Family Affluence Based Inequality in Oral Health-Related Quality of Life in a Population of Lithuanian Adolescents


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Sample Size Calculation
2.3. Study Design, Participants, and Data Collection
2.4. Evaluation of Oral Health-Related Quality of Life
2.5. Evaluation of Orthodontic Status
2.6. Evaluation of Family Affluence
2.7. Statistical Analysis
3. Results
3.1. Descriptive Statistics and Correlations
3.2. Direct Influence of Malocclusion and Family Affluence on OHRQoL
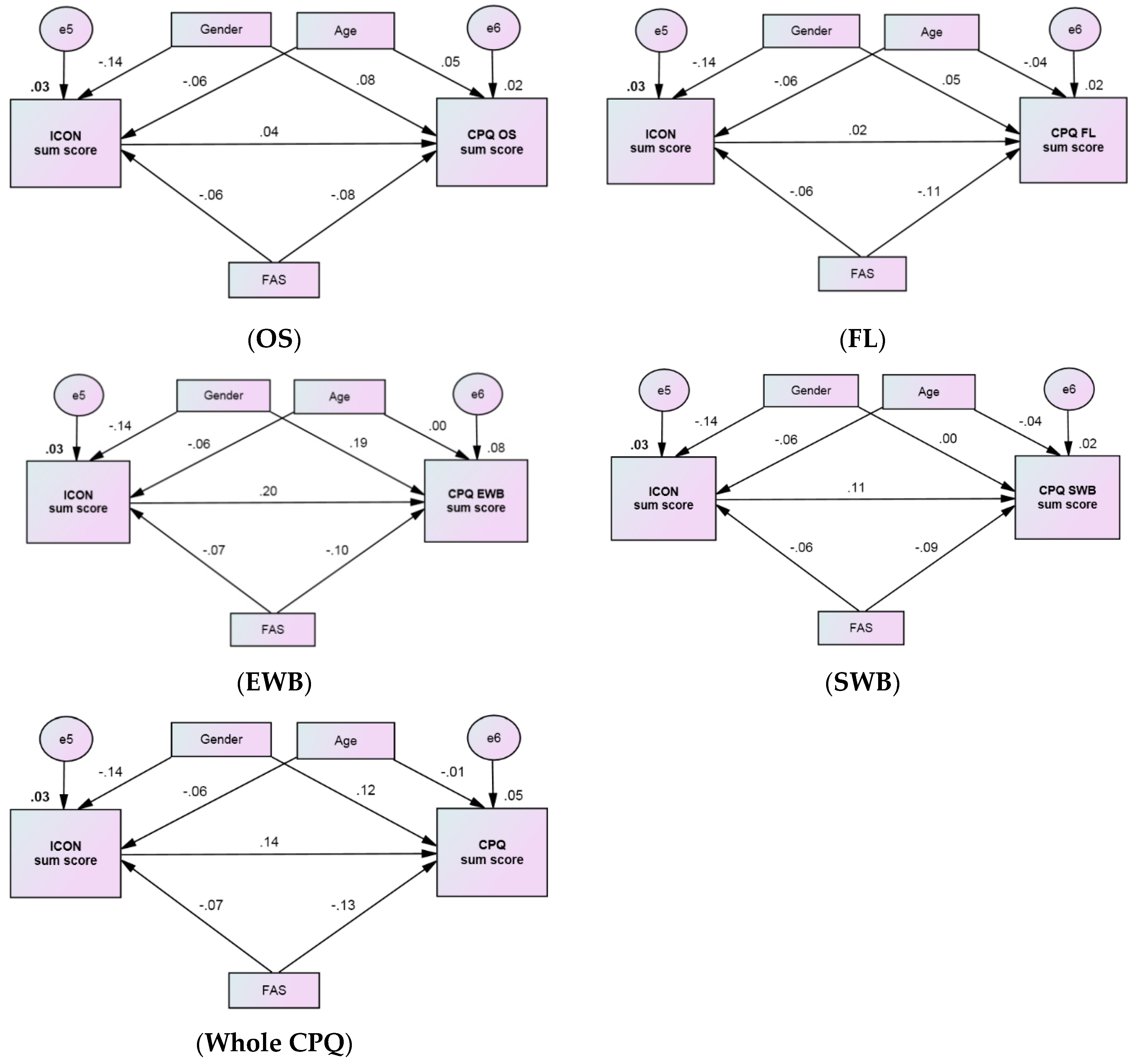
3.3. Path Analysis of the Associations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
Abbreviations
| AC | Aesthetic Component |
| CI | Confidence Interval |
| CPQ | Child Perceptions Questionnaire |
| EWB | Emotional Well-Being |
| FAS | Family Affluence Scale |
| FL | Functional Limitations |
| ICON | Index of Complexity Outcome and Need |
| NBR | Negative Binomial Regression |
| OHRQoL | Oral Health-Related Quality of Life |
| OS | Oral Symptoms |
| RSSM | Ratio of Sum Score Means |
| QoL | Quality of Life |
| SD | Standard Deviation |
| SES | Socio-Economic Status |
| SWB | Social Well-Being |
References
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Org. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Baubinienė, D. Ortodontinių Anomalijų Paplitimas IR Gydymo Reikalingumas Tarp Lietuvos Moksleivių (Prevalence of Malocclusion and Treatment Need in Lithuanian Schoolchildren). Ph.D. Dissertation, Kaunas University of Medicine, Kaunas, Lithuania, 2010. (In Lithuanian). [Google Scholar]
- Dimberg, L.; Arnrup, K.; Bondemark, L. The impact of malocclusion on the quality of life among children and adolescents: A systematic review of quantitative studies. Eur. J. Orthod. 2015, 37, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Kragt, L.; Dhamo, B.; Wolvius, E.B.; Ongkosuwito, E.M. The impact of malocclusions on oral health-related quality of life in children—A systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 1881–1894. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; McGrath, C.; Hagg, U. The Impact of Malocclusion/Orthodontic Treatment Need on the Quality of Life. Angle Orthod. 2009, 79, 585–591. [Google Scholar]
- Masood, Y.; Masood, M.; Zainul, N.N.B.; Araby, N.B.A.A.; Hussain, S.F.; Newton, T.; Newton, J.T. Impact of malocclusion on oral health related quality of life in young people. Health Qual. Life Outcomes 2013, 11, 25. [Google Scholar] [CrossRef]
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Association between Global Life Satisfaction and Self-Rated Oral Health Conditions among Adolescents in Lithuania. Int. J. Environ. Res. Public Health 2017, 14, 1338. [Google Scholar] [CrossRef]
- Chen, M.; Feng, Z.-C.; Liu, X.; Li, Z.-M.; Cai, B.; Wang, D.-W. Impact of malocclusion on oral health–related quality of life in young adults. Angle Orthod. 2015, 85, 986–991. [Google Scholar] [CrossRef]
- Mat, A. The Determinants of Children’s Oral Health Related Quality of Life. Ph.D. Thesis, University of Sheffield, Sheffield, UK, 2010. [Google Scholar]
- ICOHIRP. Social Inequalities in Oral Health: From Evidence to Action. Secondary Social Inequalities in Oral Health: From Evidence to Action. 2015. Available online: http://www.icohirp.com/monograph.html (accessed on 20 June 2019).
