Feasibility and Reliability of a Physical Fitness Test Battery in Individuals with Down Syndrome

 ,
, 
Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Design
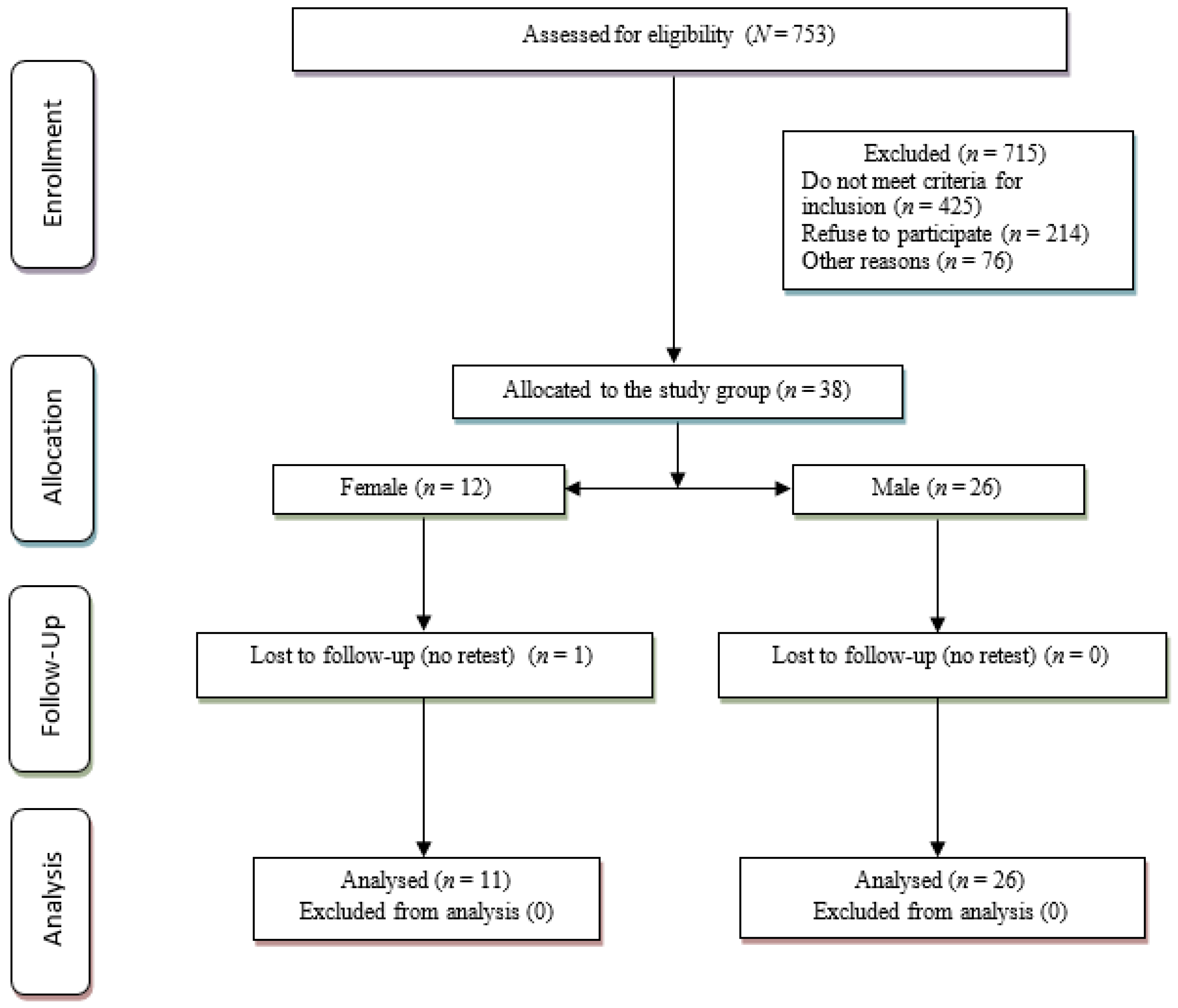
2.2. Participants
2.3. Procedures
2.4. Measurements
2.5. Body Composition (2)
2.6. Motor Fitness (1)
2.7. Musculoskeletal Fitness (4)
2.8. Cardiorespiratory Fitness (1)
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Karmiloff-Smith, A.; Al-Janabi, T.; D’Souza, H.; Groet, J.; Massand, E.; Mok, K.; Startin, C.; Fisher, E.; Hardy, J.; Nizetic, D.; et al. The importance of understanding individual differences in Down syndrome. F1000Research 2016, 5, 389. [Google Scholar] [CrossRef] [PubMed]
- De Asúa, D.R.; Parra, P.; Costa, R.; Moldenhauer, F.; Suárez, C. Evaluation of the impact of abdominal obesity on glucose and lipid metabolism disorders in adults with Down syndrome. Res. Dev. Disabil. 2014, 35, 2942–2949. [Google Scholar] [CrossRef] [PubMed]
- Cowley, P.M.; Ploutz-Snyder, L.L.; Baynard, T.; Heffernan, K.S.; Jae, S.Y.; Hsu, S.; Lee, M.; Pitetti, K.H.; Reiman, M.P.; Fernhall, B. The effect of progressive resistance training on leg strength, aerobic capacity and functional tasks of daily living in persons with Down syndrome. Disabil. Rehabil. 2011, 33, 2229–2236. [Google Scholar] [CrossRef] [PubMed]
- Sinai, A.; Hassiotis, A.; Rantell, K.; Strydom, A. Assessing Specific Cognitive Deficits Associated with Dementia in Older Adults with Down Syndrome: Use and Validity of the Arizona Cognitive Test Battery (ACTB). PLoS ONE 2016, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chen, S.; How, Y.M.; Zhang, A.L. Benefits of physical exercise intervention on fitness of individuals with Down syndrome. Int. J. Rehabil. Res. 2013, 36, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Tsimaras, V.K.; Fotiadou, E.G. Effect of Training on the Muscle Strength and Dynamic Balance Ability of Adults with Down Syndrome. J. Strength Cond. Res. 2004, 18, 343. [Google Scholar] [PubMed]
