Impact of Job Demands and Resources on Nurses’ Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the Nursing Profession


Abstract
:
1. Introduction
2. Theory
2.1. The Job Demands-Resources (JD-R) Model
2.2. Towards a Nursing Sector-Specific Design of the Job Demands-Resources Model
3. Methods
3.1. Sample and Procedure
3.2. Measures
3.3. Statistical Analyses
4. Results
4.1. Preliminary Analyses
4.2. Model Fit and Hypotheses’ Tests
5. Discussion
Limitations of this Study and Recommendations for Future Research
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Sochalski, J.; Silber, J.H. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. J. Am. Med. Assoc. 2002, 288, 1987–1994. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sermeus, W.; Van den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; et al. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ Br. Med. J. 2012, 344, e1717. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.R.; Tourangeau, A.E. Staying in nursing: What factors determine whether nurses intend to remain employed? J. Adv. Nurs. 2012, 68, 1589–1600. [Google Scholar] [CrossRef] [PubMed]
- Hasselhorn, H.; Tackenberg, P.; Mueller, B. (Eds.) Work Conditions and Intent to Leave the Profession Among Nursing Staff in Europe; Report No. 2003: 7; A research project initiated by SALTSA (Joint Program for Working Life Research in Europe) and funded by the by the European Committee (QLK6-CT-2001-00475); National Institute for Working Life: Stockholm, Sweden, 2003. [Google Scholar]
- Heinen, M.M.; van Achterberg, T.; Schwendimann, R.; Zander, B.; Matthews, A.; Kózka, M.; Ensio, A.; Sjetne, I.S.; Casbas, T.M.; Ball, J.; et al. Nurses’ intention to leave their profession: A cross sectional observational study in 10 European countries. Int. J. Nurs. Stud. 2013, 50, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; You, L.M.; Chen, S.X.; Hao, Y.T.; Zhu, X.W.; Zhang, L.F.; Aiken, L.H. The relationship between hospital work environment and nurse outcomes in Guangdong, China: A nurse questionnaire survey. J. Clin. Nurs. 2012, 21, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- North, N.; Erasmussen, E.; Hughes, F.; Finlayson, M.; Ashton, T.; Campbell, T.; Tomkins, S. Turnover amongst nurses in New Zealand’s district health boards: A national survey of nursing turnover and turnover costs. N. Z. J. Employ. Relat. 2005, 30, 49–62. [Google Scholar]
- Jones, C.B. The costs of nurse turnover: Part 1: An economic perspective. J. Nurs. Adm. 2004, 34, 562–570. [Google Scholar] [CrossRef]
- O’Brien-Pallas, L.; Griffin, P.; Shamian, J.; Buchan, J.; Duffield, C.; Hughes, F.; Laschinger, H.K.; North, N.; Stone, P.W. The impact of nurse turnover on patient, nurse, and system outcomes: A pilot study and focus for a multicenter international study. Policy Politics Nurs. Pract. 2006, 7, 169–179. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Job demands–resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef]
