Active Ottumwa: Adapting Evidence-Based Recommendations to Promote Physical Activity in a Micropolitan New Destination Community

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Overview and Study Design
2.2. Study Foundation and Community Advisory Board
2.3. Study Population
2.4. Intervention
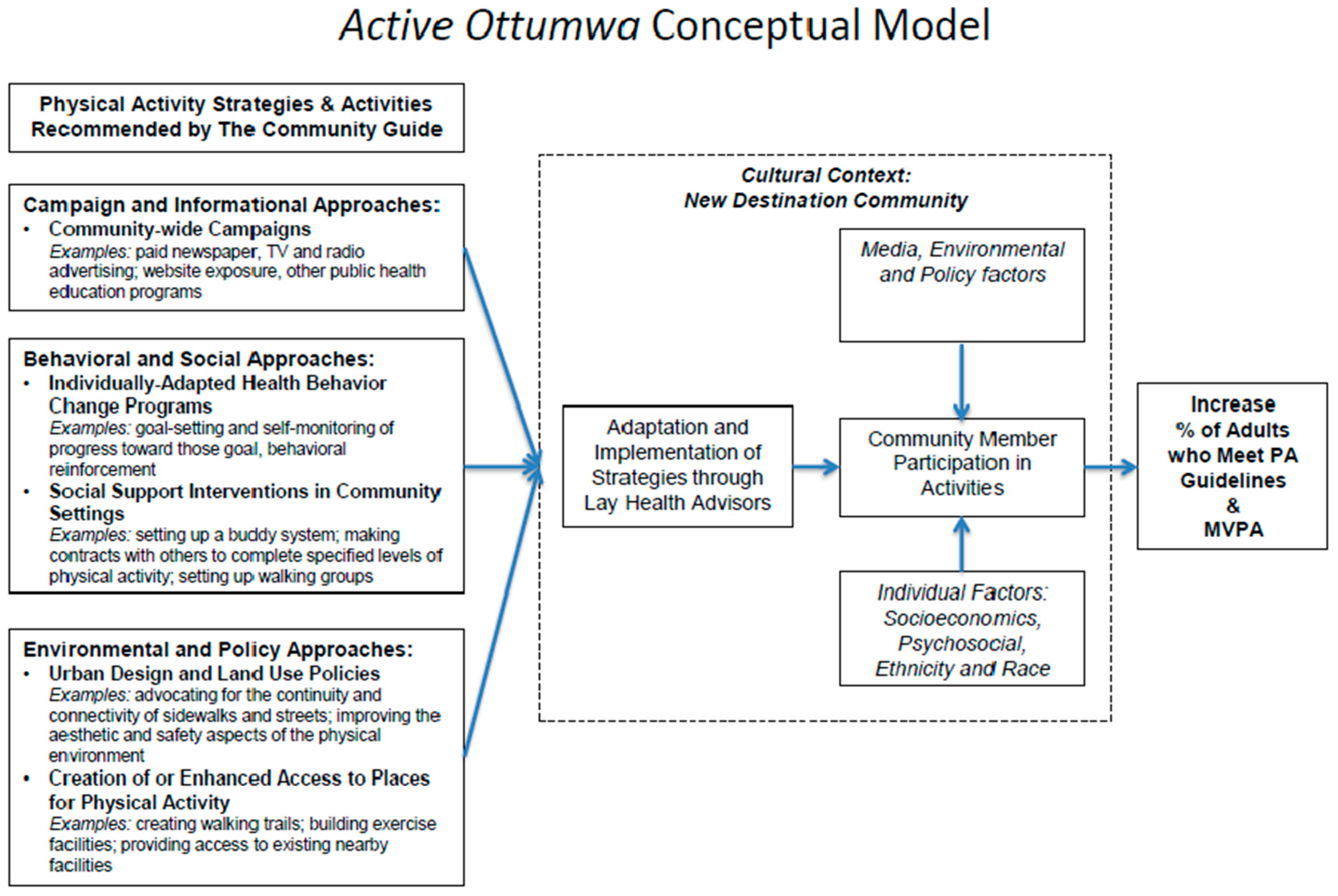
2.4.1. Evidence-Based Physical Activity Interventions
2.4.2. Adaptations
2.4.3. LHA Model
2.4.4. PAL Training and Support
2.4.5. Campaign and Informational Approaches
2.4.6. Environmental and Policy Approaches
2.5. Evaluation
Primary and Secondary Outcomes
2.6. Individual-Level Evaluation Procedures
2.6.1. Cross-Sectional Community Surveys
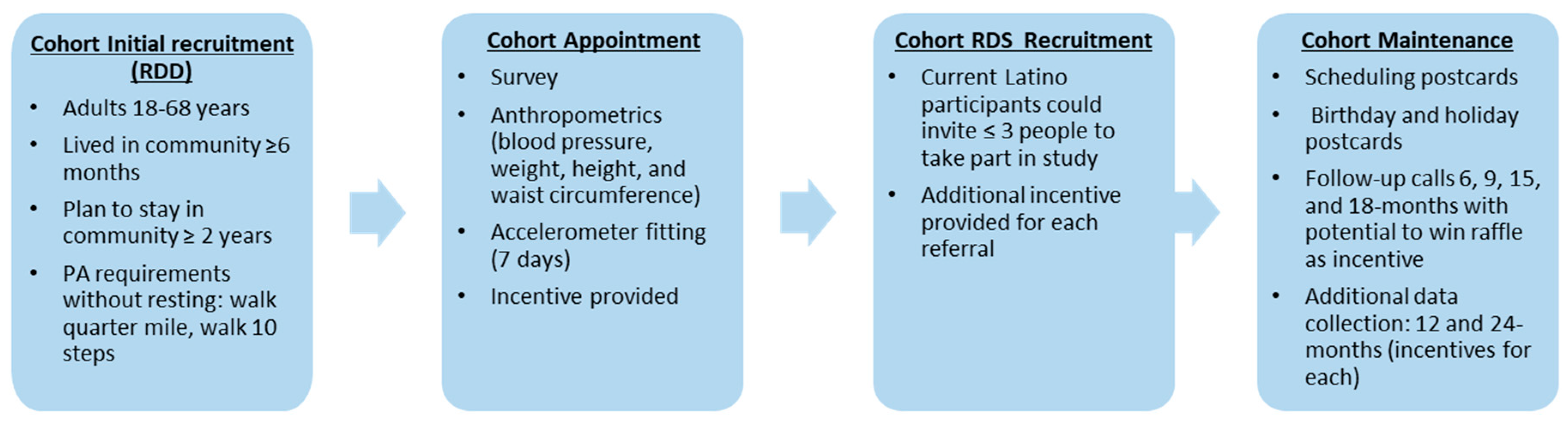
2.6.2. Longitudinal Cohort
2.7. Community Level Evaluation Procedures
2.7.1. System of Observing Play and Recreation in Communities (SOPARC)
2.7.2. Rural Active Living Assessment (RALA)
2.8. Planned Analysis
2.8.1. Cross-sectional Community Survey Data
2.8.2. Longitudinal Cohort Data
2.8.3. SOPARC Analysis
2.8.4. Qualitative Data Analysis of RALA Interviews
2.8.5. Intervention Implementation
2.9. Power Calculations
3. Results To Date
4. Discussion
4.1. Lessons Learned
4.1.1. Capacity and Resources of the Community to Implement the Intervention
4.1.2. Implementing Intervention Timeline
4.1.3. Supporting and Maintaining Physical Activity Leaders
4.1.4. Community Advisory Board Essential on the Adaptation and Implementation of Strategies
4.1.5. Validity of Measures for Micropolitan Rural Communities
4.1.6. Ethical Implications
4.2. Strengths and Limitations
4.3. Next Steps
4.3.1. Activate Active Ottumwa Ambassadors (AOAs)
4.3.2. Development of a Toolkit to Promote PA in Micropolitan Cities
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AO | Active Ottumwa |
| AOA | Active Ottumwa Ambassadors |
| CAB | Community advisory board |
| CBPR | Community-based participatory research |
| CGPS | Community Guide for Preventive Services |
| ISRC | Iowa Social Science Research Center |
| MVPA | Moderate to vigorous physical activity |
| PA | Physical activity |
| PAL | Physical activity leader |
| RALA | Rural Active Living Assessment |
| RDD | Random digit dial |
| RDS | Respondent driven sampling |
| REDCap | Research Electronic Data Capture |
| SOPARC | System of Observing Play and Recreation in Communities |
| UI PRC | University of Iowa Prevention Research Center |
Appendix A
| Timeline | ||||||
| Activities | 2015 | 2016 | 2017 | 2018 | 2019 | |
| Identify, recruit and train Physical Activity Leaders (PALs) | x | |||||
| Determine and adapt intervention strategies to Ottumwa | x | |||||
