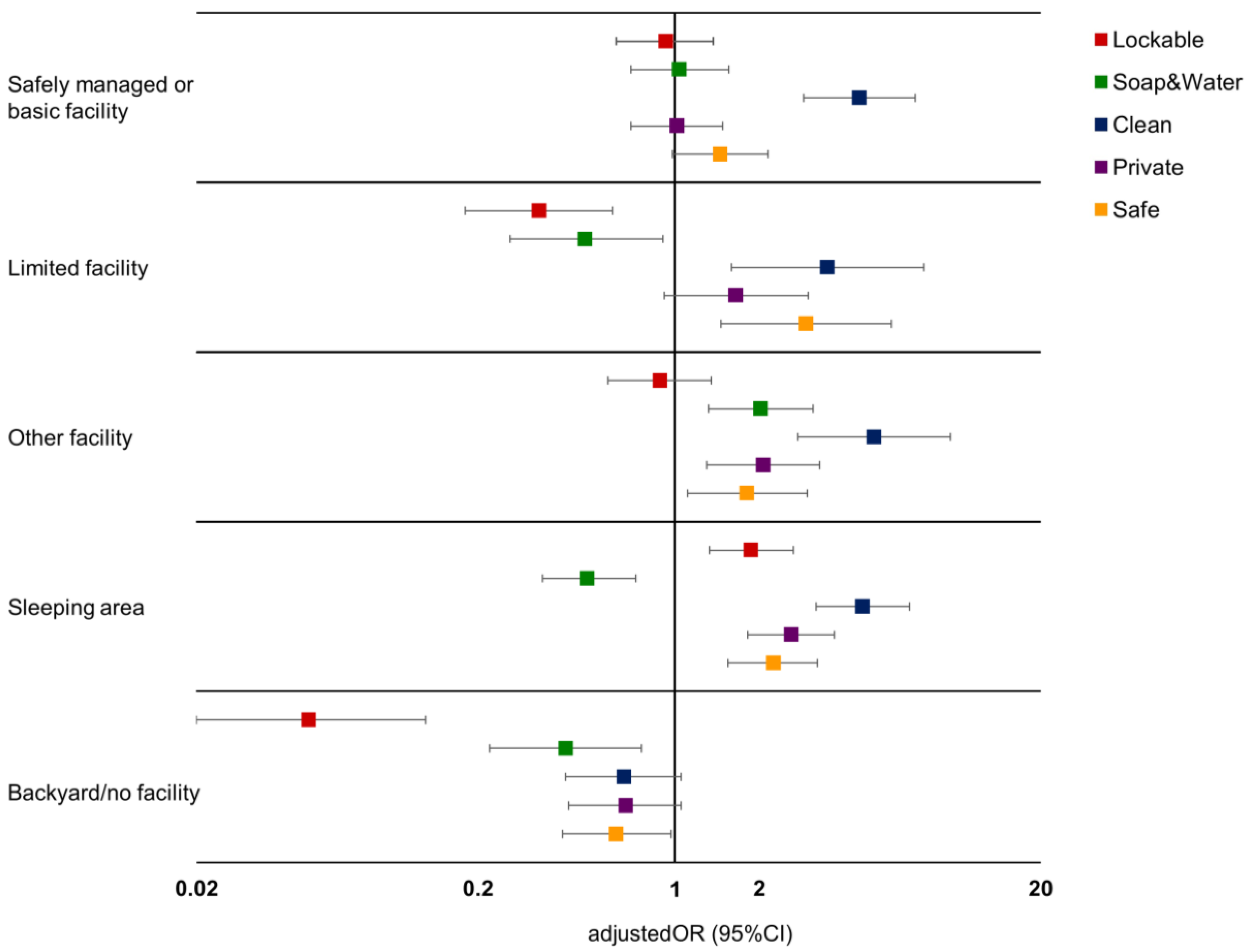
3.3. Relationships between Women’s Description of Their Menstrual Management Location
3.4. Women’s Perceptions of Their Menstrual Management Location
4. Discussion
4.1. Measures
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Statement
References
- Das, P.; Baker, K.K.; Dutta, A.; Swain, T.; Sahoo, S.; Das, B.S.; Panda, B.; Nayak, A.; Bara, M.; Bilung, B. Menstrual hygiene practices, wash access and the risk of urogenital infection in women from Odisha, India. PLoS ONE 2015, 10, e0130777. [Google Scholar] [CrossRef] [PubMed]
- Hennegan, J.; Dolan, C.; Steinfield, L.; Montgomery, P. A qualitative understanding of the effects of reusable sanitary pads and puberty education: Implications for future research and practice. Reprod. Health 2017, 14, 78. [Google Scholar] [CrossRef] [PubMed]
- Mason, L.; Nyothach, E.; Alexander, K.; Odhiambo, F.O.; Eleveld, A.; Vulule, J.; Rheingans, R.; Laserson, K.F.; Mohammed, A.; Phillips-Howard, P.A. ‘We keep it secret so no one should know’—A qualitative study to explore young schoolgirls attitudes and experiences with menstruation in rural Western Kenya. PLoS ONE 2013, 8, e79132. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.; Hirsch, J.S.; Nathanson, C.; Parker, R.G. Comfortably, safely, and without shame: Defining menstrual hygiene management as a public health issue. Am. J. Public Health 2015, 105, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Geertz, A.; Iyer, L.; Kasen, P.; Mazzola, F.; Peterson, K. An Opportunity to Address Menstrual Health and Gender Equity; Online; FSG: Boston, MA, USA, 2016. [Google Scholar]
- Sommer, M.; Sahin, M. Overcoming the taboo: Advancing the global agenda for menstrual hygiene management for schoolgirls. Am. J. Public Health 2013, 103, 1556–1559. [Google Scholar] [CrossRef] [PubMed]
- Hennegan, J.; Montgomery, P. Do menstrual hygiene management interventions improve education and psychosocial outcomes for women and girls in low and middle income countries? A systematic review. PLoS ONE 2016, 11, e0146985. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.A.; Winch, P.J.; Caruso, B.A.; Obure, A.F.; Ogutu, E.A.; Ochari, I.A.; Rheingans, R.D. ‘The girl with her period is the one to hang her head’ reflections on menstrual management among schoolgirls in rural Kenya. BMC Int. Health Hum. Rights 2011, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Chandra-Mouli, V.; Patel, S.V. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low- and middle-income countries. Reprod. Health 2017, 14, 30. [Google Scholar] [CrossRef] [PubMed]