- Estryn-Béhar, M.; Van der Heijden, B.I.; Oginska, H.; Camerino, D.; Le Nézet, O.; Conway, P.M.; Fry, C.; Hasselhorn, H.M.; The NEXT Study Group. The impact of social work environment, teamwork characteristics, burnout, and personal factors upon intent to leave among European nurses. Med. Care 2007, 45, 939–950. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.J.M.; Van Dam, K.; Hasselhorn, H.M. Intention to leave nursing: The importance of interpersonal work context, work-home interference, and job satisfaction beyond the effect of occupational commitment. Career Dev. Int. 2009, 14, 616–635. [Google Scholar] [CrossRef]
- Cowden, T.L.; Cummings, G.G. Testing a theoretical model of clinical nurses’ intent to stay. Health Care Manag. Rev. 2015, 40, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Determinants and prevalence of burnout in emergency nurses: A systematic review of 25 years of research. Int. J. Nurs. Stud. 2015, 52, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E.; Euwema, M.C. Job resources buffer the impact of job demands on burnout. J. Occup. Health Psychol. 2005, 10, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E. The Job Demands-Resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; De Jonge, J.; Janssen, P.P.M.; Schaufeli, W.B. Burnout and engagement at work as a function of demands and control. Scand. J. Work Environ. Health 2001, 27, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estryn-Behar, M.; Kaminski, M.; Peigne, E.; Bonnet, N.; Vaichere, E.; Gozlan, C.; Azoulay, S.; Giorgi, M. Stress at work and mental health status among female hospital workers. Br. J. Ind. Med. 1990, 47, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Rudman, A.; Gustavsson, P.; Hultell, D. A prospective study of nurses’ intentions to leave the profession during their first five years of practice in Sweden. Int. J. Nurs. Stud. 2014, 51, 612–624. [Google Scholar] [CrossRef]
- Uğur Gök, A.; Kocaman, G. Reasons for leaving nursing: A study among Turkish nurses. Contemp. Nurse 2011, 39, 65–74. [Google Scholar] [CrossRef]
- Sęk, H. Determinants and mechanisms of professional burnout in the model of social cognitive psychology. In Professional Burnout-Causes, Mechanisms, Prevention; PWN: Warszawa, Poland, 2000; pp. 83–112. (In Polish) [Google Scholar]
- Kahn, R.L.; Byosiere, P. Stress in organizations. In Handbook of Industrial and Organizational Psychology; Dunnette, M.D., Hough, L.M., Eds.; Consulting Psychologists Press: Palo Alto, CA, USA, 1992; Volume 3, pp. 571–650. [Google Scholar]
- Van der Heijde, C.M.; Van der Heijden, B.I.J.M. A competence-based and multidimensional operationalization and measurement of employability. Hum. Resour. Manag. U.S. 2006, 45, 449–476. [Google Scholar] [CrossRef] [Green Version]
- Van der Heijden, B.I.J.M.; De Lange, A.H.; Demerouti, E.; Van der Heijde, C.M. Employability and Career Success Across the Life-Span. Age Effects on the Employability-Career Success Relationship. J. Vocat. Behav. 2009, 74, 156–164. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.J.M.; Notelaers, G.; Peters, P.; Stoffers, J.; De Lange, A.H.; Froehlich, D.; Van der Heijde, C.M. Development and validation of the short-form employability five-factor instrument. J. Vocat. Behav. 2018, 106, 236–248. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Demerouti, E. Job demands–resources theory. In Wellbeing: A Complete Reference Guide, Work and Wellbeing; Chen, P.Y., Cooper, C.L., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2014; Volume 3, pp. 37–64. [Google Scholar]