| Baseline, 12- and 24-month longitudinal cohort of measures | x | x | x | x | ||
| Observations of trail and parks usage (SOPARC) | x | |||||
| Assessment of physical activity city environment (RALA) | x | |||||
| Intervention implementation | x | x | ||||
| Cohort maintanance (repeated at 6, 12 and 18 months) | x | x | ||||
| 2018 Cross-sectional community survey | x | |||||
| Analysis and reporting (data analysis, reporting of results, Development of toolkit for use in other Iowa communities) | x | |||||
Appendix B
| Community-Wide Cross-Sectional Survey | Cohort Assessment | Community-Wide Cross-Sectional Survey | ||||
| Construct | Baseline | 12-Month Follow-Up | 24-Month Follow-Up | |||
| Health Related Quality of Life | ||||||
| Perceived overall health | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Physical and mental health | ✓ | ✓ | ||||
| Sleep | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Depression | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Health Care | ||||||
| Insurance | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Access to regular care | ✓ | ✓ | ✓ | ✓ | ||
| Past health conditions | ✓ | ✓ | ✓ | |||
| Alcohol and Drugs | ||||||
| Alcohol consumption | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Cigarettes and tobacco | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Vaping | ✓ | |||||
| Nutrition | ||||||
| Drink consumption | ✓ | ✓ | ||||
| Fast food consumption | ✓ | ✓ | ||||
| Fruit and vegetables | ✓ | |||||
| Water | ✓ | |||||
| Self-monitoring diet | ✓ | |||||
| Food security | ✓ | |||||
| Physical Activity | ||||||
| Vigorous activity at work | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Moderate activity at work | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Vigorous activity for recreation | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Moderate activity for recreation | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Activity during travel | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Sedentary behavior | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Park usage | ✓ | ✓ | ✓ | ✓ | ||
| Park identification | ✓ | ✓ | ✓ | |||
| Outcome Expectations | ||||||
| Physical activity outcome expectations | ✓ | ✓ | ||||
| Support for Physical Activity | ||||||
| Physical activity social support | ✓ | ✓ | ||||
| Environmental support | ✓ | |||||
| Self-efficacy | ||||||
| Physical activity self-efficacy | ✓ | ✓ | ||||
| Motivators | ||||||
| Motivators for physical activity | ✓ | ✓ | ||||
| Barriers | ||||||
| Barriers to physical activity | ✓ | ✓ | ||||
| Social Norms | ||||||
| Subjective norms | ✓ | ✓ | ||||