- Bossink, L.; Van Der Putten, A.A.; Vlaskamp, C. Understanding low levels of physical activity in people with intellectual disabilities: A systematic review to identify barriers and facilitators. Res. Dev. Disabil. 2017, 68, 95–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, V.; Campos, C.; Sá, A.; Cavadas, M.; Pinto, J.; Simões, P.; Machado, S.; Murillo-Rodríguez, E.; Barbosa-Rocha, N. Wii-based exercise program to improve physical fitness, motor proficiency and functional mobility in adults with Down syndrome. J. Intellect. Disabil. Res. 2017, 61, 755–765. [Google Scholar] [CrossRef]
- Cunha, A.S.; Silva-Filho, A.C.; Dias, C.J.; Durans, R.; Brito-Monzani, J.D.O.; Rodrigues, B.; Mostarda, C.T. Impacts of low or vigorous levels of physical activity on body composition, hemodynamics and autonomic modulation in Down syndrome subjects. Motriz Revista Educação Física 2018, 24, 1–8. [Google Scholar] [CrossRef]
- Ayán Pérez, C.; Martínez-Lemos, I.; Lago-Ballesteros, J.; Cancela Carral, J.M.; Loira-Camiña, N. Reliability and Validity of Physical Fitness Field-Based Tests in Down Syndrome: A Systematic Review. J. Policy Pract. Intellect. Disabil. 2016, 13, 142–156. [Google Scholar] [CrossRef]
- Cowley, P.M.; Ploutz-Snyder, L.L.; Baynard, T.; Heffernan, K.; Jae, S.Y.; Hsu, S.; Lee, M.; Pitetti, K.H.; Reiman, M.P.; Fernhall, B. Physical Fitness Predicts Functional Tasks in Individuals with Down Syndrome. Med. Sci. Sports Exerc. 2010, 42, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Ptomey, L.T.; Szabo, A.N.; Willis, E.A.; Gorczyca, A.M.; Danon, J.C.; Donnelly, J.E.; Greene, J. Changes in cognitive function after a 12-week exercise intervention in adults with Down syndrome. Disabil. Health J. 2018, 11, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Shields, N.; Bos, R.V.D.; Buhlert-Smith, K.; Prendergast, L.; Taylor, N. A community-based exercise program to increase participation in physical activities among youth with disability: A feasibility study. Disabil. Rehabil. 2018, 41, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Mihajlovic-Madzarevic, V. Appendix C: World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. In Clinical Trials Audit Preparation; Wiley: Hoboken, NJ, USA, 2010; pp. 225–229. [Google Scholar]