- Tullar, J.M.; Amick, B.C., III; Brewer, S.; Diamond, P.M.; Kelder, S.H.; Mikhail, O. Improve employee engagement to retain your workforce. Health Care Manag. Rev. 2016, 41, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. The general causality orientations scale: Self-determination in personality. J. Res. Personal. 1985, 19, 109–134. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.J.M.; Peeters, M.C.; Le Blanc, P.M.; Van Breukelen, J.W.M. Job characteristics and experience as predictors of occupational turnover intention and occupational turnover in the European nursing sector. J. Vocat. Behav. 2018, 108, 108–120. [Google Scholar] [CrossRef]
- Bakker, A.B.; Sanz-Vergel, A.I. Weekly work engagement and flourishing: The role of hindrance and challenge job demands. J. Vocat. Behav. 2013, 83, 397–409. [Google Scholar] [CrossRef]
- Bakker, A.B.; Van Veldhoven, M.; Xanthopoulou, D. Beyond the demand-control model: Thriving on high job demands and resources. J. Pers. Psychol. 2010, 9, 3–16. [Google Scholar] [CrossRef]
- Riedl, E.M.; Thomas, J. The moderating role of work pressure on the relationships between emotional demands and tension, exhaustion, and work engagement: An experience sampling study among nurses. Eur. J. Work Organ. Psychol. 2019, 28, 414–429. [Google Scholar] [CrossRef]
- Scanlan, J.N.; Still, M. Relationships between burnout, turnover intention, job satisfaction, job demands and job resources for mental health personnel in an Australian mental health service. BMC Health Serv. Res. 2019, 19, 62. [Google Scholar] [CrossRef]
- Van Woerkom, M.; Bakker, A.B.; Nishii, L.H. Accumulative job demands and support for strength use: Fine-tuning the job demands-resources model using conservation of resources theory. J. Appl. Psychol. 2016, 101, 141–150. [Google Scholar] [CrossRef]
- Mullarkey, S.; Wall, T.D.; Warr, P.B.; Clegg, C.W.; Stride, C. Measures of Job Satisfaction, Mental Health and Job-Related Well-Being: A Bench-Marking Manual; Institute of Work Psychology: Sheffield, UK, 1999. [Google Scholar]
- Van der Heijden, B.I.J.M.; Bakker, A.B. Toward a mediation model of employability enhancement: A study of employee-supervisor pairs in the building sector. Career Dev. Q. 2011, 59, 232–248. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.J.M. Organisational influences upon the development of occupational expertise throughout the career. Int. J. Train. Dev. 2003, 7, 142–165. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.J.M.; Gorgievski, M.J.; De Lange, A.H. Learning at the workplace and sustainable employability: A multi-source model moderated by age. Eur. J. Work Organ. Psychol. 2016, 25, 13–30. [Google Scholar] [CrossRef]
- Rothman, R.A.; Perrucci, R. Organizational careers and professional expertise. Adm. Sci. Q. 1970, 15, 282–293. [Google Scholar] [CrossRef]
- De Jonge, J.; Mulder, M.J.G.P.; Nijhuis, F.J.N. The incorporation of different demand concepts in the Job Demand-Control model: Effects on health care professionals. Soc. Sci. Med. 1999, 48, 1149–1160. [Google Scholar] [CrossRef]