- Miiro, G.; Rutakumwa, R.; Nakiyingi-Miiro, J.; Nakuya, K.; Musoke, S.; Namakula, J.; Francis, S.; Torondel, B.; Gibson, L.J.; Ross, D.A. Menstrual health and school absenteeism among adolescent girls in Uganda (MENISCUS): A feasibility study. BMC Women’s Health 2018, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Caruso, B.; Fehr, A.; Inden, K.; Sahin, M.; Ellis, A.; Andes, K.; Freeman, M. Wash in Schools Empowers Girls’ Education in Freetown, Sierra Leone: An Assessment of Menstrual Hygiene Management in Schools; UNICEF: New York, NY, USA, 2013. [Google Scholar]
- Haver, J.; Caruso, B.A.; Ellis, A.; Sahin, M.; Villasenor, J.M.; Andes, K.L.; Freeman, M.C. ‘Wash in Schools Empowers Girls’ Education in Masbate Province and Metro Manila, Philippines: An Assessment of Menstrual Hygiene Management in Schools’; UNICEF, Emory University: New York, NY, USA, 2013. [Google Scholar]
- Sommer, M. Where the education system and women’s bodies collide: The social and health impact of girls’ experiences of menstruation and schooling in tanzania. J. Adolesc. 2010, 33, 521–529. [Google Scholar] [CrossRef] [PubMed]
- van Eijk, A.M.; Sivakami, M.; Thakkar, M.B.; Bauman, A.; Laserson, K.F.; Coates, S.; Phillips-Howard, P.A. Menstrual hygiene management among adolescent girls in India: A systematic review and meta-analysis. BMJ Open 2016, 6, e010290. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.; Chandraratna, S.; Cavill, S.; Mahon, T.; Phillips-Howard, P.A. Managing menstruation in the workplace: An overlooked issue in low- and middle income countries. Int. J. Equity Health 2016, 15, 86. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.C.; Hulland, K.R.S.; Caruso, B.A.; Swain, R.; Freeman, M.C.; Panigrahi, P.; Dreibelbis, R. Sanitation-related psychosocial stress: A grounded theory study of women across the life-course in Odisha, India. Soc. Sci. Med. 2015, 139, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Henley, P.; Lowthers, M.; Koren, G.; Fedha, P.T.; Russell, E.; VanUum, S.; Arya, S.; Darnell, R.; Creed, I.F.; Trick, C.G. Cultural and socio-economic conditions as factors contributing to chronic stress in sub-Saharan African communities. Can. J. Physiol. Pharmacol. 2014, 92, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Hulland, K.R.S.; Chase, R.P.; Caruso, B.A.; Rojalin, S.; Bismita, B.; Sahoo, K.C.; Panigrahi, P.; Dreibelbis, R. Sanitation, stress, and life stage: A systematic data collection study among women in Odisha, India. PLoS ONE 2015, 10, e0141883. [Google Scholar] [CrossRef] [PubMed]
- WASH United; Simavi. Infographic MHM and SDGS. Available online: http://menstrualhygieneday.org/project/infographic-mhm-and-sdgs/ (accessed on 13 December 2017).