- Sgan-Cohen, H.D.; Evans, R.W.; Whelton, H.; Villena, R.S.; MacDougall, M.; Williams, D.M. Global Oral Health Inequalities Research Agenda (IADR-GOHIRA(R)): A call to action. J. Dent. Res. 2013, 92, 209–211. [Google Scholar] [CrossRef]
- Da Cunha, I.P.; Pereira, A.C.; Frias, A.C.; Vieira, V.; de Castro Meneghim, M.; Batista, M.J.; Cortellazzi, K.L.; Bulgareli, J.V. Social vulnerability and factors associated with oral impact on daily performance among adolescents. Health Qual. Life Outcomes 2017, 15, 173. [Google Scholar] [CrossRef]
- Araki, M.; Yasuda, Y.; Ogawa, T.; Tumurkhuu, T.; Ganburged, G.; Bazar, A.; Fujiwara, T.; Moriyama, K. Associations between Malocclusion and Oral Health-Related Quality of Life among Mongolian Adolescents. Int. J. Environ. Res. Public Health 2017, 14, 902. [Google Scholar] [CrossRef] [PubMed]
- Vedovello, S.A.; Ambrosano, G.M.; Pereira, A.C.; Valdrighi, H.C.; Filho, M.V.; de Castro Meneghim, M. Association between malocclusion and the contextual factors of quality of life and socioeconomic status. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Locker, D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent. Oral Epidemiol. 2007, 35, 348–356. [Google Scholar] [CrossRef] [PubMed]
- De Paula, J.S.; Leite, I.C.G.; De Almeida, A.B.; Ambrosano, G.M.B.; Mialhe, F.L. The impact of socioenvironmental characteristics on domains of oral health-related quality of life in Brazilian schoolchildren. BMC Oral Health 2013, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Inglehart, M.R.; Bagramian, R.A. Oral health related quality of life: An introduction. In Oral Health Related Quality of Life; Inglehart, M.R., Bagramian, R.A., Eds.; Quintessence Publishing: Chicago, IL, USA, 2011; pp. 1–6. [Google Scholar]
- Jokovic, A.; Locker, D.; Stephens, M.; Kenny, D.; Tompson, B.; Guyatt, G. Validity and Reliability of a Questionnaire for Measuring Child Oral-health-related Quality of Life. J. Dent. Res. 2002, 81, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Borzabadi-Farahani, A. An insight into four orthodontic treatment need indices. Prog. Orthod. 2011, 12, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Bellot-Arcís, C.; Montiel-Company, J.M.; Almerich-Silla, J.M.; Bourzgui, F. (Eds.) Orthodontics—Basic aspects and clinical considerations. In Orthodontic Treatment Need: An Epidemiological Approach; InTech: Rijeka, Croatia, 2012; pp. 3–28. [Google Scholar]
- Borzabadi-Farahani, A.; Borzabadi-Farahani, A. Agreement between the index of complexity, outcome, and need and the dental and aesthetic components of the index of orthodontic treatment need. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 233–238. [Google Scholar] [CrossRef]
- G*Power 3.1 Manual. 1 March 2017. Available online: http://www.gpower.hhu.de/fileadmin/redaktion/Fakultaeten/Mathematisch-Naturwissenschaftliche_Fakultaet/Psychologie/AAP/gpower/GPowerManual.pdf (accessed on 12 June 2019).
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Modification and psychometric evaluation of the child perceptions questionnaire (CPQ11–14) in assessing oral health related quality of life among Lithuanian children. BMC Oral Health 2019, 19, 1. [Google Scholar] [CrossRef]