| Descriptive norms | ✓ | ✓ | ||||
| Costs of Physical Activity | ||||||
| Economic costs | ✓ | ✓ | ✓ | |||
| Perceptions | ||||||
| Parenting | ✓ | |||||
| Unintended Effects | ||||||
| Exercise injury | ✓ | ✓ | ✓ | |||
| Anthropometric Measures | ||||||
| Blood pressure | ✓ | ✓ | ✓ | ✓ | ||
| Weight | ✓ | ✓ | ✓ | ✓ | ||
| Height | ✓ | ✓ | ✓ | ✓ | ||
| Waist Circumference | ✓ | ✓ | ✓ | ✓ | ||
| Neighborhood Context | ||||||
| Social cohesion | ✓ | ✓ | ✓ | |||
| Aesthetics | ✓ | ✓ | ||||
| Safety | ✓ | ✓ | ||||
| Walkability | ✓ | ✓ | ||||
| Food environment | ✓ | ✓ | ||||
| Violence | ✓ | ✓ | ||||
| Community involvement | ✓ | |||||
| Neighborhood health priorities | ✓ | |||||
| Spatial stigma | ✓ | |||||
| Community Health | ||||||
| Health of community | ✓ | |||||
| Social Support | ||||||
| Social Support | ✓ | ✓ | ||||
| Psychosocial Stressors | ||||||
| Vigilance | ✓ | ✓ | ||||
| Discrimination | ✓ | ✓ | ||||
| Reasons for discrimination | ✓ | ✓ | ||||
| Acculturation | ||||||
| Latino/Hispanic background | ✓ | ✓ | ✓ | |||
| Generational and Immigration | ||||||
| Country of birth | ✓ | ✓ | ✓ | |||
| Time of residency in the U.S. | ✓ | ✓ | ✓ | |||
| Parents’ nationality | ✓ | ✓ | ✓ | |||
| Grandparents’ nationality | ✓ | |||||
| Contact with native county | ✓ | |||||
| Awareness of the Program | ||||||
| Results of AO messages | ✓ | ✓ | ✓ | ✓ | ||
References
- Centers for Disease Control and Prevention. Current Physical Activity Guidelines. Available online: https://www.cdc.gov/cancer/dcpc/prevention/policies_practices/physical_activity/guidelines.htm (accessed on 15 February 2018).
- Clark, T.; Norris, T.; Schiller, J.S. Early Release of Selected Estimates Based on Data from the 2016 National Health Interview Survey. National Center for Health Statistics, May 2017. Available online: https://www.cdc.gov/nchs/data/nhis/earlyrelease/earlyrelease201705.pdf (accessed on 16 February 2018).
- Nocon, M.; Hiemann, T.; Muller-Riemenschneider, F.; Thalau, F.; Roll, S.; Willich, S.N. Association of physical activity with all-cause and cardiovascular mortality: A systematic review and meta-analysis. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Reiner, M.; Niermann, C.; Jekauc, D.; Woll, A. Long-term health benefits of physical activity—A systematic review of longitudinal studies. BMC Public Health 2013, 13, 813. [Google Scholar] [CrossRef] [PubMed]
- Samitz, G.; Egger, M.; Zwahlen, M. Domains of physical activity and all-cause mortality: Systematic review and dose-response meta-analysis of cohort studies. Int. J. Epidemiol. 2011, 40, 1382–1400. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Frederick, S.M.; Thorpe, R.J.; Bell, C.N.; Bleich, S.N.; Ford, J.G.; LaVeist, T.A. Examination of Race Disparities in Physical Inactivity among Adults of Similar Social Context. Ethn. Dis. 2014, 24, 363–369. [Google Scholar] [PubMed]