- Wouters, M.; Van Der Zanden, A.M.; Evenhuis, H.M.; Hilgenkamp, T.I.M. Feasibility and Reliability of Tests Measuring Health-Related Physical Fitness in Children with Moderate to Severe Levels of Intellectual Disability. Am. J. Intellect. Dev. Disabil. 2017, 122, 422–438. [Google Scholar] [CrossRef] [PubMed]
- Boer, P.; Moss, S. Test–retest reliability and minimal detectable change scores of twelve functional fitness tests in adults with Down syndrome. Res. Dev. Disabil. 2016, 48, 176–185. [Google Scholar] [CrossRef]
- Ayán-Pérez, C.; Martínez-Lemos, R.I.; Cancela-Carral, J.M. Reliability and convergent validity of the 6-min run test in young adults with Down syndrome. Disabil. Health J. 2017, 10, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Hilgenkamp, T.I.M.; Van Wijck, R.; Evenhuis, H.M. Feasibility and reliability of physical fitness tests in older adults with intellectual disability: A pilot study. J. Intellect. Dev. Disabil. 2012, 37, 158–162. [Google Scholar] [CrossRef]
- Vera-Garcia, E.; Pérez-Cruzado, D.; Cuesta-Vargas, A.I.; Mayoral-Cleries, F. Physical fitness and levels of physical activity in people with severe mental illness: A cross-sectional study. BMC Sports Sci. Med. Rehabil. 2017, 9, 17. [Google Scholar]
- Ortega, F.B.; Cadenas-Sánchez, C.; Sánchez-Delgado, G.; Mora-González, J.; Martínez-Téllez, B.; Artero, E.G.; Castro-Piñero, J.; Labayen, I.; Chillón, P.; Löf, M.; et al. Systematic Review and Proposal of a Field-Based Physical Fitness-Test Battery in Preschool Children: The PREFIT Battery. Sport. Med. 2015, 45, 533–555. [Google Scholar] [CrossRef]
- Suni, J.; Husu, P.; Rinne, M. Fitness for Health: The ALPHA-FIT Test Battery for Adults Aged 18–69-Tester’s Manual. Available online: http://www.ukkinstituutti.fi/filebank/500-ALPHA_FIT_Testers_Manual.pdf (accessed on 26 July 2019).