- World Health Organization (WHO); United Nations Children’s Fund (UNICEF). Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and Sdg Baselines; World Health Organization (WHO); United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2017. [Google Scholar]
- Khan, S.M.; Bain, R.E.; Lunze, K.; Unalan, T.; Beshanski-Pedersen, B.; Slaymaker, T.; Johnston, R.; Hancioglu, A. Optimizing household survey methods to monitor the sustainable development goals targets 6.1 and 6.2 on drinking water, sanitation and hygiene: A mixed-methods field-test in Belize. PLoS ONE 2017, 12, e0189089. [Google Scholar] [CrossRef] [PubMed]
- The Ministry of Drinking Water and Sanitation, Government of India. Menstrual Hygiene Management: National Guidelines; The Ministry of Drinking Water and Sanitation, Government of India: New Delhi, India, 2015. [Google Scholar]
- Loughnan, L.; Bain, R.; Rop, R.; Sommer, M.; Slaymaker, T. What can existing data on water and sanitation tell us about menstrual hygiene management? Waterlines 2016, 35, 228–244. [Google Scholar] [CrossRef]
- Sommer, M.; Figueroa, C.; Kwauk, C.; Jones, M.; Fyles, N. Attention to menstrual hygiene management in schools: An analysis of education policy documents in low-and middle-income countries. Int. J. Educ. Dev. 2017, 57, 73–82. [Google Scholar] [CrossRef]
- Zimmerman, L.; Olson, H.; Tsui, A.; Radloff, S. Pma2020: Rapid turn-around survey data to monitor family planning service and practice in ten countries. Stud. Fam. Plan. 2017, 48, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Centre for Research, Evaluation Resources and Development (CRERD); Bayero University Kano (BUK); Johns Hopkins Bloomberg School of Public Health (JHSPH). Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 2, PMA2015/Nigeria-R2 (Kaduna & Lagos) Nigeria; PMA2020: Baltimore, MD, USA, 2015. [Google Scholar]
- Kaduna State Government. About. 2018. Available online: https://kdsg.gov.ng/about-2/ (accessed on 16 February 2018).
- Kaduna State Government. Kaduna State Sustainable Development Goals Report 2017; Kaduna State Government: Kaduna, Nigeria, 2017. [Google Scholar]
- National Population Commission—NPC/Nigeria and ICF International. Nigeria Demographic and Health Survey 2013; NPC/Nigeria and ICF International: Abuja, Nigeria, 2014. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 15.1; StataCorp LP: College Station, TX, USA, 2018. [Google Scholar]
- Fisher, J. For Her It’s the Big Issue: Putting Women and the Centre of Water Supply, Sanitation and Hygiene; Water Supply and Sanitation Collaborative Council: Geneva, Switzerland, 2006. [Google Scholar]
- Reddy, B.; Snehalatha, M. Sanitation and personal hygiene: What does it mean to poor and vulnerable women? Indian J. Gend. Stud. 2011, 18, 381–404. [Google Scholar] [CrossRef]
- Bhakta, A.; Reed, B.; Fisher, J. Cleansing in hidden spaces: The bathign needs of perimenopausal women. In Proceedings of the 40th WEDC International Conference 2017, Loughborough, UK, 24–28 July 2017. [Google Scholar]