- Houkes, I.; Janssen, P.M.; De Jonge, J.; Nijhuis, F.J.N. Specific relationships between work characteristics and intrinsic work motivation, burnout and turnover intention: A multi-sample analysis. Eur. J. Work Organ. Psychol. 2001, 10, 1–23. [Google Scholar] [CrossRef]
- Van der Doef, M.; Maes, S. The job demand-control (-support) model and psychological well-being: A review of 20 years of empirical research. Work Stress 1999, 13, 87–114. [Google Scholar] [CrossRef]
- Rhoades, L.; Eisenberger, R. Perceived organizational support: A review of the literature. J. Appl. Psychol. 2002, 87, 698–714. [Google Scholar] [CrossRef]
- Peterson, S.L. Toward a theoretical model of employee turnover: A human resource development perspective. Hum. Resour. Dev. Rev. 2004, 3, 151–176. [Google Scholar] [CrossRef]
- Estryn-Behar, M. Work Schedules and Night Work in Health Care. In Encyclopedia of Occupational Health and Safety, 4th ed.; International Labor Office: Geneva, Switzerland, 1997; pp. 22–26. [Google Scholar]
- Stordeur, S.; D’hoore, W.; Vandenberghe, C. Leadership, organizational stress, and emotional exhaustion among nursing hospital staff. J. Adv. Nurs. 2001, 35, 533–542. [Google Scholar] [CrossRef]
- Lucas, M.; Atwood, J.; Hagaman, R. Replication and validation of anticipated turnover model for urban registered nurses. Nurs. Res. 1993, 42, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Tett, R.P.; Meyer, J.P. Job satisfaction, organizational commitment, turnover intention, and turnover: Path analyses on meta-analytic findings. Pers. Psychol. 1993, 46, 259–293. [Google Scholar] [CrossRef]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef] [PubMed]
- Debray, Q.; Estryn-Behar, M.; Guillibert, E.; Azoulay, S.; Bonnet, N. Travail féminin en milieu hospitalier: Un facteur de dépression: Une étude pilote [Female work in a hospital environment: A factor of depression: A pilot study]. Psychiatre Psychobiol. 1988, 3, 389–399. [Google Scholar]
- Hockey, G.R. Cognitive-energetical control mechanisms in the management of work demands and psychological health. In Attention: Selection, Awareness, and Control; Baddeley, A., Weiskrantz, L., Eds.; Clarendon Press: Oxford, UK, 1993; pp. 328–345. [Google Scholar]
- Hobfoll, S.E. Social and psychological resources and adaptation. Rev. Gen. Psychol. 2002, 6, 307–324. [Google Scholar] [CrossRef]
- Halbesleben, J.R.; Neveu, J.P.; Paustian-Underdahl, S.C.; Westman, M. Getting to the “COR” understanding the role of resources in conservation of resources theory. J. Manag. 2014, 40, 1334–1364. [Google Scholar]
- Zhang, L.; Fan, C.; Deng, Y.; Lam, C.F.; Hu, E.; Wang, L. Exploring the interpersonal determinants of job embeddedness and voluntary turnover: A conservation of resources perspective. Hum. Resour. Manag. 2019, 1–20. [Google Scholar] [CrossRef]
- Kooij, D.; De Lange, A.; Jansen, P.; Dikkers, J. Older workers’ motivation to continue to work: Five meanings of age. J. Manag. Psychol. 2008, 23, 364–394. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.J.M. Interpersonal work context as a possible buffer against age-related stereotyping. Ageing Soc. 2018, 38, 129–165. [Google Scholar] [CrossRef]
- Wright, J.D.; Hamilton, R.F. Work satisfaction and age: Some evidence for the ‘job change’ hypothesis. Soc. Forces 1978, 56, 1140–1157. [Google Scholar]