- Neighbors, C.J.; Marquez, D.X.; Marcus, B.H. Leisure-time physical activity disparities among Hispanic subgroups in the United States. Am. J. Public Health 2008, 98, 1460–1464. [Google Scholar] [CrossRef] [PubMed]
- Parks, S.E.; Housemann, R.A.; Brownson, R.C. Differential correlates of physical activity in urban and rural adults of various socioeconomic backgrounds in the United States. J. Epidemiol. Community Health 2003, 57, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Brownson, R.C.; Smith, C.A.; Pratt, M.; Mack, N.E.; Jackson-Thompson, J.; Dean, C.G.; Dabney, S.; Wilkerson, J.C. Preventing cardiovascular disease through community-based risk reduction: The Bootheel Heart Health Project. Am. J. Public Health 1996, 86, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Lineger, J.M.; Chesson, C.V.; Nice, D.S. Physical fitness gains following simple environmental change. Am. J. Prev. Med. 1991, 7, 298–310. [Google Scholar] [CrossRef]
- Kriska, A.M.; Bayles, C.; Cauley, J.A.; LaPorte, R.E.; Sandler, R.B.; Pambianco, G. A randomized exercise trial in older women: Increased activity over two years and the factors associated with compliance. Med. Sci. Sports Exerc. 1986, 18, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Arredondo, E.M.; Elder, J.P.; Haughton, J.; Slymen, D.J.; Sallis, J.F.; Perez, L.G.; Serrano, N.; Parra, M.T.; Valdivia, R.; Ayala, G.X. Fe en Accion: Promoting Physical Activity Among Churchgoing Latinas. Am. J. Public Health 2017, 107, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X. San Diego Prevention Research Center Team. Effects of a promotor-based intervention to promote physical activity: Familias Sanas y Activas. Am. J. Public Health 2011, 101, 2261–2268. [Google Scholar] [CrossRef] [PubMed]
- Rowan, C.P.; Riddell, M.C.; Gledhill, N.; Jamnik, V.K. Community-Based Culturally Preferred Physical Activity Intervention Targeting Populations at High Risk for Type 2 Diabetes: Results and Implications. Can. J. Diabetes 2016, 40, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Richardson, N.; Carroll, P.; Harrison, M.; Donohoe, A.; Keohane, A.; Robertson, S.; Kelly, L. An investigation of a community based physical activity intervention for adult men, ‘Men on the Move’. Eur. J. Public Health 2017, 27. [Google Scholar] [CrossRef]
