1. Introduction
Atrazine is the second most widely used herbicide in the United States, primarily applied to corn and sorghum crops [
1]. Much of the concern about atrazine arises from its persistence in soil and its transport to surface and groundwater drinking water sources [
2], making it the most commonly detected pesticide in surface water sources in the United States and frequently detected in groundwater sources as well [
1,
3].
Atrazine is an endocrine disruptor [
1,
4,
5], and while some aspects of the toxic mechanisms are unclear, atrazine disrupts the hypothalamic-pituitary-gonadal axis by inhibiting luteinizing hormone production, increasing aromatase production, and disrupting ovarian function [
6,
7,
8,
9]. Low ecologically relevant doses of atrazine have been shown to decrease testosterone levels, reduce spermatogenesis, and alter gonad development in amphibians, leading sometimes to complete chemical feminization of male frogs [
10,
11]. Exposure to atrazine induces delayed puberty, decreased testosterone and increased estradiol levels, reduced sperm counts, and altered testis architecture [
8,
12,
13,
14,
15] among male rats and delayed puberty, lengthened estrous cycles, and decreased number of menstrual cycles [
9,
16] among females.
There is limited epidemiologic evidence of an effect of prenatal exposure to atrazine on adverse birth outcomes in humans. Winchester et al. [
17] observed a temporal association between atrazine application and birth defects in an ecologic study in the U.S. Two studies of births in the Midwest have found that increased atrazine levels in drinking water sources is associated with elevated odds of small for gestational age (SGA), with one indicating that the timing of exposure is critical for understanding this association [
18,
19]. Exposure to atrazine through contaminated drinking water has been associated with increased risk of preterm birth in Kentucky [
20] and four Midwestern states [
21]. In France, Chevrier et al. [
22] reported that the presence of atrazine biomarkers in maternal urine was associated with lower birth weight, length, and head circumference. A recent study found an association between atrazine and both preterm birth and very preterm births in Midwestern counties in which <10% of the population is using private well water [
21]. With the exception of the one prospective cohort study in France [