- Watkins, C.E.; Subich, L.M. Annual review, 1992–1994: Career development, reciprocal work/non-work interaction, and women’s workforce anticipation. J. Vocat. Behav. 1995, 47, 109–163. [Google Scholar] [CrossRef]
- Edwards, J.R.; Cable, D.M.; Williamson, I.O.; Lambert, L.S.; Shipp, A.J. The phenomenology of fit: Linking the person and environment to the subjective experience of person–environment fit. J. Appl. Psychol. 2006, 91, 802–827. [Google Scholar] [CrossRef] [PubMed]
- Castle, N.G.; Degenholtz, H.; Rosen, J. Determinants of staff job satisfaction of caregivers in two nursing homes in Pennsylvania. BMC Health Serv. Res. 2006, 6, 60. [Google Scholar] [CrossRef] [PubMed]
- Chiok Foong Loke, J. Leadership behaviours: Effects on job satisfaction, productivity, and organizational commitment. J. Nurs. Manag. 2001, 9, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Kovner, C.T.; Brewer, C.S.; Cheng, Y.; Djukic, M. Work attitudes of older RNs. Policy Politics Nurs. Pract. 2007, 8, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Nei, D.; Snyder, L.A.; Litwiller, B.J. Promoting retention of nurses: A meta-analytic examination of causes of nurse turnover. Health Care Manag. Rev. 2015, 40, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Norman, L.D.; Donelan, K.; Buerhaus, P.I.; Willis, G.; Williams, M.; Ulrich, B.; Dittus, R. The older nurse in the workplace: Does age matter? Nurs. Econ. 2005, 23, 282–289. [Google Scholar]
- Piko, B.F. Burnout, role conflict, job satisfaction, and psychosocial health among Hungarian health care staff: A questionnaire survey. Int. J. Nurs. Stud. 2006, 43, 311–318. [Google Scholar] [CrossRef]
- Price, J.L.; Mueller, C.W. A causal model of turnover for nurses. Acad. Manag. J. 1981, 24, 543–565. [Google Scholar]
- Price, J.L. The Study of Turnover; Iowa State University Press: Ames, IA, USA, 1977. [Google Scholar]
- Chan, M.F.; Luk, A.L.; Leong, S.M.; Yeung, S.M.; Van, I.K. Factors influencing Macao nurses’ intention to leave current employment. J. Clin. Nurs. 2009, 18, 893–901. [Google Scholar] [CrossRef]
- Delobelle, P.; Rawlinson, J.L.; Ntuli, S.; Malatsi, I.; Decock, R.; Depoorter, A.M. Job satisfaction and turnover intent of primary healthcare nurses in rural South Africa: A questionnaire survey. J. Adv. Nurs. 2011, 67, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Mazurenko, O.; Gupte, G.; Shan, G. Analyzing US nurse turnover: Are nurses leaving their jobs or the profession itself? J. Hosp. Adm. 2015, 4, 48–56. [Google Scholar]
- Ng, T.W.; Feldman, D.C. Organizational tenure and job performance. J. Manag. 2010, 36, 1220–1250. [Google Scholar] [CrossRef]
- Finkelstein, L.M.; Farrell, S.K. An expanded view of age bias in the workplace. In Aging and Work in the 21st Century; Shultz, K.S., Adams, G.A., Eds.; Lawrence Erlbaum Associates: London, UK, 2007. [Google Scholar]
- Van den Broeck, A.; De Cuyper, N.; De Witte, H.; Vansteenkiste, M. Not all job demands are equal: Differentiating job hindrances and job challenges in the Job Demands–Resources model. Eur. J. Work Organ. Psychol. 2010, 19, 735–759. [Google Scholar] [CrossRef]
- Messchendorp, H.J.; Van der Weerd, E.; Steenbeek, R.; Dinkgreve, R.; Meulenkamp, T.; Mettendaf, A. Work in the Picture; Industry Report 2002 Employee Consultation CAO Occupational Health Nursing and Care Homes; Prismant: Utrecht, The Netherlands, 2002. [Google Scholar]
