Decomposing Income-Related Inequalities in Self-Reported Depression and Self-Rated Health Among Married Immigrants in South Korea

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Study Sample
2.2. Variables
2.2.1. Dependent Health Variables
2.2.2. Demographic and Socio-Economic Variables
2.3. Statistical Analysis
2.3.1. Concentration Index
2.3.2. Erreygers CI: Corrected Concentration Index
2.3.3. Decomposition of the Erreygers CI
3. Results
3.1. Sample Characteristics and Prevalence of Self-Reported Depression/Poor SRH
3.2. Income-Related Inequality in the Prevalence of Self-Reported Depression and Poor SRH
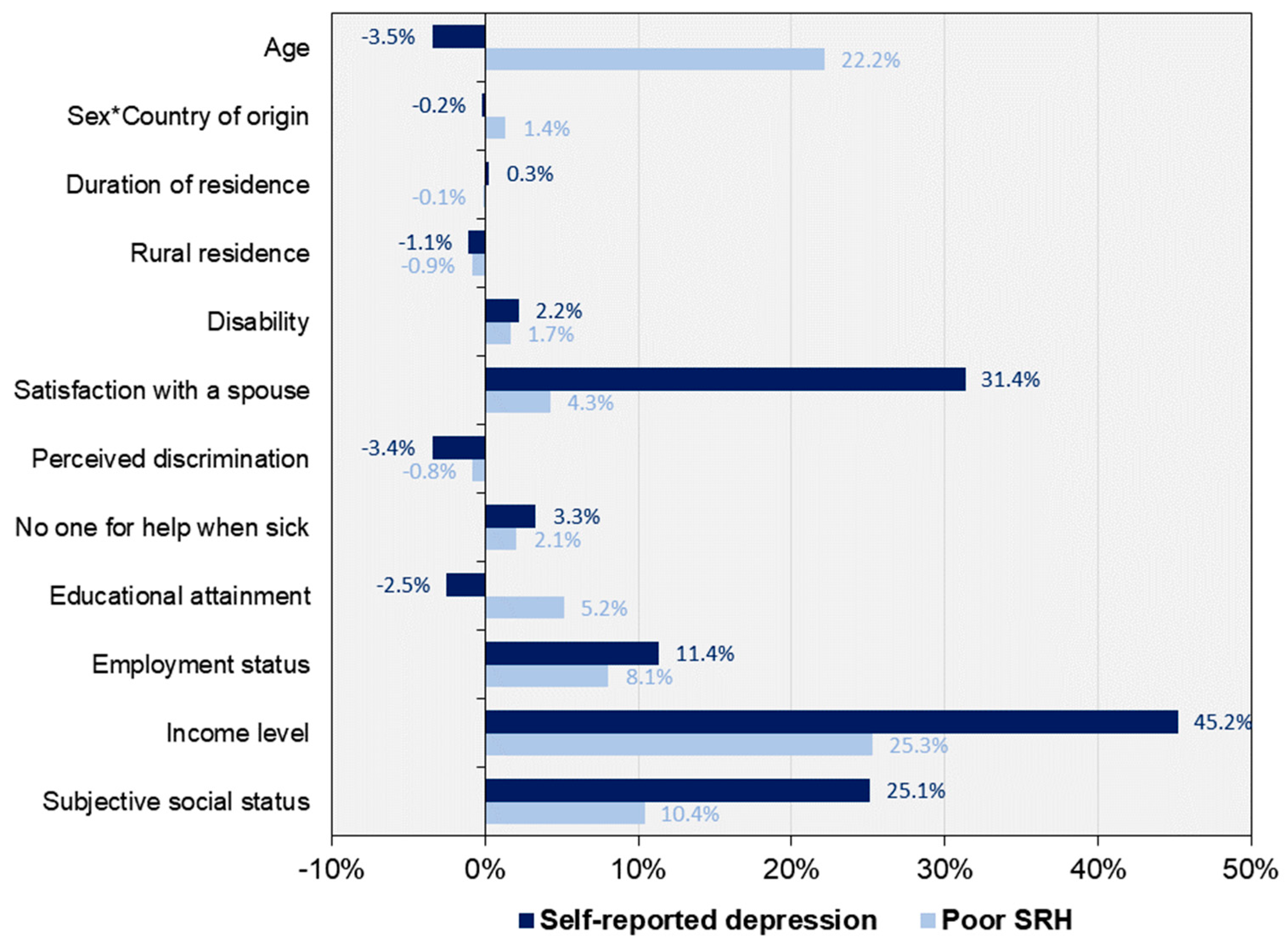
3.3. Decomposition of the Erreygers CI into Contributing Factors
4. Discussion
4.1. Income-Related Inequality in the Prevalence of Self-Reported Depression and Poor SRH among Married Immigrants
4.2. Decomposing Income-Related Health Inequality into Its Determinants
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations. International Migration Report 2017: Highlights (ST/ESA/SER.A/404); United Nations: New York, NY, USA, 2017. [Google Scholar]
- Korea Immigration Service. 1998–2017 Korea Immigragtion Service Statistics. Available online: http://www.index.go.kr/potal/main/EachDtlPageDetail.do?idx_cd=2756 (accessed on 1 February 2019).