22], all previous epidemiological studies of atrazine and birth outcomes have relied on ecologic exposure estimates obtained retrospectively through environmental monitoring data.
The United States Environmental Protection Agency (USEPA) defines the legal limits for water contaminants and water testing schedules, as mandated in the Safe Drinking Water Act. The maximum contaminant level (MCL) for atrazine in drinking water is 3 µg/L [
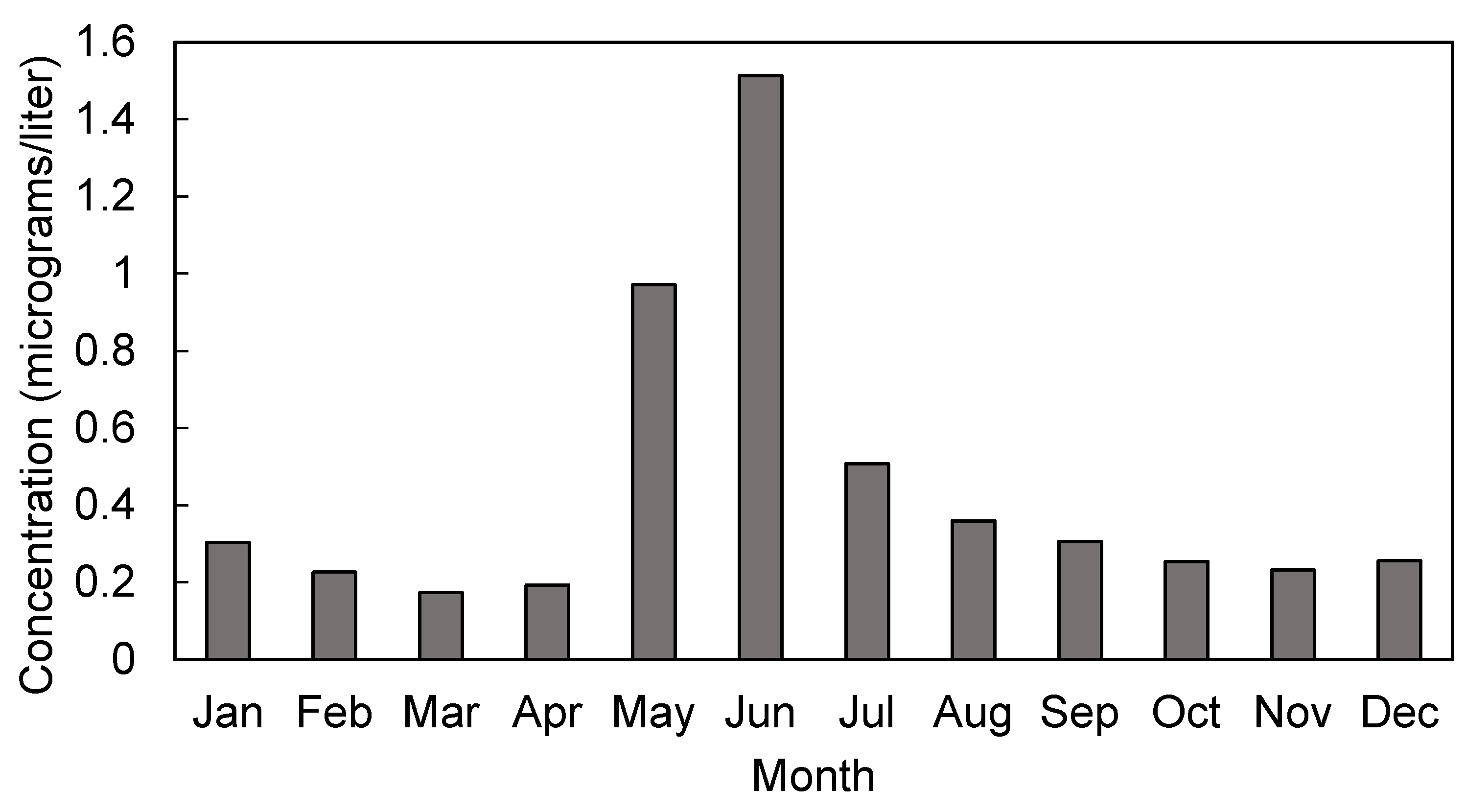
23]. Public water systems are required to test for atrazine quarterly, unless atrazine concentrations are consistently below the MCL, at which point testing can be reduced to once every three years. Those water systems that have atrazine or total combined triazine measurements exceeding 2.6 µg/L in finished water, or 12.5 µg/L in raw water, over a 90-day average are inducted into the Atrazine Monitoring Program (AMP) for 5 years. Community water systems (CWS) in the AMP are required to measure atrazine weekly during the season of peak atrazine use and biweekly throughout the remainder of the year [
24].
The primary objective of this study was to examine the association between atrazine concentrations in drinking water and selected adverse birth outcomes among those communities receiving drinking water from community water systems that were part of USEPA’s Atrazine Monitoring Program between 2006 and 2008 in the state of Ohio. This study also aimed to explore the utility of environmental and health data collected through routine monitoring by state and federal agencies for addressing epidemiologic questions, in line with the Centers for Disease Control and Prevention Environmental Public Health Tracking Program [
25].
4. Discussion
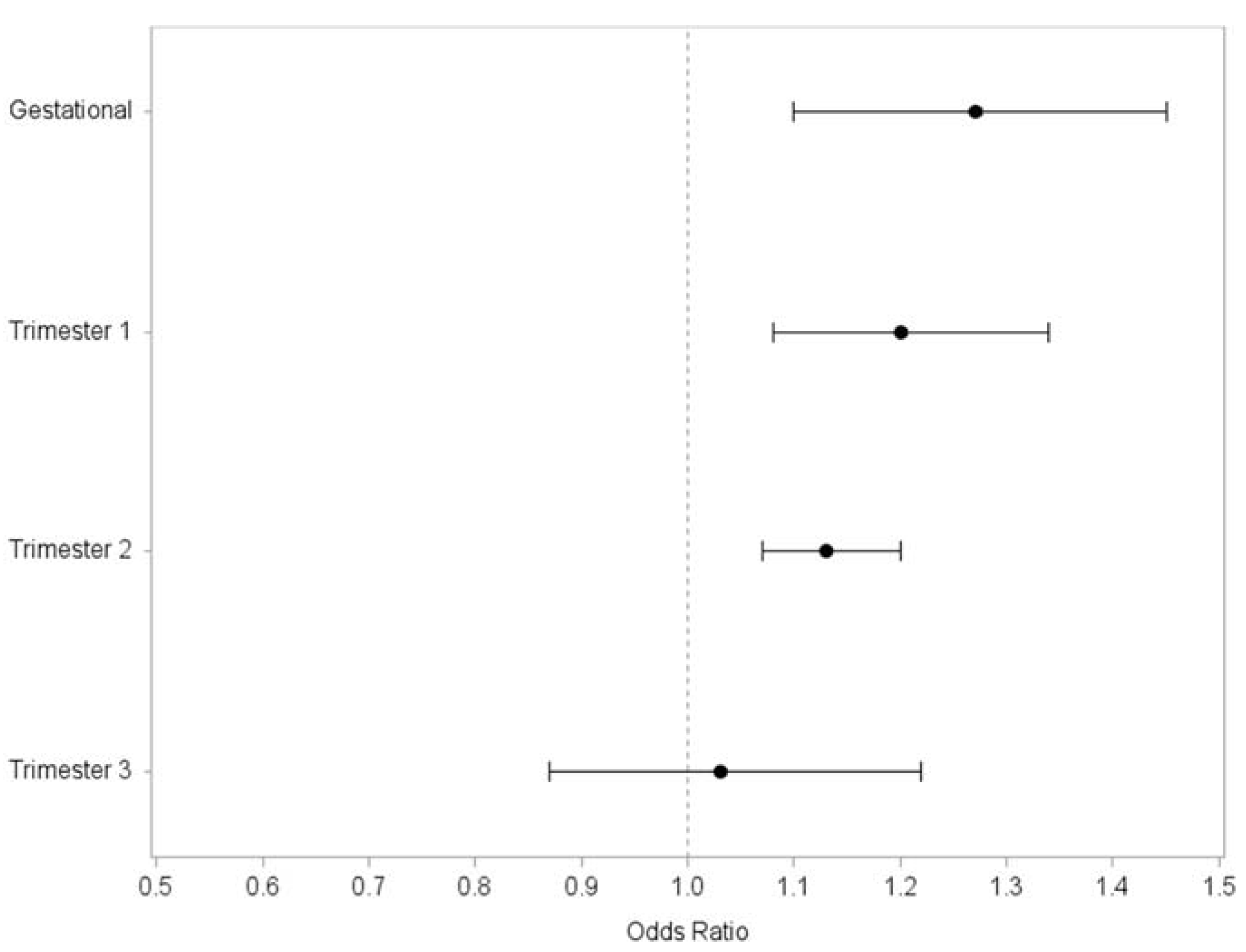
The aim of this study was to examine the relationship between atrazine exposure during pregnancy and selected adverse birth outcomes among communities that have been served by water systems monitored by the USEPA’s Atrazine Monitoring Program. Furthermore, this research was aimed at elucidating the window of exposure that is most critical for these birth outcomes. In this analysis of all live singleton births within AMP communities in Ohio between 2006 and 2008, we observed a significant increase in odds of term LBW births with increasing atrazine exposure. This association was observed within models of atrazine