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Validity of Lithuanian Version of the Child Perceptions Questionnaire Among Adolescents up to the Ages of 18. J. Clin. Res. Med. 2018, 1, 1–9. [Google Scholar]
- WHO. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Richmond, S. Evaluating Effective Orthodontic Care; FIRST Numerics Ltd.: Cardiff, UK, 2008. [Google Scholar]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef]
- Moksony, F.; Hegedus, R. The use of Poisson regression in the sociological study of suicide. Corvinus J. Sociol. Soc. Policy 2014, 5, 97–114. [Google Scholar] [CrossRef]
- Hayat, M.J.; Higgins, M. Understanding poisson regression. J. Nurs. Educ. 2014, 53, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Čekanavičius, V.; Murauskas, G. Taikomoji Regresinė Analizė Socialiniuose Tyrimuose (Applied Regression Analysis in Social Siences); Vilnius University: Vilnius, Lithuania, 2014. (In Lithuanian) [Google Scholar]
- Čekanavičius, V.; Murauskas, G. Statistika IR Jos Taikymai (Statistics and Its Applications), 3 Knyga; REV UAB BĮ: Vilnius, Lithuania, 2009. (In Lithuanian) [Google Scholar]
- Arbuckle, J.L. IBM SPSS AMOS 21 User’s Guide; Amos Development Corporation: Crawfordville, FL, USA, 2012. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA; London, UK, 2015. [Google Scholar]
- Sun, L.; Wong, H.M.; McGrath, C.P.J. The factors that influence oral health-related quality of life in 15-year-old children. Health Qual. Life Outcomes 2018, 16, 19. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, T.S.; Tureli, M.C.M.; Gavião, M.B.D. Validity and reliability of the Child Perceptions Questionnaires applied in Brazilian children. BMC Oral Health 2009, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Relationship Between Orthodontic Treatment Need and Oral Health-Related Quality of Life among 11–18-Year-Old Adolescents in Lithuania. Int. J. Environ. Res. Public Health 2018, 15, 1012. [Google Scholar] [CrossRef] [PubMed]
- Simões, R.C.; Goettems, M.L.; Schuch, H.S.; Torriani, D.D.; Demarco, F.F. Impact of Malocclusion on Oral Health-Related Quality of Life of 8–12 Years Old Schoolchildren in Southern Brazil. Braz. Dent. J. 2017, 28, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Foster Page, L.A.; Thomson, W.M.; Jokovic, A.; Locker, D. Validation of the Child Perceptions Questionnaire (CPQ11–14). J. Dent. Res. 2005, 84, 649–652. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.L.; Conboy, F.; Macfarlane, T.; Mandall, N. The child perception questionnaire is valid for malocclusions in the United Kingdom. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 536–540. [Google Scholar] [CrossRef]
- Spalj, S.; Slaj, M.; Varga, S.; Strujic, M.; Slaj, M. Perception of orthodontic treatment need in children and adolescents. Eur. J. Orthod. 2010, 32, 387–394. [Google Scholar] [CrossRef]
- Seehra, J.; Newton, J.T.; Dibiase, A.T. Interceptive orthodontic treatment in bullied adolescents and its impact on self-esteem and oral-health-related quality of life. Eur. J. Orthod. 2013, 35, 615–621. [Google Scholar] [CrossRef]