- National Statistical Office. Population Trends. Available online: http://kosis.kr/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ZTITLE&parmTabId=M_01_01&parentId=A.1;A2.2;#A2.2 (accessed on 20 February 2019).
- D’Aoust, A.-M. Circulation of Desire: The Security Governance of the International ‘Mail-Order Brides’ Industry. In Security and Global Governmentality: Globalization, Governance and the State; de Larrinaga, M., Doucet, M.G., Eds.; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Kim, K.; Piper, N. Marriage migration in Southeast and East Asia revisited through a migration-development nexus lens AU—Chung, Chinsung. Crit. Asian Stud. 2016, 48, 463–472. [Google Scholar]
- Lee, Y.; Park, S. The mental health of married immigrant women in South Korea and its risk and protective factors: A literature review. Int. J. Soc. Psychiatry 2018, 64, 80–91. [Google Scholar] [CrossRef]
- Delara, M. Social Determinants of Immigrant Women’s Mental Health. Advan. Public Health 2016, 2016, 1–11. [Google Scholar] [CrossRef]
- Jeong, H.S.; Kim, Y.S.; Lee, T.M.; Ma, K.H.; Choi, Y.J.; Park, G.P.; Dong, J.Y.; Hwang, J.M.; Lee, E.A. A National Survey on Multicultural Families 2015 (No. 2016-03) (in Korean); Korean Women’s Development Institute: Seoul, Korea, 2016. [Google Scholar]
- Ministry of Health and Welfare; Korea Centers for Disease Control & Prevention. Population Health Statistics—The 2017 Korea National Health and Nutrition Examination Survey. Available online: http://www.index.go.kr/unify/idx-info.do?idxCd=4037 (accessed on 20 February 2019).
- Nazroo, J.Y. The structuring of ethnic inequalities in health: Economic position, racial discrimination, and racism. Am. J. Public Health 2003, 93, 277–284. [Google Scholar] [CrossRef]
- Nazroo, J.Y. Genetic, Cultural or Socio-economic Vulnerability? Explaining Ethnic Inequalities in Health. Sociol. Health Illn. 1998, 20, 710–730. [Google Scholar]
- Mangalore, R.; Knapp, M. Income-related inequalities in common mental disorders among ethnic minorities in England. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 351–359. [Google Scholar] [CrossRef]
- Shao, C.; Meng, X.; Cui, S.; Wang, J.; Li, C. Income-related health inequality of migrant workers in China and its decomposition: An analysis based on the 2012 China Labor-force Dynamics Survey data. J. Chin. Med. Assn. JCMA 2016, 79, 531–537. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, S.V.; Huijts, T.; Avendano, M. Self-reported health assessments in the 2002 World Health Survey: How do they correlate with education? Bull. World Health Organ. 2010, 88, 131–138. [Google Scholar] [CrossRef]
- Pérez-Zepeda, M.U.; Belanger, E.; Zunzunegui, M.-V.; Phillips, S.; Ylli, A.; Guralnik, J. Assessing the Validity of Self-Rated Health with the Short Physical Performance Battery: A Cross-Sectional Analysis of the International Mobility in Aging Study. PLoS ONE 2016, 11, e0153855. [Google Scholar] [CrossRef]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef]
- Mahoney, J.; Drinka, T.J.K.; Abler, R.; Gunter-Hunt, G.; Matthews, C.; Gravenstein, S.; Carnes, M. Screening for Depression: Single Question Versus GDS. J. Am. Geriatrics Soc. 1994, 42, 1006–1008. [Google Scholar]
- Hong, J. Effects of Ethnic Identity on the Relationship Between Mental Health and Perceived Discrimination Among Ethnic Return Migrants: The Case of Korean Chinese Return-Migrated to South Korea. J. Immigrant Minority Health/Cen. Minority Public Health 2019, 21, 522–532. [Google Scholar] [CrossRef]
- Krieger, N.; Smith, K.; Naishadham, D.; Hartman, C.; Barbeau, E.M. Experiences of discrimination: Validity and reliability of a self-report measure for population health research on racism and health. Soc. Sci. Med. 2005, 61, 1576–1596. [Google Scholar] [CrossRef] [Green Version]
- OECD. Purchasing Power Parities (PPP) (Indicator). Available online: https://data.oecd.org/conversion/purchasing-power-parities-ppp.htm (accessed on 8 February 2019).