- Johnson, R.; Robertson, W.; Towey, M.; Stewart-Brown, S.; Clarke, A. Changes over time in mental well-being, fruit and vegetable consumption and physical activity in a community-based lifestyle intervention: A before and after study. Public Health 2017, 146, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Cadmus, L.; Patrick, M.B.; Maciejewski, M.L.; Topolski, T.; Belza, B.; Patrick, D.L. Community-based aquatic exercise and quality of life in persons with osteoarthritis. Med. Sci. Sports Exerc. 2010, 42, 8–15. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. Metropolitan and Micropolitan. Available online: https://www.census.gov/programs-surveys/metro-micro/about.html (accessed on 15 February 2018).
- Lichter, D.T.; Johnson, K.M. Immigrant Gateways and Hispanic Migration to New Destinations. Int. Migr. Rev 2009, 43, 496–518. [Google Scholar] [CrossRef]
- Matthews, K.A.; Croft, J.B.; Liu, Y.; Lu, H.; Kanny, D.; Wheaton, A.G.; Cunningham, T.J.; Khan, L.K.; Caraballo, R.S.; Holt, J.B.; et al. Health-related behaviors by urban-rural county classification–United States, 2013. MMWR Surveill. Summ. 2017, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wahl, A.M.G.; Breckenridge, R.S.; Gunkel, S.E. Latinos, residential segregation and spatial assimilation in micropolitan areas: Exploring the American dilemma on a new frontier. Soc. Sci. Res. 2007, 36, 995–1020. [Google Scholar] [CrossRef]
- Crowley, M.; Lichter, D.T. Social disorganization in new Latino destinations? Rural Sociol. 2010, 74, 573–604. [Google Scholar] [CrossRef]
- Eng, E.; Rhodes, S.; Parker, E. Natural helper models to enhance a community’s health and competence. In Emerging Theories in Health Promotion Practice and Research, 2nd ed.; DiClemente, R.J., Crosby, R., Kegler, M., Eds.; Jossey-Bass: San Francisco, CA, USA, 2009; pp. 126–156. [Google Scholar]
- Centers for Disease Control and Prevention. Winnable Battles. Available online: http://www.cdc.gov/winnablebattles/ (accessed on 8 August 2013).
- Community Preventive Services Task Force. Physical Activity. Available online: https://www.thecommunityguide.org/topic/physical-activity (accessed on 22 February 2018).
- Castro, F.G.; Barrera, J.M.; Martinez, J.C.R. The cultural adaptation of prevention interventions: Resolving tensions between fidelity and fit. Prev. Sci. 2004, 5, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Community-based participatory research: Policy recommendations for promoting a partnership approach in health research. Educ. Health 2001, 14, 182–197. [Google Scholar] [CrossRef]
- U.S. Census Bureau. QuickFacts: Ottumwa City, Iowa. Available online: https://www.census.gov/quickfacts/fact/table/ottumwacityiowa/PST045216 (accessed on 15 February 2018).