- Seehra, J.; Fleming, P.S.; Newton, T.; DiBiase, A.T. Bullying in orthodontic patients and its relationship to malocclusion, self-esteem and oral health-related quality of life. J. Orthod. 2011, 38, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Colussi, P.R.G.; Hugo, F.N.; Muniz, F.W.M.G.; Rösing, C.K. Oral Health-Related Quality of Life and Associated Factors in Brazilian Adolescents. Braz. Dent. J. 2017, 28, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machry, R.V.; Knorst, J.K.; Tomazoni, F.; Ardenghi, T.M. School environment and individual factors influence oral health related quality of life in Brazilian children. Braz. Oral Res. 2018, 32, 63. [Google Scholar] [CrossRef] [PubMed]
- Paula, J.S.; Da Cruz, J.N.; Ramires, T.G.; Ortega, E.M.M.; Mialhe, F.L. Longitudinal impact of clinical and socioenvironmental variables on oral health-related quality of life in adolescents. Braz. Oral Res. 2017, 31, 70. [Google Scholar] [CrossRef] [PubMed]
- Paula, J.S.; Leite, I.C.; Almeida, A.B.; Ambrosano, G.M.; Pereira, A.C.; Mialhe, F.L. The influence of oral health conditions, socioeconomic status and home environment factors on schoolchildren’s self-perception of quality of life. Health Qual. Life Outcomes 2012, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- Piovesan, C.; Antunes, J.L.F.; Guedes, R.S.; Ardenghi, T.M. Impact of socioeconomic and clinical factors on child oral health-related quality of life (COHRQoL). Qual. Life Res. 2010, 19, 1359–1366. [Google Scholar] [CrossRef]
- Polk, D.E.; Weyant, R.J.; Manz, M.C. Socioeconomic factors in adolescents’ oral health: Are they mediated by oral hygiene behaviors or preventive interventions? Community Dent. Oral Epidemiol. 2010, 38, 1–9. [Google Scholar] [CrossRef]
- Sardenberg, F.; Martins, M.T.; Bendo, C.B.; Pordeus, I.A.; Paiva, S.M.; Auad, S.M.; Vale, M.P. Malocclusion and oral health-related quality of life in Brazilian school children. Angle Orthod. 2013, 83, 83–89. [Google Scholar] [CrossRef]
- Sun, L.; Wong, H.M.; McGrath, C.P.J. The factors that influence the oral health-related quality of life in 12-year-old children: Baseline study of a longitudinal research. Health Qual. Life Outcomes 2017, 15, 155. [Google Scholar] [CrossRef]
- Tumurkhuu, T.; Fujiwara, T.; Komazaki, Y.; Kawaguchi, Y.; Tanaka, T.; Inazawa, J.; Ganburged, G.; Bazar, A.; Ogawa, T.; Moriyama, K. Association between maternal education and malocclusion in Mongolian adolescents: A cross-sectional study. BMJ Open 2016, 6, e012283. [Google Scholar] [CrossRef]
- Kumar, S.; Goyal, A.; Tadakamadla, J.; Tibdewal, H.; Duraiswamy, P.; Kulkarni, S. Oral health related quality of life among children with parents and those with no parents. Community Dent Health 2011, 28, 227–231. [Google Scholar] [PubMed]
- Healey, D.L.; Gauld, R.D.; Thomson, W.M. The socio-demographic and malocclusion characteristics of adolescents presenting for specialist orthodontic treatment in New Zealand practices. Aust. Orthod. J. 2015, 31, 20–25. [Google Scholar] [PubMed]
- Mtaya, M.; Brudvik, P.; Åstrøm, A.N. Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12- to 14-year-old Tanzanian schoolchildren. Eur. J. Orthod. 2009, 31, 467–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Normando, T.S.; Barroso, R.F.F.; Normando, D. Influence of the socioeconomic status on the prevalence of malocclusion in the primary dentition. Dent. Press J. Orthod. 2015, 20, 74–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joury, E.; Johal, A.; Marcenes, W. The role of socio-economic position in predicting orthodontic treatment outcome at the end of 1 year of active treatment. Eur. J. Orthod. 