- OECD. Exchange Rates (Indicator). Available online: https://data.oecd.org/conversion/exchange-rates.htm#indicator-chart (accessed on 8 February 2019).
- World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 20 February 2019).
- Van Doorslaer, E.; Koolman, X. Explaining the differences in income-related health inequalities across European countries. Health Econ. 2004, 13, 609–628. [Google Scholar] [CrossRef]
- Wagstaff, A.; Paci, P.; van Doorslaer, E. On the measurement of inequalities in health. Soc. Sci. Med. 1991, 33, 545–557. [Google Scholar] [CrossRef] [Green Version]
- Van Doorslaer, E.; Koolman, X.; Jones, A.M. Explaining income-related inequalities in doctor utilisation in Europe. Health Econ. 2004, 13, 629–647. [Google Scholar] [CrossRef]
- Erreygers, G. Correcting the concentration index. J. Health Econ. 2009, 28, 504–515. [Google Scholar] [CrossRef]
- Erreygers, G.; Clarke, P.; Van Ourti, T. “Mirror, mirror, on the wall, who in this land is fairest of all?”—Distributional sensitivity in the measurement of socioeconomic inequality of health. J. Health Econ. 2012, 31, 257–270. [Google Scholar] [CrossRef]
- Wagstaff, A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 2005, 14, 429–432. [Google Scholar] [CrossRef]
- Wagstaff, A.; van Doorslaer, E.; Watanabe, N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J. Econ. 2003, 112, 207–223. [Google Scholar] [CrossRef] [Green Version]
- StataCorp. Stata Statistical Software: Release 12; StataCorp LP: College Station, TX, USA, 2007. [Google Scholar]
- Van de Poel, E.; Van Doorslaer, E.; O’Donnell, O. Measurement of inequity in health care with heterogeneous response of use to need. J. Health Econ. 2012, 31, 676–689. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, O.; O’Neill, S.; Van Ourti, T.; Walsh, B. Conindex: Estimation of concentration indices. Stata J. 2016, 16, 112–138. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. The Korea National Health and Nutrition Examination Survey—Statistical Information Report; Ministry of Health and Welfare: Sejong, Korea, 2017.
- Wiking, E.; Johansson, S.E.; Sundquist, J. Ethnicity, acculturation, and self reported health. A population based study among immigrants from Poland, Turkey, and Iran in Sweden. J. Epidemiol. Community Health 2004, 58, 574–582. [Google Scholar] [CrossRef] [Green Version]
- Blázquez, M.; Cottini, E.; Herrarte, A. The socioeconomic gradient in health: How important is material deprivation? J. Econ. Inequality 2013, 12, 239–264. [Google Scholar] [CrossRef]
- Tøge, A.G.; Bell, R. Material deprivation and health: A longitudinal study. BMC Public Health 2016, 16, 747. [Google Scholar] [CrossRef]
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef] [Green Version]
- Tyhurst, L. Displacement and migration. A study in social psychiatry. Am. J. Psychiatry 1951, 107, 561–568. [Google Scholar] [CrossRef]
- Beiser, M. The health of immigrants and refugees in Canada. Can. J. Publ. Health-Rev. Can. San. 2005, 96 (Suppl. 2), S30–S44. [Google Scholar]
- Hahn, R.A.; Truman, B.I. Education Improves Public Health and Promotes Health Equity. Int. J. Health Serv.: Plan. Admin. Eval. 2015, 45, 657–678. [Google Scholar] [CrossRef]