exposure averaged over the entire gestation of the pregnancy. Furthermore, our results suggest that atrazine exposure within the first and second trimesters of pregnancy, but not during the third trimester, are associated with term LBW, indicating that exposure to atrazine in drinking water in early and mid-pregnancy may be most critical for its toxic effects on the fetus. We observed no significant evidence of an association between atrazine exposure via drinking water and SGA, VLBW, PTB, or VPTB.
The exact mechanism through which atrazine would reduce birth weight is not well understood. Findings from rat models showing reduced pup weight after in utero exposure to atrazine lend biologic plausibility to our findings [
34,
35]. Our findings are consistent with previous epidemiologic research which has shown an inverse relationship between atrazine exposure and birth weight [
22], but conflicts with another study which found no association between atrazine exposure via drinking water and low birth weight in a population of infants in Brittany, France [
36]. While previous studies have shown evidence of an association between atrazine exposure and small for gestational age and preterm birth [
21], we found no evidence of these associations in our study of singleton births occurring within communities served by AMP water systems in Ohio from 2006 to 2008.
Reduced birth weight has serious public health impacts. The risk of neonatal mortality is highest among the smallest and largest infants, as measured by birth weight. This same pattern of increased risk is seen later in life as well, with a reversed “J” shape association between birthweight and cardiovascular disease and all-cause mortality [
26]. Our findings suggest that the morbidity and mortality burden from this adverse birth outcome can be lessened through reducing gestational exposures to atrazine in drinking water.
Water systems are enrolled in the AMP as a result of repeated exceedances of the 3 µg/L MCL for atrazine, but only 4% of samples from the water systems in this study exceeded the MCL. Our findings are unchanged when we remove those observations for which gestational atrazine estimates exceeded the MCL. While further epidemiologic research is needed, these results suggest that the current MCL for atrazine may not be protective against some adverse birth outcomes such as term low birth weight.