- Kristensen, T.S. A New Tool for Assessing Psychosocial Factors at Work: The Copenhagen Psychosocial Questionnaire; National Institute of Occupational Health: Copenhagen, Denmark, 2000. [Google Scholar]
- Netemeyer, R.G.; Boles, J.S.; McMurrian, R. Development and validation of work–family conflict and family–work conflict scales. J. Appl. Psychol. 1996, 81, 400–410. [Google Scholar] [CrossRef]
- Van der Heijden, B.I.J.M. The Measurement and Development of Professional Expertise throughout the Career. A Retrospective Study among Higher Level Dutch Professionals. Ph.D. Thesis, University of Twente, Enschede, The Netherlands, 1998. [Google Scholar]
- Siegrist, J.; Starke, D.; Chandola, T.; Godin, I.; Marmot, M.; Niedhammer, I.; Peter, R. The measurement of effort–reward imbalance at work: European comparisons. Soc. Sci. Med. 2004, 58, 1483–1499. [Google Scholar] [CrossRef]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen Burnout Inventory; A new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Marsh, H.W.; Balla, J.R.; Hau, K.T. An evaluation of incremental fit indices: A clarification of mathematical and empirical properties. In Advanced Structural Equation Modeling: Issues and Techniques; Marcoulides, G.A., Schumacker, R.E., Eds.; Erlbaum: Mahwah, NJ, USA, 1996; pp. 315–353. [Google Scholar]
- Van de Schoot, R.; Lugtig, P.; Hox, J. A checklist for testing measurement invariance. Eur. J. Dev. Psychol. 2012, 9, 486–492. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef]
- Sobel, M.E. Asymptotic Confidence Intervals for Indirect Effects in Structural Equation Models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Grewal, R.; Cote, J.A.; Baumgartner, H. Multicollinearity and measurement error in structural equation models: Implications for theory testing. Mark. Sci. 2004, 23, 519–524. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale Development: Theory and Applications; Sage: Los Angeles, CA, USA, 2012. [Google Scholar]
- Blau, G. Does a corresponding set of variables for explaining voluntary organizational turnover transfer to explaining voluntary occupational turnover? J. Vocat. Behav. 2007, 70, 135–148. [Google Scholar] [CrossRef]
- Estryn-Behar, M.; Van der Heijden, B.I.J.M.; Fry, C.; Hasselhorn, H.M. Longitudinal analysis of personal and work-related factors associated with turnover among nurses. Nurs. Res. 2010, 59, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Van der Heijden, B.I.J.M.; Kümmerling, A.; Van Dam, K.; Van der Schoot, E.; Estryn-Béhar, M.; Hasselhorn, H.M. The impact of social support upon intention to leave among female nurses in Europe: Secondary analysis of data from the NEXT survey. Int. J. Nurs. Stud. 2010, 47, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Adams, G.A.; Beehr, T.A. Turnover and retirement: A comparison of their similarities and differences. Pers. Psychol. 1998, 51, 643–665. [Google Scholar] [CrossRef]
- Griffeth, R.W.; Hom, P.W.; Gaertner, S. A meta-analysis of antecedents and correlates of employee turnover: Update, moderator test, and research implications for the next millennium. J. Manag. 2000, 26, 463–488. [Google Scholar] [CrossRef]