- Hennegan, J.; Dolan, C.; Wu, M.; Scott, L.; Montgomery, P. Measuring the prevalence and impact of poor menstrual hygiene management: A quantitative survey of schoolgirls in rural Uganda. BMJ Open 2016, 6, e012596. [Google Scholar] [CrossRef] [PubMed]
- Caruso, B.A.; Clasen, T.F.; Hadley, C.; Yount, K.M.; Haardörfer, R.; Rout, M.; Dasmohapatra, M.; Cooper, H.L. Understanding and defining sanitation insecurity: Women’s gendered experiences of urination, defecation and menstruation in rural Odisha, India. BMJ Glob. Health 2017, 2, e000414. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Main Household Facility | Other Sanitation Facility | Sleeping Area | Backyard/No Facility | Total | |
|---|---|---|---|---|---|
| (n = 962) | (n = 337) | (n = 521) | (n = 174) | (n = 1994) | |
| % | % | % | % | % | |
| Household sanitation (n = 1994) | |||||
| Safely managed/basic | 57.81 | 21.32 | 17.24 | 3.63 | 34.78 |
| Limited | 52.47 | 28.02 | 18.81 | 0.70 | 13.63 |
| Unimproved | 59.26 | 7.13 | 28.30 | 5.31 | 33.67 |
| Open defecation | 0.00 | 12.36 | 59.65 | 27.99 | 17.92 |
| Handwashing place (n = 1991) | |||||
| Yes | 52.38 | 25.99 | 17.50 | 6.12 | 28.92 |
| No | 44.94 | 12.59 | 33.46 | 9.02 | 71.08 |
| Age (n = 1994) | |||||
| 15–19 | 51.15 | 15.74 | 25.00 | 8.11 | 26.94 |
| 20–24 | 46.59 | 13.17 | 30.48 | 9.76 | 19.60 |
| 25–34 | 46.28 | 15.64 | 30.18 | 7.90 | 30.52 |
| 35 and older | 44.36 | 18.54 | 29.91 | 7.20 | 22.93 |
| Education (n = 1994) | |||||
| None | 57.24 | 4.70 | 28.45 | 9.61 | 35.68 |
| Primary school | 46.33 | 10.72 | 34.90 | 8.05 | 22.53 |
| Secondary school | 38.77 | 26.02 | 26.88 | 8.34 | 33.11 |
| Higher education | 40.53 | 36.20 | 21.48 | 1.79 | 8.68 |
| Marital status (n = 1991) | |||||
| Married or cohabitating | 49.53 | 12.42 | 29.81 | 8.24 | 73.41 |
| Divorced or widowed | 38.95 | 19.06 | 35.75 | 6.24 | 3.46 |
| Never married | 41.15 | 26.31 | 24.44 | 8.09 | 23.13 |
| Wealth quintile (n = 1994) | |||||
| 1 (lowest) | 44.85 | 4.18 | 39.92 | 11.05 | 17.29 |
| 2 | 56.62 | 5.19 | 24.87 | 13.32 | 20.34 |
| 3 | 48.23 | 6.89 | 34.53 | 10.36 | 17.71 |
| 4 | 43.84 | 21.69 | 31.62 | 2.85 | 20.29 |
| 5 (highest) | 43.88 | 31.84 | 18.82 | 5.46 | 24.37 |
| Rurality (n = 1994) | |||||
| Urban | 49.82 | 28.02 | 17.79 | 4.37 | 28.10 |
| Rural | 46.19 | 11.09 | 33.07 | 9.64 | 71.90 |
| Menstrual materials (n = 1969) | |||||
| Pads (and other items) | 41.62 | 30.42 | 21.77 | 6.19 | 29.06 |
| Cloth (and other items) | 49.83 | 8.43 | 32.08 | 9.66 | 59.46 |
| Pads & cloth | 50.24 | 15.62 | 30.02 | 4.12 | 8.85 |
| Other | 57.14 | 19.13 | 17.34 | 6.39 | 2.62 |
| Reuse menstrual materials (n = 1988) | |||||
| Yes | 51.18 | 9.39 | 30.38 | 9.05 | 67.80 |
| No | 38.76 | 29.42 | 25.70 | 6.13 | 32.20 |
| Main Household Facility (n = 962) | Other Sanitation Facility (n = 337) | |||
| OR (95%CI) | aOR (95%CI) | OR (95%CI) | aOR (95%CI) | |
| Household sanitation | ||||
| Safely managed/basic | 0.93 (0.71–1.23) | 1.76 (1.26–2.46) | 2.76 (1.81–4.22) | 1.22 (0.76–1.97) |
| Limited | 0.72 (0.51–1.02) | 1.63 (1.08–2.48) | 4.29 (2.63–6.98) | 1.70 (0.97–2.98) |