- Acevedo-Garcia, D.; Sanchez-Vaznaugh, E.V.; Viruell-Fuentes, E.A.; Almeida, J. Integrating social epidemiology into immigrant health research: A cross-national framework. Soc. Sci. Med. 2012, 75, 2060–2068. [Google Scholar] [CrossRef]
- Chang, H.C.; Wallace, S.P. Migration processes and self-rated health among marriage migrants in South Korea. Ethn. Health 2016, 21, 20–38. [Google Scholar] [CrossRef]
- Zsembik, B.A.; Fennell, D. Ethnic variation in health and the determinants of health among Latinos. Soc. Sci. Med. 2005, 61, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.-Y.; Byoun, S.-J. Domestic violence against migrant women in South Korea: Addressing the needs of a uniquely situated victim population in domestic violence policy. Int. Soc. Work 2012, 57, 645–660. [Google Scholar] [CrossRef]
- Cabieses, B.; Cookson, R.; Espinoza, M.; Santorelli, G.; Delgado, I. Did Socioeconomic Inequality in Self-Reported Health in Chile Fall after the Equity-Based Healthcare Reform of 2005? A Concentration Index Decomposition Analysis. PLoS One 2015, 10, e0138227. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Depression | No Depression | Poor SRH | No Poor SRH |
|---|---|---|---|---|
| Age, % | ||||
| ≤34 | 37.4 | 62.6 | 3.2 | 96.8 |
| 35–49 | 32.8 | 67.2 | 8.9 | 91.1 |
| 50–64 | 30.2 | 69.8 | 21.0 | 79.0 |
| ≥65 | 40.5 | 59.5 | 54.8 | 45.2 |
| Sex and Country of origin, % | ||||
| Women from LMI countries | 37.0 | 63.0 | 8.9 | 91.1 |
| Women from HI countries | 31.2 | 68.8 | 8.7 | 91.3 |
| Men from LMI countries | 27.1 | 72.9 | 14.5 | 85.5 |
| Men from HI countries | 23.0 | 77.0 | 5.0 | 95.0 |
| Years of residence, mean (SD) | 9.56 (6.02) | 10.17 (6.88) | 12.52 (7.42) | 9.69 (6.45) |
| Rural residence, % | 34.2 * | 65.8 * | 6.4 | 93.6 |
| Urban residence, % | 34.8 * | 65.2 * | 10.4 | 89.6 |
| Disability card holder, % | 55.3 | 44.7 | 53.3 | 46.7 |
| Non-disability card holder, % | 34.5 | 65.5 | 9.1 | 90.9 |
| Spouse satisfaction, % | ||||
| Very dissatisfied | 70.9 | 29.1 | 23.5 | 76.5 |
| Dissatisfied | 70.3 | 29.7 | 17.6 | 82.4 |
| Fair | 47.2 | 52.8 | 13.3 | 86.7 |
| Satisfied | 31.7 | 68.3 | 7.9 | 92.1 |
| Very satisfied | 22.5 | 77.5 | 6.5 | 93.5 |
| Perceived discrimination, % | 43.2 | 56.8 | 10.9 | 89.1 |
| No perceived discrimination, % | 28.8 | 71.2 | 8.5 | 91.5 |
| Nobody available for help when sick, % | 39.7 | 60.3 | 12.7 | 87.3 |
| Somebody available for help when sick, % | 31.9 | 68.1 | 7.7 | 92.3 |
| Education, % | ||||
| ≤Middle school | 37.5 | 62.5 | 14.3 | 85.7 |
| High school | 34.7 | 65.3 | 9.1 | 90.9 |
| ≥University | 31.5 | 68.5 | 4.9 | 95.1 |
| Employment, % | ||||
| Regular | 29.1 | 70.9 | 5.6 | 94.4 |
| Temporary/day labour | 36.7 | 63.3 | 10.4 | 89.6 |
| Not working | 37.8 | 62.2 | 12.1 | 87.9 |
| Subjective social status, % | ||||
| Low | 44.6 | 55.4 | 17.8 | 82.2 |
| Middle | 30.2 | 69.8 | 5.5 | 94.5 |
| High | 20.9 | 79.1 | 3.1 | 96.9 |
| Income Level & CI | Depression | Poor SRH |
|---|---|---|
| Income level, (unit = 10,000 KRW) | ||
| <100 (n = 865) | 49.0% | 34.7% |
| 100–200 (n = 3105) | 40.1% | 14.2% |
| 200–300 (n = 5073) | 35.8% | 7.5% |
| 300–400 (n = 3420) | 31.7% | 6.2% |
| ≥400 (n = 2858) | 25.7% | 4.0% |
| Uncorrected CI(SE) | −0.0937 (0.0070) | −0.3247 (0.0189) |
| Indirectly std. uncorrected CI(SE) | −0.0923 (0.0068) | −0.2064 (0.0142) |