- Vieira, W.D.O.; Ostolin, T.L.V.D.P.; Ferreira, M.; Sperandio, E.F.; Dourado, V.Z. Test timed up and go and its correlation with age and functional exercise capacity in asymptomatic women. Fisioter. Mov. 2017, 30, 463–471. [Google Scholar] [CrossRef] [Green Version]
- Salb, J.; Finlayson, J.; Almutaseb, S.; Scharfenberg, B.; Becker, C.; Sieber, C.; Freiberger, E. Test-retest reliability and agreement of physical fall risk assessment tools in adults with intellectual disabilities. J. Intellect. Disabil. Res. 2015, 59, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Valdivia, O.D.; Cañada, M.A.M.; Ortega, F.Z.; Rodríguez, J.J.A.; Sánchez, M.F. Evolutividad de la capacidad flexora según el sexo y el nivel de enseñanza. Apunt. Med. l’Esport 2010, 44, 10–17. [Google Scholar] [CrossRef]
- Terblanche, E.; Boer, P.H. The functional fitness capacity of adults with Down syndrome in South Africa. J. Intellect. Disabil. Res. 2013, 57, 826–836. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, R.C.; Lemus, N.C. Hand Grip Strength in Adults with Intellectual Disabilities Fuerza manual de adultos con discapacidad intelectual. Apunts. Educación Física Y Deportes 2017, 3, 44–50. [Google Scholar] [CrossRef]
- Kato, T.; Miyamoto, K.; Shimizu, K. Postural reaction during maximum grasping maneuvers using a hand dynamometer in healthy subjects. Gait Posture 2004, 20, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Paz-Lourido, B.; Rodríguez, A. Physical fitness profile in adults with intellectual disabilities: Differences between levels of sport practice. Res. Dev. Disabil. 2011, 32, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Skowroński, W.; Horvat, M.; Nocera, J.; Roswal, G.; Croce, R. Eurofit Special: European Fitness Battery Score Variation among Individuals with Intellectual Disabilities. Adapt. Phys. Act. Q. 2009, 26, 54–67. [Google Scholar] [CrossRef]
- Butland, R.J.A.; Pang, J.; Gross, E.R.; Woodcock, A.A.; Geddes, D.M. Two-, six-, and 12-minute walking. Br. Med. J. 1982, 284, 1607–1608. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Atkinson, G.; Atkinson, D.G.; Nevill, A.M. Statistical Methods for Assessing Measurement Error (Reliability) in Variables Relevant to Sports Medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- Nasuti, G.; Stuart-Hill, L.; Temple, V.A. The Six-Minute Walk Test for adults with intellectual disability: A study of validity and reliability. J. Intellect. Dev. Disabil. 2013, 38, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Vis, J.C.; Thoonsen, H.; Duffels, M.G.; De Bruin-Bon, R.A.; Huisman, S.A.; Van Dijk, A.P.; Hoendermis, E.S.; Berger, R.M.; Bouma, B.J.; Mulder, B.J. Six-Minute Walk Test in Patients with Down Syndrome: Validity and Reproducibility. Arch. Phys. Med. Rehabil. 2009, 90, 1423–1427. [Google Scholar] [CrossRef] [PubMed]
- Hilgenkamp, T.I.; Van Wijck, R.; Evenhuis, H.M. Low physical fitness levels in older adults with ID: Results of the HA-ID study. Res. Dev. Disabil. 2012, 33, 1048–1058. [Google Scholar] [CrossRef] [PubMed]
- Tejero-González, C.; Martinez-Gomez, D.; Bayon-Serna, J.; Izquierdo-Gomez, R.; Castro-Piñero, J.; Veiga, O. Reliability of the Alpha Health-Related. J. Strength Cond. Res. 2013, 27, 3221–3224. [Google Scholar] [PubMed]
- Villamonte, R.; Vehrs, P.R.; Feland, J.B.; Johnson, A.W.; Seeley, M.K.; Eggett, D. Reliability of 16 Balance Tests in Individuals with Down Syndrome. Percept. Mot. Skills 2011, 111, 530–542. [Google Scholar] [CrossRef]