- Lee, K.; Carswell, J.J.; Allen, N. A meta-analytic review of occupational commitment: Relations with person- and work-related variables. J. Appl. Psychol. 2000, 85, 799–811. [Google Scholar] [CrossRef]
- Blau, G.J.; Lunz, M.E. Testing the incremental effect of professional commitment on intent to leave one’s profession beyond the effects of external, personal, and work-related variables. J. Vocat. Behav. 1998, 52, 260–269. [Google Scholar] [CrossRef]
- Kirpal, S. Work identities of nurses. Between caring and efficiency demands. Career Dev. Int. 2004, 9, 274–304. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | female | 94.44 | 0.23 | - | ||||||||||||||
| 2 | Tenure in the profession | 13.62 | 8.57 | 0.01 | ||||||||||||||
| 3 | age | 39.80 | 9.68 | 0.02 | 0.74 ** | |||||||||||||
| 4 | Emotional demands | 3.45 | 0.58 | −0.15 ** | 0.02 | −0.01 ** | 0.70 | |||||||||||
| 5 | Quantitative demands | 2.99 | 0.55 | 0.55 | 0.03 | −0.06 * | 0.28 ** | 0.70 | ||||||||||
| 6 | Physical demands | 3.19 | 2.55 | 0.02 | −0.16 ** | −0.30 ** | 0.27 ** | 0.31 ** | 0.87 | |||||||||
| 7 | Family-work conflict | 1.51 | 0.60 | −0.04 | −0.05 | −0.11 ** | 0.03 | 0.14 ** | 0.06 | 0.85 | ||||||||
| 8 | Quality of leadership | 3.09 | 0.76 | 0.05 | −0.05 | −0.03 | −0.01 | −0.15 ** | −0.05 | −0.08 ** | 0.87 | |||||||
| 9 | Developmental opportunities | 3.72 | 0.66 | −0.04 | −0.07 * | −0.19 ** | 0.21 ** | 0.12 ** | 0.08 ** | −0.01 | 0.22 ** | 0.75 | ||||||
| 10 | Social support; supervisor | 3.04 | 0.86 | 0.00 | −0.06 * | −0.04 | 0.00 | −0.12 ** | −0.00 | −0.05 | 0.63 ** | 0.20 ** | 0.84 | |||||
| 11 | Social support; colleagues | 3.71 | 0.63 | −0.01 | −0.13 ** | −0.27 ** | 0.14 ** | 0.06 * | 0.16 ** | −0.02 | 0.13 ** | 0.29 ** | 0.20 ** | 0.77 | ||||
| 12 | Perceived effort | 1.89 | 0.49 | −0.07 * | -0.01 | −0.11 ** | 0.23 ** | 0.53 ** | 0.26 ** | 0.16 ** | −0.12 ** | 0.12 ** | 0.11 ** | 0.03 | 0.85 | |||
| 13 | Meaning of work | 4.22 | 0.57 | 0.06 | −0.11 ** | −0.10 ** | 0.06 * | 0.04 | 0.05 | −0.05 | 0.24 ** | 0.45 ** | 0.24 ** | 0.21 ** | 0.00 | 0.81 | ||
| 14 | Burnout | 1.64 | 0.55 | 0.00 | −0.08 ** | −0.15 ** | 0.11 ** | 0.23 ** | 0.09 ** | 0.21 ** | 0.11 ** | 0.02 | −0.07 * | 0.00 | 0.34 ** | −0.63 ** | 0.83 | |
| 15 | Occupational turnover | 1.43 | 0.70 | −0.08 * | −0.01 | −0.06 ** | 0.02 | 0.06 * | −0.00 | 0.10 ** | 0.14 ** | −0.09 ** | −0.10 ** | 0.02 | 0.06 ** | −0.19 ** | −0.16 ** | 0.85 |
| Determinants of Occupational Turnover Intention | Age < 40 | Age > 40 |
|---|---|---|
| Emotional demands *** | 3.50 | 3.40 |
| Quantitative demands | 3.00 | 2.97 |
| Physical demands *** | 30.22 | 20.94 |
| Family-work conflict ** | 1.56 | 1.46 |
| Quality of leadership | 3.10 | 3.07 |
| Developmental opportunities *** | 3.82 | 3.63 |
| Social support, from supervisor | 3.08 | 3.00 |
| Social support, from colleagues ** | 3.84 | 3.60 |
| Perceived effort ** | 11.53 | 11.02 |
| Meaning of work | 4.25 | 4.19 |
| Burnout *** | 1.57 | 1.71 |
| Gender | 94.00% | 94.87% |
| Professional tenure *** | 7.94 | 19.10 |
| Occupational turnover intention | 1.46 | 1.40 |
| How often have you thought about giving up nursing completely? | Less than 40; Age in years | 40 and over; Age in years |