| Erreygers CI(SE) | −0.1298 (0.0097) | −0.1231 (0.0072) |
| Wagstaff CI(SE) | −0.1433 (0.0108) | −0.3587 (0.0209) |
| Sociodemographic Factors | Exploratory Variables | Depression | Poor SRH | |||
|---|---|---|---|---|---|---|
| CI | Cont. | Cont. | ||||
| Duration of residence | 9.960 | 0.004 | −0.002 * | 0.000 | 0.001 ** | 0.000 |
| Age | ||||||
| 35–49 | 0.392 | 0.074 | −0.048 ** | −0.006 | 0.049 ** | 0.006 |
| 50–64 | 0.147 | −0.105 | −0.097 ** | 0.006 | 0.127 ** | −0.008 |
| ≥65 | 0.027 | −0.723 | −0.052 | 0.004 | 0.318 ** | −0.025 |
| Sex and Country of origin | ||||||
| Women from LMI countries | 0.757 | −0.023 | 0.024 | -0.002 | 0.035 ** | −0.002 |
| Women from HI countries | 0.058 | 0.160 | 0.020 | 0.001 | 0.038 ** | 0.001 |
| Men from LMI countries | 0.142 | −0.044 | −0.046 | 0.001 | 0.025 * | −0.001 |
| Rural residence | 0.243 | −0.074 | −0.020 * | 0.001 | −0.015 ** | 0.001 |
| Disability card holder | 0.007 | −0.468 | 0.202** | −0.003 | 0.147** | −0.002 |
| Satisfaction with a spouse | ||||||
| Dissatisfied | 0.042 | −0.162 | 0.016 | 0.000 | −0.025 | 0.001 |
| Fair | 0.284 | −0.100 | −0.184 ** | 0.021 | −0.058 * | 0.007 |
| Satisfied | 0.288 | −0.007 | −0.329 ** | 0.003 | −0.083 ** | 0.001 |
| Very satisfied | 0.376 | 0.104 | −0.409 ** | −0.064 | −0.085 ** | −0.013 |
| Perceived discrimination | 0.405 | 0.022 | 0.128 ** | 0.004 | 0.028 ** | 0.001 |
| No one for help when sick | 0.353 | −0.067 | 0.046 ** | −0.004 | 0.027 ** | −0.003 |
| Education | ||||||
| High school | 0.436 | −0.016 | 0.004 | 0.000 | −0.019 ** | 0.001 |
| ≥University | 0.272 | 0.175 | 0.018 | 0.003 | −0.036 ** | −0.007 |
| Employment | ||||||
| Temporary/day | 0.304 | 0.026 | 0.041 ** | 0.001 | 0.009 | 0.000 |
| Not working | 0.374 | −0.195 | 0.055 ** | −0.016 | 0.035 ** | −0.010 |
| Income level, (unit = 10,000 KRW) | ||||||
| 100–200 | 0.200 | −0.684 | −0.075 ** | 0.041 | −0.030 * | 0.016 |
| 200–300 | 0.330 | −0.154 | −0.097 ** | 0.020 | −0.055 ** | 0.011 |
| 300–400 | 0.231 | 0.407 | −0.107 ** | −0.040 | −0.053 ** | −0.020 |
| ≥400 | 0.181 | 0.819 | −0.134 ** | −0.080 | −0.065 ** | −0.039 |
| Subjective social status | ||||||
| Middle | 0.626 | 0.104 | −0.095 ** | −0.025 | −0.040 ** | −0.010 |
| High | 0.041 | 0.322 | −0.148 ** | −0.008 | −0.046 ** | −0.002 |
| Residual | - | - | - | 0.0106 | - | −0.0262 |
| Total CI | - | - | - | −0.1298 | - | −0.1231 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.; Lee, J. Decomposing Income-Related Inequalities in Self-Reported Depression and Self-Rated Health Among Married Immigrants in South Korea. Int. J. Environ. Res. Public Health 2019, 16, 1869. https://doi.org/10.3390/ijerph16101869
Hong J, Lee J. Decomposing Income-Related Inequalities in Self-Reported Depression and Self-Rated Health Among Married Immigrants in South Korea. International Journal of Environmental Research and Public Health. 2019; 16(10):1869. https://doi.org/10.3390/ijerph16101869
Chicago/Turabian StyleHong, Jihyung, and Jaehee Lee. 2019. "Decomposing Income-Related Inequalities in Self-Reported Depression and Self-Rated Health Among Married Immigrants in South Korea" International Journal of Environmental Research and Public Health 16, no. 10: 1869. https://doi.org/10.3390/ijerph16101869