- Hilgenkamp, T.I.; Van Wijck, R.; Evenhuis, H.M. Physical fitness in older people with ID—Concept and measuring instruments: A review. Res. Dev. Disabil. 2010, 31, 1027–1038. [Google Scholar] [CrossRef] [PubMed]
- Hui, S.S.-C.; Yuen, P.Y. Validity of the modified back-saver sit-and-reach test: A comparison with other protocols. Med. Sci. Sports Exerc. 2000, 32, 1655–1659. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual, 2nd ed.; Human Kinetics: Pudsey, UK, 2013. [Google Scholar]
- Oppewal, A.; Hilgenkamp, T.I.M. Adding meaning to physical fitness test results in individuals with intellectual disabilities. Disabil. Rehabil 2018, 1–8. [Google Scholar] [CrossRef]
- Salaun, L.; Berthouze-Aranda, S.E. Physical Fitness and Fatness in Adolescents with Intellectual Disabilities. J. Appl. Res. Intellect. Disabil. 2012, 25, 231–239. [Google Scholar] [CrossRef]
- Van Biesen, D.; Pineda, R.C. Balance and strength assessment of Special Olympics athletes: How feasible and reliable is the Fun Fitness test battery? Eur. J. Adapt. Phys. Act. 2019, 12, 6. [Google Scholar] [CrossRef]


{kind=link}
| Physical Fitness Component | Test | n | TEST Mean (SD) | RE-TEST Mean (SD) | ICC (95% CI) | SEM | MDC | FEASIBILITY % |
|---|---|---|---|---|---|---|---|---|
| Body composition | Waist Circumference (cm) | 37 | 94.94 (14.17) | 95.51 (15.23) | 0.96 (0.928–0.981) | 2.83 | 7.84 | 98.65 |
| Body Mass Index (kg/m2) | 37 | 30.75 (6.42) | 30.58 (6.56) | 0.99 (0.971–0.992) | 0.79 | 2.20 | 100 | |
| Motor fitness | Timed Up and Go test (s) | 37 | 5.07 (1.01) | 4.92 (0.99) | 0.89 (0.787–0.942) | 0.33 | 0.93 | 100 |
| Musculoskeletal fitness | Deep Trunk Flexibility test (cm) | 37 | 32.06 (7.42) | 32.80 (7.12) | 0.87 (0.764–0.933) | 2.60 | 7.21 | 97.3 |
| Hand Grip (kg) | 37 | 21.41 (6.25) | 21.54 (6.67) | 0.90 (0.810–0.948) | 2.05 | 5.69 | 100 | |
| 10 Timed-Stand Test (s) | 37 | 21.94 (6.34) | 20.63 (6.19) | 0.80 (0.651–0.894) | 2.77 | 7.69 | 97.3 | |
| 30-s Sit-Up (number) | 37 | 15.22 (5.27) | 15.48 (5.11) | 0.80 (0.628–0.899) | 2.31 | 6.40 | 82.45 | |
| Cardiorespiratory fitness | 6-Min Walk Test (m) | 37 | 463.08 (82.14) | 457.44 (93.73) | 0.77 (0.595–0.874) | 42.26 | 117.14 | 98.65 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabeza-Ruiz, R.; Alcántara-Cordero, F.J.; Ruiz-Gavilán, I.; Sánchez-López, A.M. Feasibility and Reliability of a Physical Fitness Test Battery in Individuals with Down Syndrome. Int. J. Environ. Res. Public Health 2019, 16, 2685. https://doi.org/10.3390/ijerph16152685
Cabeza-Ruiz R, Alcántara-Cordero FJ, Ruiz-Gavilán I, Sánchez-López AM. Feasibility and Reliability of a Physical Fitness Test Battery in Individuals with Down Syndrome. International Journal of Environmental Research and Public Health. 2019; 16(15):2685. https://doi.org/10.3390/ijerph16152685
Chicago/Turabian StyleCabeza-Ruiz, Ruth, Francisco Javier Alcántara-Cordero, Isaac Ruiz-Gavilán, and Antonio Manuel Sánchez-López. 2019. "Feasibility and Reliability of a Physical Fitness Test Battery in Individuals with Down Syndrome" International Journal of Environmental Research and Public Health 16, no. 15: 2685. https://doi.org/10.3390/ijerph16152685
APA StyleCabeza-Ruiz, R., Alcántara-Cordero, F. J., Ruiz-Gavilán, I., & Sánchez-López, A. M. (2019). Feasibility and Reliability of a Physical Fitness Test Battery in Individuals with Down Syndrome. International Journal of Environmental Research and Public Health, 16(15), 2685. https://doi.org/10.3390/ijerph16152685