2011, 33, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Nalcaci, R.; Demirer, S.; Ozturk, F.; Altan, B.A.; Sokucu, O.; Bostanci, V. The Relationship of Orthodontic Treatment Need with Periodontal Status, Dental Caries, and Sociodemographic Factors. Sci. World J. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferro, R.; Besostri, A.; Denotti, G.; Campus, G. Public community orthodontics in Italy. Description of an experience. Eur. J. Paediatr. Dent. 2013, 14, 237–240. [Google Scholar] [PubMed]
- Harris, E.F.; Glassell, B.E. Sex differences in the uptake of orthodontic services among adolescents in the United States. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Agou, S.; Locker, D.; Streiner, D.L.; Tompson, B. Impact of self-esteem on the oral-health-related quality of life of children with malocclusion. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 484–489. [Google Scholar] [CrossRef]
- De Souza Barbosa, T.; Duarte Gavião, M.B.; Castelo, P.M.; Leme, M.S. Factors Associated with Oral Health-related Quality of Life in Children and Preadolescents: A Cross-sectional Study. Oral Health Prev. Dent. 2016, 14, 137–148. [Google Scholar]
- Peres, K.G.; Barros, A.J.D.; Anselmi, L.; Peres, M.A.; Barros, F.C. Does malocclusion influence the adolescent’s satisfaction with appearance? A cross-sectional study nested in a Brazilian birth cohort. Community Dent. Oral Epidemiol. 2008, 36, 137–143. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n | (%) | Mean | (SD) |
|---|---|---|---|---|
| Age | 881 | 15.55 | (1.51) | |
| 11–14 years | 177 | (20.1) | ||
| 15–16 years | 413 | (46.9) | ||
| 17–18 years | 291 | (33.0) | ||
| Gender | ||||
| Boys/Age | 360 | (40.9) | 15.55 | (1.51) |
| Girls/Age | 521 | (59.1) | 15.55 | (1.51) |
| Family affluence | ||||
| Low | 110 | (12.5) | ||
| Medium | 348 | (39.5) | ||
| High | 423 | (48.0) | ||
| ICON sum score | 881 | 39.07 | (21.03) | |
| ≤43 | 600 | (68.1) | ||
| >43 | 281 | (31.9) | ||
| Whole CPQ sum score: mean (SD) | 881 | 10.49 | (10.48) | |
| OS | 881 | 4.00 | (2.96) | |
| FL | 881 | 1.94 | (2.94) | |
| EWB | 881 | 3.30 | (4.93) | |
| SWB | 881 | 1.25 | (2.93) | |
| Whole CPQ sum score: median (IQR) | 881 | 7 | (3; 14) | |
| OS | 881 | 3 | (2; 6) | |
| FL | 881 | 1 | (1; 3) | |
| EWB | 881 | 2 | (0; 5) | |
| SWB | 881 | 0 | (0; 1) |
| Sum Scores | Whole CPQ | OS | FL | EWB | SWB | FAS |
|---|---|---|---|---|---|---|
| ICON | 0.13 ** | 0.04 | 0.02 | 0.18 ** | 0.11 ** | −0.02 |
| Whole CPQ | X | X | X | X | −0.12 ** | |
| OS | 0.39 ** | 0.39 ** | 0.31 ** | −0.09 * | ||
| FL | 0.48 ** | 0.44 ** | −0.08 * | |||
| EWB | 0.57 ** | −0.11 ** | ||||
| SWB | −0.05 |
| Variable | RSSM (95% CI) | ||||
|---|---|---|---|---|---|
| OS | FL | EWB | SWB | Whole CPQ | |
| Gender | |||||
| Boys (ref.) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Girls | 1.10 (0.9–1.28) | 1.19 * (1.00–1.41) | 1.79 *** (1.53–2.10) | 1.07 (0.89–1.29) | 1.29 *** (1.11–1.49) |
| Age | |||||
| 11–14 years (ref.) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 15–16 years | 1.10 (0.90–1.34) | 1.10 (0.89–1.38) | 0.94 (0.77–1.16) | 1.12 (0.88–1.43) | 1.05 (0.87–1.27) |
| 17–18 years | 1.16 (0.94–1.44) | 0.97 (0.76–1.22) | 1.03 (0.83–1.28) | 1.03 (0.79–1.33) | 1.06 (0.87–1.30) |