|---|---|---|
| Never | 63.45% | 69.38% |
| Several times per year | 29.14% | 23.88% |
| Several times per month | 5.69% | 4.15% |
| Several times per week | 1.38% | 2.08% |
| Every day | 0.34% | 0.52% |
| Model | χ2 | df | CFI | RMSEA | IFI | TLI | χ2 | df |
|---|---|---|---|---|---|---|---|---|
| Unconstrained | 232.09 | 108 | 0.95 | 0.030 | 0.95 | 0.92 | ||
| Structural weights | 245.91 | 123 | 0.95 | 0.031 | 0.95 | 0.91 | 13.82 *** | 15 |
| Structural intercepts | 272.87 | 127 | 0.94 | 0.031 | 0.94 | 0.91 | 40.78 *** | 19 |
| Structural means | 965.61 | 137 | 0.64 | 0.071 | 0.64 | 0.52 | 733.52 *** | 29 |
| Structural covariances | 1199.94 | 169 | 0.55 | 0.072 | 0.55 | 0.51 | 967.85 *** | 61 |
| Structural residuals | 1205.27 | 173 | 0.55 | 0.071 | 0.55 | 0.52 | 973.17 *** | 65 |
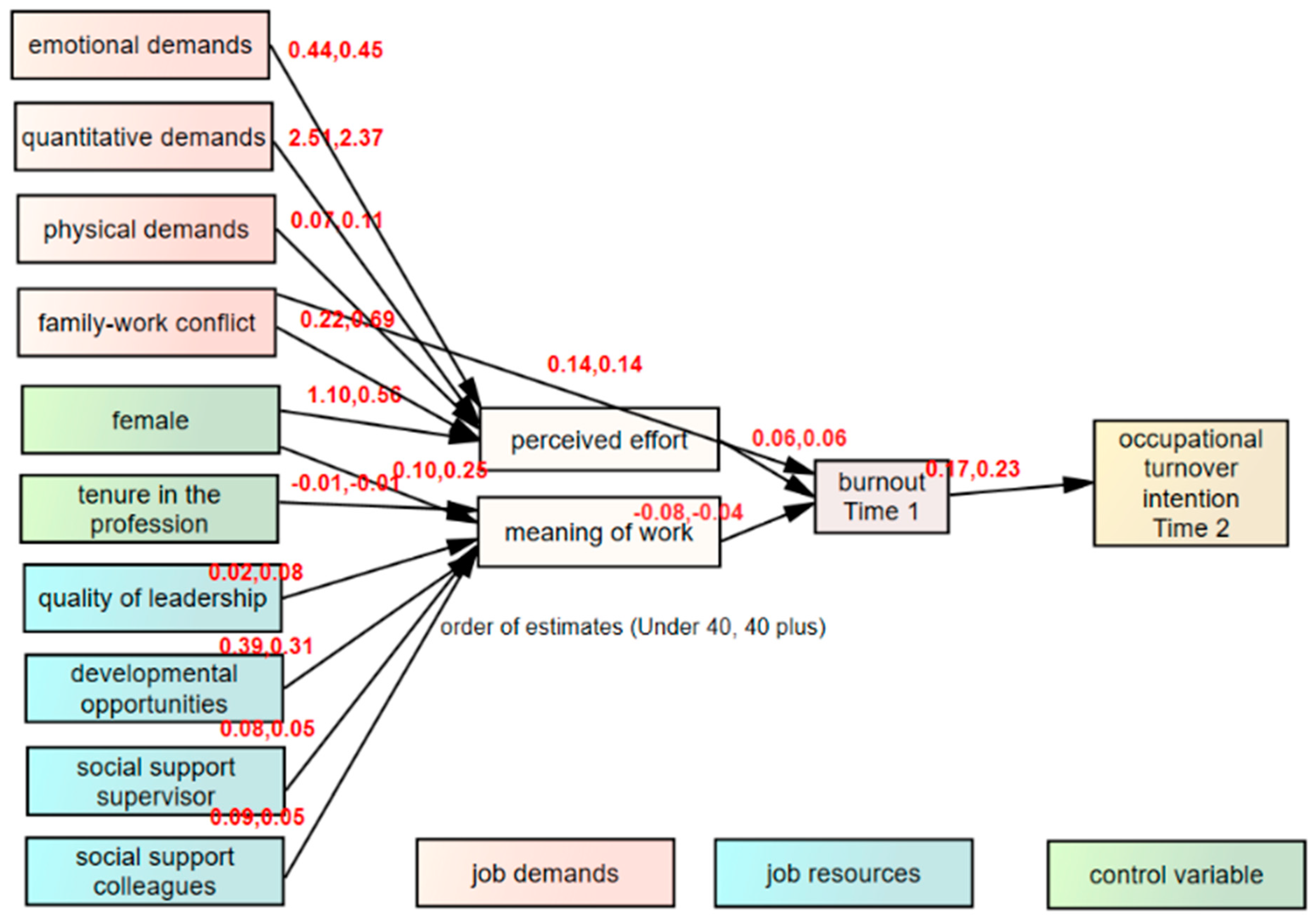
| Determinants of Occupational Turnover Intention | Perceived Effort | Meaning of Work | Burnout | Occupational Turnover Intention | ||||
|---|---|---|---|---|---|---|---|---|
| Under 40 | 40 plus | Under 40 | 40 plus | Under 40 | 40 plus | Under 40 | 40 plus | |
| Emotional demands | 0.44 (0.08) * | 0.45 (0.09) * | ||||||
| Quantitative demands | 2.51 (0.49) *** | 2.37 (0.44) *** | ||||||
| Physical demands | 0.07 (0.06) | 0.11 (0.09) * | ||||||
| Family-work conflict | 0.22 (0.05) | 0.69 (0.14) *** | 0.14 (0.15) *** | 0.14 (0.15) *** | ||||
| Quality of leadership | 0.02 (0.03) | 0.08 (0.10) * | ||||||
| Developmental opportunities | 0.39 (0.43) *** | 0.31 (0.37) *** | ||||||
| Social support from supervisor | 0.08 (0.08) * | 0.05 (0.06) | ||||||
| Social support from colleagues | 0.09 (0.13) *** | 0.05 (0.08) | ||||||
| Perceived effort | 0.06 (0.30) *** | 0.06 (0.31) *** | ||||||
| Meaning of work | −0.08 (−0.08) * | −0.04 (−0.04) * | ||||||
| Burnout | 0.17 (0.14) *** | 0.23 (0.17) *** | ||||||
| Gender | 1.10 (0.09) ** | 0.56 (0.04) | 0.10 (0.04) | 0.25 (0.10) ** | ||||
| Professional tenure | −0.01 (−0.11) *** | −0.01 (−0.11) *** | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van der Heijden, B.; Brown Mahoney, C.; Xu, Y. Impact of Job Demands and Resources on Nurses’ Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the Nursing Profession. Int. J. Environ. Res. Public Health 2019, 16, 2011. https://doi.org/10.3390/ijerph16112011
Van der Heijden B, Brown Mahoney C, Xu Y. Impact of Job Demands and Resources on Nurses’ Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the Nursing Profession. International Journal of Environmental Research and Public Health. 2019; 16(11):2011. https://doi.org/10.3390/ijerph16112011
Chicago/Turabian StyleVan der Heijden, Beatrice, Christine Brown Mahoney, and Yingzi Xu. 2019. "Impact of Job Demands and Resources on Nurses’ Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the Nursing Profession" International Journal of Environmental Research and Public Health 16, no. 11: 2011. https://doi.org/10.3390/ijerph16112011
APA StyleVan der Heijden, B., Brown Mahoney, C., & Xu, Y. (2019). Impact of Job Demands and Resources on Nurses’ Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the Nursing Profession. International Journal of Environmental Research and Public Health, 16(11), 2011. https://doi.org/10.3390/ijerph16112011