Most previous epidemiologic studies of atrazine and birth outcomes have been limited by ecologic exposure and outcome assessment. In the present study, birth outcomes and covariates were assessed at the individual level from birth certificates, providing more accurate outcome ascertainment and robust control of confounding. Atrazine exposure was estimated at the water system level in this study, which offers substantial refinement of exposure classification from the ecologic measurements that combine observations across multiple CWSs used in some of the prior studies [
18,
20,
36]. Furthermore, the sampling frame under the USEPA’s Atrazine Monitoring Program is more intensive than the frame for low-risk CWSs, which allows more robust determination of monthly atrazine concentrations and minimizes the number of months missing data in this analysis. Despite the reduction in exposure misclassification by estimating atrazine for each unique water system, we remain unable to account for personal drinking water behaviors (e.g., use of bottled water or filters), which can substantially influence an individual’s exposure. We lacked data on atrazine exposure from other sources such as diet, although atrazine residue is not often detected on food products and is not considered to be a significant contributor to overall atrazine exposure in the general population [
37]. Furthermore, this study assessed the relationship between exposure to one contaminant and multiple birth outcomes, which does not address the fact that drinking water contains varying levels of multiple contaminants.
We made an assumption that the service boundaries of the AMP water systems in this study corresponded to the geographic boundaries of the city in which each was located. For nearly half of these water systems, we received verbal confirmation from treatment plant operators and water system managers that this was in fact the case. We performed a sensitivity analysis by restricting the gestational atrazine models to only these confirmed water systems to attempt to further reduce exposure misclassification. In this sub-group analysis, we saw consistent magnitude and direction of association between atrazine and term low birth weight compared with the full sample, but lacked sufficient numbers to detect a significant increase in odds of this rare outcome.
Our outcome and covariate data originated from birth certificates. The reliability of birth certificate data, however, varies widely by data element. Overall, the Ohio birth certificate data contained low levels (<3%) of missing data on the key covariates used in these analyses. A notable exception is the high level of missing data on prenatal care (26%). Those who were missing data on their prenatal care status were more likely to be non-Hispanic black, “Other” race/ethnicity, and young. We chose to only use those covariates that are considered to be well-reported and highly accurate on birth certificates, such as maternal age, race/ethnicity, marital status, parity, plurality, infant gender, birth weight, and gestational age [
38,
39,
40,
41,
42,
43,
44,
45].
We lacked information on whether or not the mothers of the infants in these analyses had moved at any point during their pregnancy and assumed that the residence listed on the birth certificate was the residence throughout the entire pregnancy. Rates of pregnancy mobility are estimated between 12 and 32% [
46,
47,
48,
49], and vary by geography and demographic factors.
Our study was restricted to a small percentage of births (3%) in the state of Ohio for this analysis of AMP water systems. The population in these AMP communities differed from the state population in important ways. A much higher percentage of infants were born to mothers who were non-Hispanic white (86%) compared to the state as a whole (76%). Additionally, these AMP communities had a higher proportion of births from women enrolled in WIC (50% versus 42%) and who reported smoking (35% versus 26%). The small sample size relative to the state population and the demographic differences between the AMP communities and the state as a whole limit the generalizability of the study results. Ideally, future research on the association between atrazine in drinking water and adverse birth outcomes would include a representative sample of births to increase the generalizability of study findings.
Despite these limitations, the study had several notable strengths. The exposure estimates used in this study are highly geographically and temporally refined, which allowed specific exposure windows, such as trimesters, to be examined. The large number of births included in this study allowed the examination of two rare outcomes, very preterm birth and very low birth weight, which have not been reported previously. Furthermore, this study also benefited from individual-level data on important covariates.
Our findings suggest that additional epidemiologic research should examine the reproductive effects of exposure to atrazine in areas of relatively low contaminant exposure. Ideally, future research would employ biomarkers of exposure or individual assessment of drinking water exposures rather than relying on the ecologic exposure measures presented in these analyses. Despite the limitations in the exposure ascertainment, our findings demonstrate that linking environmental monitoring data with health outcomes data, such as vital statistics databases, holds promise for identifying potential associations, which can subsequently be investigated using with more refined exposure and outcome ascertainment.




{kind=link}
{kind=link}