- U.S. Census Bureau. 2012–2016 American Community Survey 5-Year Estimates. Available online: https://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?pid=ACS_16_5YR_DP05&src=pt (accessed on 3 May 2018).
- Remington, P.L.; Catlin, B.B.; Gennuso, K.P. The County Health Rankings: Rationale and methods. Popul. Health Metr. 2015, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.M.; Cruz, T.H.; Hess, J.M.; Kozoll, R.; Page-Reeves, J. Implementing Physical Activity Recommendations in a Tri-Ethnic Rural Community through a Community-University Partnership. Prog. Community Health Partnersh. 2017, 11, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, P.A.; Burroughs, E.L.; Granner, M.L.; Wilcox, S.; Hutto, B.E.; Bryant, C.A.; Peck, L.; Pekuri, L. Impact of a Community-Based Prevention Marketing Intervention to Promote Physical Activity Among Middle-Aged Women. Health Educ. Behav. 2010, 37, 403–423. [Google Scholar] [CrossRef] [PubMed]
- Hartman, M.A.; Stronks, K.; Highfield, L.; Cremer, S.W.; Verhoeff, A.P.; Nierkens, V. Disseminating evidence-based interventions to new populations: A systematic approach to consider the need for adaptation. Implement. Sci. 2015, 10. [Google Scholar] [CrossRef]
- Cancer Prevention and Control Research Network. Putting Public Health Evidence in Action Training Workshop. Available online: http://cpcrn.org/pub/evidence-in-action/ (accessed on 26 April 2018).
- Israel, B.A. Social networks and social support: Implications for natural helper and community level interventions. Health Educ. Q. 1985, 12, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Eng, E.; Young, R. Lay health advisors as community change agents. Fam. Community Health 1992, 15, 24–40. [Google Scholar] [CrossRef]
- Rhodes, S.D.; Hergenrather, K.C.; Bloom, F.R.; Leichliter, J.S.; Montano, J. Outcomes from a community-based, participatory lay health adviser HIV/STD prevention intervention for recently arrived immigrant Latino men in rural North Carolina. AIDS Educ. Prev. 2009, 21, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Valente, T.W.; Pumpuang, P. Identifying opinion leaders to promote behavior change. Health Educ. Behav. 2007, 34, 881–896. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X.; Vaz, L.; Earp, J.A.; Elder, J.P.; Cherrington, A. Outcome effectiveness of the lay health advisor model among Latinos in the United States: An examination by role. Health Educ. Res. 2010, 25, 815–840. [Google Scholar] [CrossRef] [PubMed]
- Baker, E.A.; Bouldin, N.; Durham, M.; Lowell, M.E.; Gonzalez, M.; Jodaitis, N.; Cruz, L.N.; Torres, I.; Torres, M.; Adams, S.T. The Latino Health Advocacy Program: A collaborative lay health advisor approach. Health Educ. Behav. 1997, 24, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Beam, N.; Tessaro, I. The Lay Health Adviser Model in Theory and Practice–An Example of an Agency-Based Program. Fam. Community Health 1994, 17, 70–79. [Google Scholar] [CrossRef]
- Bird, J.A.; Otero-Sabogal, R.; Ha, N.-T.; McPhee, S.J. Tailoring Lay Health Worker Interventions for Diverse Cultures: Lessons Learned from Vietnamese and Latina Communities. Health Educ. Q. 2016, 23, 105–122. [Google Scholar] [CrossRef]
- Cherrington, A.; Ayala, G.X.; Amick, H.; Scarinci, I.; Allison, J.; Corbie-Smith, G. Applying the community health worker model to diabetes management: Using mixed methods to assess implementation and effectiveness. J. Health Care Poor Underserved 2008, 19, 1044–1059. [Google Scholar] [CrossRef] [PubMed]