| Unimproved | 1.00 | 1.00 | 1.00 | 1.00 |
| Open defecation | - | - | 1.57 (0.96–2.56) | 1.85 (1.09–3.15) |
| Sleeping Area (n = 521) | Backyard/No Facility (n = 174) | |||
| OR (95%CI) | aOR (95%CI) | OR (95%CI) | aOR (95%CI) | |
| Household sanitation | ||||
| Safely managed/basic | 0.61 (0.44–0.85) | 0.57 (0.39–0.82) | 0.63 (0.33–1.19) | 0.38 (0.16–0.90) |
| Limited | 0.67 (0.45–1.01) | 0.59 (0.36–0.98) | 0.09 (0.02–0.37) | 0.03 (0.00–0.21) |
| Unimproved | 1.00 | 1.00 | 1.00 | 1.00 |
| Open defecation | 3.68 (2.65–5.11) | 3.56 (2.50–5.06) | 7.26 (4.61–11.44) | 9.86 (5.76–16.87) |
| Clean | Private | Safe | Lockable | Soap & Water | |
|---|---|---|---|---|---|
| Clean | 1.00 | ||||
| Private | 0.24 *** | 1.00 | |||
| Safe | 0.38 *** | 0.31 *** | 1.00 | ||
| Lockable | 0.17 *** | 0.24 *** | 0.16 *** | 1.00 | |
| Soap & Water | 0.12 *** | 0.11 *** | 0.01 | 0.37 *** | 1.00 |
| Clean | Private | Safe | Lockable | Soap & Water | |
|---|---|---|---|---|---|
| % | % | % | % | % | |
| Menstrual management location | |||||
| Safely managed/basic | 91.26 | 72.82 | 80.64 | 47.30 | 39.39 |
| Limited | 92.19 | 83.06 | 90.43 | 41.44 | 40.52 |
| Unimproved | 56.62 | 52.99 | 56.28 | 26.17 | 30.50 |
| Other sanitation facility | 91.43 | 86.60 | 86.82 | 60.10 | 62.64 |
| Sleeping area | 87.86 | 81.12 | 75.52 | 54.93 | 18.19 |
| No facility | 47.05 | 45.25 | 52.49 | 6.27 | 19.76 |
| Handwashing place | |||||
| Yes | 91.06 | 81.95 | 89.08 | 56.69 | 49.79 |
| No | 75.36 | 67.84 | 66.70 | 38.00 | 26.90 |
| Age | |||||
| 15–19 | 79.42 | 69.82 | 71.99 | 46.53 | 35.49 |
| 20–24 | 75.05 | 69.35 | 73.04 | 40.36 | 29.24 |
| 25–34 | 81.47 | 73.73 | 71.97 | 43.18 | 32.02 |
| 35+ | 82.38 | 74.13 | 76.20 | 43.22 | 37.22 |
| Education | |||||
| None | 69.84 | 58.39 | 64.21 | 24.34 | 23.47 |
| Primary school | 80.01 | 72.99 | 66.77 | 40.31 | 27.45 |
| Secondary school | 85.88 | 80.36 | 82.39 | 58.89 | 38.83 |
| Higher education | 97.86 | 92.58 | 91.40 | 72.43 | 71.33 |
| Marital status | |||||
| Married/cohabitating | 77.78 | 69.20 | 71.56 | 38.81 | 31.32 |
| Divorced/widowed | 74.62 | 81.49 | 74.57 | 54.66 | 29.49 |
| Never married | 87.22 | 79.26 | 77.91 | 56.96 | 41.61 |
| Wealth | |||||
| 1 (lowest) | 68.17 | 55.58 | 69.44 | 24.97 | 19.62 |
| 2 | 68.47 | 55.46 | 55.84 | 18.96 | 22.98 |
| 3 | 70.99 | 68.20 | 65.94 | 36.49 | 26.53 |
| 4 | 85.58 | 80.21 | 74.28 | 50.61 | 32.20 |
| 5 (highest) | 96.54 | 89.22 | 91.78 | 71.20 | 55.30 |
| Rurality | |||||
| Urban | 95.21 | 89.66 | 88.45 | 40.04 | 48.54 |
| Rural | 73.88 | 64.98 | 67.19 | 52.49 | 27.76 |
| Menstrual materials | |||||
| Pads (+other) | 96.24 | 85.53 | 88.82 | 63.05 | 48.19 |
| Cloth (+other) | 70.73 | 64.92 | 66.28 | 31.76 | 25.91 |
| Pads & cloth | 91.88 | 77.63 | 77.21 | 52.01 | 38.89 |
| Other | 70.44 | 65.91 | 50.20 | 64.48 | 34.80 |
| Reuse menstrual material | |||||
| Yes | 74.79 | 66.60 | 68.85 | 32.63 | 27.93 |
| No | 91.00 | 83.49 | 82.49 | 66.73 | 45.85 |
| Clean | Private | Safe | ||||
| OR (95%CI) | aOR (95%CI) | OR (95%CI) | aOR (95%CI) | OR (95%CI) | aOR (95%CI) | |