| Severity of malocclusion | |||||
| ICON sum score ≤43 (ref.) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| ICON sum score >43 | 1.02 (0.87–1.19) | 0.96 (0.81–1.15) | 1.61 *** (1.37–1.89) | 1.62 *** (1.35–1.95) | 1.24 ** (1.07–1.43) |
| Family affluence | |||||
| Low (ref.) | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Medium | 0.93 (0.73–1.18) | 0.77 * (0.59–0.99) | 0.78 * (0.61–1.00) | 0.70 * (0.53–0.92) | 0.82 (0.66–1.03) |
| High | 0.89 (0.70–1.12) | 0.69 ** (0.54–0.89) | 0.75 * (0.59–0.95) | 0.57 *** (0.44–0.75) | 0.76 * (0.61–0.95) |
| Characteristics | Estimates | ||||
|---|---|---|---|---|---|
| OS | FL | EWB | SWB | Whole CPQ | |
| Goodness-of-fit statistics: | |||||
| χ2 | 6.524 | 6.504 | 6.508 | 6.488 | 6.526 |
| Degree of freedom | 3 | 3 | 3 | 3 | 3 |
| χ2 /Degree of freedom | 2.175 | 2.168 | 2.169 | 2.164 | 2.175 |
| p | 0.089 | 0.090 | 0.089 | 0.090 | 0.089 |
| RMSEA (90% CI) | 0.026 (0–0.054) | 0.026 (0–0.054) | 0.026 (0–0.054) | 0.026 (0–0.054) | 0.026 (0–0.054) |
| CFI | 0.912 | 0.913 | 0.971 | 0.916 | 0.957 |
| IFI | 0.932 | 0.933 | 0.973 | 0.935 | 0.963 |
| Squared multiple correlations: | |||||
| CPQx sum score | 0.016 | 0.017 | 0.080 | 0.024 | 0.050 |
| Path | Way of Effect | Standardized Regression Weights | ||||
|---|---|---|---|---|---|---|
| OS | FL | EWB | SWB | Whole CPQ | ||
| ICON sum score | Direct effect | 0.041 | 0.018 | 0.202 *** | 0.112 *** | 0.142 *** |
| Gender | Direct effect | 0.081 ** | 0.045 | 0.190 *** | 0.001 | 0.123 *** |
| Indirect effect | −0.006 | −0.003 | −0.028 | −0.028 | −0.020 | |
| Total effect | 0.075 * | 0.042 | 0.162 *** | −0.019 | 0.103 *** | |
| Age | Direct effect | 0.050 * | −0.037 | −0.001 | −0.040 | −0.009 |
| Indirect effect | −0.002 | −0.001 | −0.013 | −0.007 | −0.009 | |
| Total effect | 0.048 | −0.038 | −0.014 | −0.047 | −0.018 | |
| FAS | Direct effect | −0.080 ** | −0.113 *** | −0.101 *** | −0.092 *** | −0.129 *** |
| Indirect effect | −0.003 | −0.001 | −0.014 | −0.007 | −0.010 | |
| Total effect | −0.083 ** | −0.114 ** | −0.115 ** | −0.097 *** | −0.139 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaborskis, A.; Kavaliauskienė, A.; Šidlauskas, A. Family Affluence Based Inequality in Oral Health-Related Quality of Life in a Population of Lithuanian Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 2106. https://doi.org/10.3390/ijerph16122106
Zaborskis A, Kavaliauskienė A, Šidlauskas A. Family Affluence Based Inequality in Oral Health-Related Quality of Life in a Population of Lithuanian Adolescents. International Journal of Environmental Research and Public Health. 2019; 16(12):2106. https://doi.org/10.3390/ijerph16122106
Chicago/Turabian StyleZaborskis, Apolinaras, Aistė Kavaliauskienė, and Antanas Šidlauskas. 2019. "Family Affluence Based Inequality in Oral Health-Related Quality of Life in a Population of Lithuanian Adolescents" International Journal of Environmental Research and Public Health 16, no. 12: 2106. https://doi.org/10.3390/ijerph16122106
APA StyleZaborskis, A., Kavaliauskienė, A., & Šidlauskas, A. (2019). Family Affluence Based Inequality in Oral Health-Related Quality of Life in a Population of Lithuanian Adolescents. International Journal of Environmental Research and Public Health, 16(12), 2106. https://doi.org/10.3390/ijerph16122106