- Earp, J.A.; Viadro, C.I.; Vincus, A.A.; Altpeter, M.; Flax, V.; Mayne, L.; Eng, E. Lay health advisors: A strategy for getting the word out about breast cancer. Health Educ. Behav. 1997, 24, 432–451. [Google Scholar] [CrossRef] [PubMed]
- McQuiston, C.; Flaskerud, J.H. “If they don’t ask about condoms, I just tell them”: A descriptive case study of Latino lay health advisers’ helping activities. Health Educ. Behav. 2003, 30, 79–96. [Google Scholar] [CrossRef] [PubMed]
- McQuiston, C.; Choi-Hevel, S.; Clawson, M. Protegiendo Nuestra Comunidad: Empowerment participatory education for HIV prevention. J. Transcult. Nurs. 2001, 12, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Tessaro, I.A.; Taylor, S.; Belton, L.; Campbell, M.K.; Benedict, S.; Kelsey, K.; DeVellis, B. Adapting a natural (lay) helpers model of change for worksite health promotion for women. Health Educ. Res. 2000, 15, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Altpeter, M.; Earp, J.A.; Bishop, C.; Eng, E. Lay health advisor activity levels: Definitions from the field. Health Educ. Behav. 1999, 26, 495–512. [Google Scholar] [CrossRef] [PubMed]
- Jackson, E.J.; Parks, C.P. Recruitment and training issues from selected lay health advisor programs among African Americans: A 20-year perspective. Health Educ. Behav. 1997, 24, 418–431. [Google Scholar] [CrossRef] [PubMed]
- Watkins, E.L.; Harlan, C.; Eng, E.; Gansky, S.A.; Gehan, D.; Larson, K. Assessing the effectiveness of lay health advisors with migrant farmworkers. Fam. Community Health 1994, 16, 72–87. [Google Scholar] [CrossRef]
- Valente, T.W. Social Networks and Health: Models, Methods, and Applications, 1st ed.; Oxford University Press: New York, NY, USA, 2010; ISBN 978-0195301014. [Google Scholar]
- Parker, E.A.; Schulz, A.J.; Israel, B.A.; Hollis, R. Detroit’s East Side Village Health Worker Partnership: Community-based lay health advisor intervention in an urban area. Health Educ. Behav. 1998, 25, 24–45. [Google Scholar] [CrossRef] [PubMed]
- Eng, E.; Parker, E. Measuring Community Competence in the Mississippi Delta: The Interface between Program Evaluation and Empowerment. Health Educ. Q. 2016, 21, 199–220. [Google Scholar] [CrossRef]
- Pew Research Center. Available online: http://www.pewresearch.org/methodology/u-s-survey-research/collecting-survey-data/ (accessed on 27 February 2018).
- Linnan, L.A.; Reiter, P.L.; Duffy, C.; Hales, D.; Ward, D.S.; Viera, A.J. Assessing and promoting physical activity in African American barbershops: Results of the FITStop pilot study. Am. J. Mens Health 2011, 5, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey Anthropometry Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2013-2014/manuals/2013_Anthropometry.pdf (accessed on 26 February 2018).
- Actigraph. GT3X+ Monitor. Available online: http://www.actigraphcorp.com/products/gt3x-monitor/ (accessed on 15 April 2013).
- Colley, R.C.; Garriguet, D.; Janssen, I.; Craig, C.L.; Clarke, J.; Tremblay, M.S. Physical activity of Canadian adults: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011, 22, 7–14. [Google Scholar] [PubMed]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, T.; Cohen, D. System for Observing Play and Recreation in Communities (SOPARC): Description and Procedures Manual. Available online: https://activelivingresearch.org/sites/default/files/SOPARC_Protocols.pdf (accessed on 13 February 2018).
- Kanters, M.; Bocarro, J.; McKenzie, T.; Suau, L.; Carlton, T. Systematic Observation of Physical Activity Using iSOPARC: An iPad Application for Research and Practice. Available online: https://activelivingresearch.org/sites/default/files/2014_iSOPARC_Kanters.pdf (accessed on 13 February 2018).