| Menstrual management location | ||||||
| Safely managed/basic | 7.72 (4.98–11.98) | 4.53 (2.87–7.16) | 2.07 (1.47–2.93) | 1.02 (0.70–1.48) | 2.18 (1.52–3.11) | 1.45 (0.98–2.15) |
| Limited | 11.48 (5.45–24.20) | 3.49 (1.59–7.67) | 6.09 (3.50–10.62) | 1.65 (0.92–2.98) | 7.16 (3.77–13.60) | 2.93 (1.46–5.89) |
| Unimproved | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Other sanitation facility | 11.18 (6.42–19.46) | 5.12 (2.74–9.56) | 5.89 (3.88–8.91) | 2.07 (1.30–3.28) | 3.53 (2.30–5.42) | 1.81 (1.11–2.96) |
| Sleeping area | 5.47 (3.79–7.90) | 4.66 (3.18–6.84) | 3.53 (2.53–4.94) | 2.60 (1.82–3.69) | 2.58 (1.83–3.63) | 2.24 (1.55–3.22) |
| No facility/field | 0.84 (0.55–1.28) | 0.66 (0.41–1.05) | 0.93 (0.62–1.41) | 0.67 (0.42–1.05) | 0.77 (0.50–1.17) | 0.62 (0.40–0.97) |
| Lockable | Soap & Water | |||||
| OR (95%CI) | aOR (95%CI) | OR (95%CI) | aOR (95%CI) | |||
| Menstrual management location | ||||||
| Safely managed/basic | 2.01 (1.40–2.88) | 0.93 (0.62–1.37) | 1.86 (1.27–2.72) | 1.04 (0.70–1.56) | ||
| Limited | 1.40 (0.90–2.16) | 0.33 (0.18–0.60) | 1.32 (0.83–2.11) | 0.48 (0.26–0.91) | ||
| Unimproved | 1.00 | 1.00 | 1.00 | 1.00 | ||
| Other sanitation facility | 3.21 (2.21–4.66) | 0.89 (0.58–1.35) | 4.55 (3.07–6.72) | 2.02 (1.32–3.10) | ||
| Sleeping area | 2.56 (1.85–3.52) | 1.87 (1.33–2.64) | 0.67 (0.45–0.98) | 0.49 (0.34–0.73) | ||
| No facility/field | 0.13 (0.06–0.30) | 0.05 (0.02–0.13) | 0.55 (0.32–0.93) | 0.41 (0.22–0.76) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hennegan, J.; Zimmerman, L.; Shannon, A.K.; Exum, N.G.; OlaOlorun, F.; Omoluabi, E.; Schwab, K.J. The Relationship between Household Sanitation and Women’s Experience of Menstrual Hygiene: Findings from a Cross-Sectional Survey in Kaduna State, Nigeria. Int. J. Environ. Res. Public Health 2018, 15, 905. https://doi.org/10.3390/ijerph15050905
Hennegan J, Zimmerman L, Shannon AK, Exum NG, OlaOlorun F, Omoluabi E, Schwab KJ. The Relationship between Household Sanitation and Women’s Experience of Menstrual Hygiene: Findings from a Cross-Sectional Survey in Kaduna State, Nigeria. International Journal of Environmental Research and Public Health. 2018; 15(5):905. https://doi.org/10.3390/ijerph15050905
Chicago/Turabian StyleHennegan, Julie, Linnea Zimmerman, Alexandra K. Shannon, Natalie G. Exum, Funmilola OlaOlorun, Elizabeth Omoluabi, and Kellogg J. Schwab. 2018. "The Relationship between Household Sanitation and Women’s Experience of Menstrual Hygiene: Findings from a Cross-Sectional Survey in Kaduna State, Nigeria" International Journal of Environmental Research and Public Health 15, no. 5: 905. https://doi.org/10.3390/ijerph15050905
APA StyleHennegan, J., Zimmerman, L., Shannon, A. K., Exum, N. G., OlaOlorun, F., Omoluabi, E., & Schwab, K. J. (2018). The Relationship between Household Sanitation and Women’s Experience of Menstrual Hygiene: Findings from a Cross-Sectional Survey in Kaduna State, Nigeria. International Journal of Environmental Research and Public Health, 15(5), 905. https://doi.org/10.3390/ijerph15050905