- Yousefian, A.; Hennessy, E.; Umstattd, M.R.; Economos, C.D.; Hallam, J.S.; Hyatt, R.R.; Hartley, D. Development of the Rural Active Living Assessment Tools: Measuring rural environments. Prev. Med. 2010, 50 (Suppl. S1), S86–S92. [Google Scholar] [CrossRef] [PubMed]
- SAS Institute Inc. SAS 9.1.3 Help and Documentation; SAS Institute Inc.: Cary, NC, USA, 2002–2004. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 2nd ed.; SAGE Publications: Thousand Oaks, CA, USA, 1998; ISBN 978-0803959408. [Google Scholar]
- NVivo Qualitative Data Analysis Software, version 10; QSR International Pty Ltd.: Melbourne, Australia, 2012.
- Troiano, R.P. Large-scale applications of accelerometers: New frontiers and new questions. Med. Sci. Sports Exerc. 2007, 39, 1501. [Google Scholar] [CrossRef] [PubMed]
- Dzewaltowski, D.A. Behavior change intervention research in community settings: How generalizable are the results? Health Prom. Int. 2004, 19, 235–245. [Google Scholar] [CrossRef]
- White, E.; Armstrong, B.K.; Saracci, R. Principles of Exposure Measurement in Epidemiology: Collecting, Evaluating and Improving Measures of Disease Risk Factors, 2nd ed.; Oxford University Press: Oxford, UK, 2008; ISBN 0191004928. [Google Scholar]
- Shelton, R.C.; Dunston, S.K.; Leoce, N.; Jandorf, L.; Thompson, H.S.; Crookes, D.M.; Erwin, D.O. Predictors of activity level and retention among African American lay health advisors (LHAs) from The National Witness Project: Implications for the implementation and sustainability of community-based LHA programs from a longitudinal study. Implement. Sci. 2016, 11, 41. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Activity | # of PALs Leading Activity 1 | Total Hours of Activity Offered | Total # of New Participants |
|---|---|---|---|
| Strength training | 4 | 42 | 269 |
| Tai Chi | 1 | 46 | 483 |
| Walking groups | 20 | 274 | 904 |
| Water aerobics | 2 | 50 | 489 |
| Yoga | 5 | 31 | 217 |
| Zumba/Dance Fitness | 3 | 41 | 175 |
| Other 2 | 11 | 80 | 429 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baquero, B.; Kava, C.M.; Ashida, S.; Daniel-Ulloa, J.; Laroche, H.H.; Haines, H.; Bucklin, R.; Maldonado, A.; Coronado Garcia, M.; Berto, S.; et al. Active Ottumwa: Adapting Evidence-Based Recommendations to Promote Physical Activity in a Micropolitan New Destination Community. Int. J. Environ. Res. Public Health 2018, 15, 917. https://doi.org/10.3390/ijerph15050917
Baquero B, Kava CM, Ashida S, Daniel-Ulloa J, Laroche HH, Haines H, Bucklin R, Maldonado A, Coronado Garcia M, Berto S, et al. Active Ottumwa: Adapting Evidence-Based Recommendations to Promote Physical Activity in a Micropolitan New Destination Community. International Journal of Environmental Research and Public Health. 2018; 15(5):917. https://doi.org/10.3390/ijerph15050917
Chicago/Turabian StyleBaquero, Barbara, Christine M. Kava, Sato Ashida, Jason Daniel-Ulloa, Helena H. Laroche, Heidi Haines, Rebecca Bucklin, Adriana Maldonado, Mayra Coronado Garcia, Sandy Berto, and et al. 2018. "Active Ottumwa: Adapting Evidence-Based Recommendations to Promote Physical Activity in a Micropolitan New Destination Community" International Journal of Environmental Research and Public Health 15, no. 5: 917. https://doi.org/10.3390/ijerph15050917
APA StyleBaquero, B., Kava, C. M., Ashida, S., Daniel-Ulloa, J., Laroche, H. H., Haines, H., Bucklin, R., Maldonado, A., Coronado Garcia, M., Berto, S., Sewell, D., Novak, N., Janz, K., Gates, C., & Parker, E. A. (2018). Active Ottumwa: Adapting Evidence-Based Recommendations to Promote Physical Activity in a Micropolitan New Destination Community. International Journal of Environmental Research and Public Health, 15(5), 917. https://doi.org/10.3390/ijerph15050917