3. Results
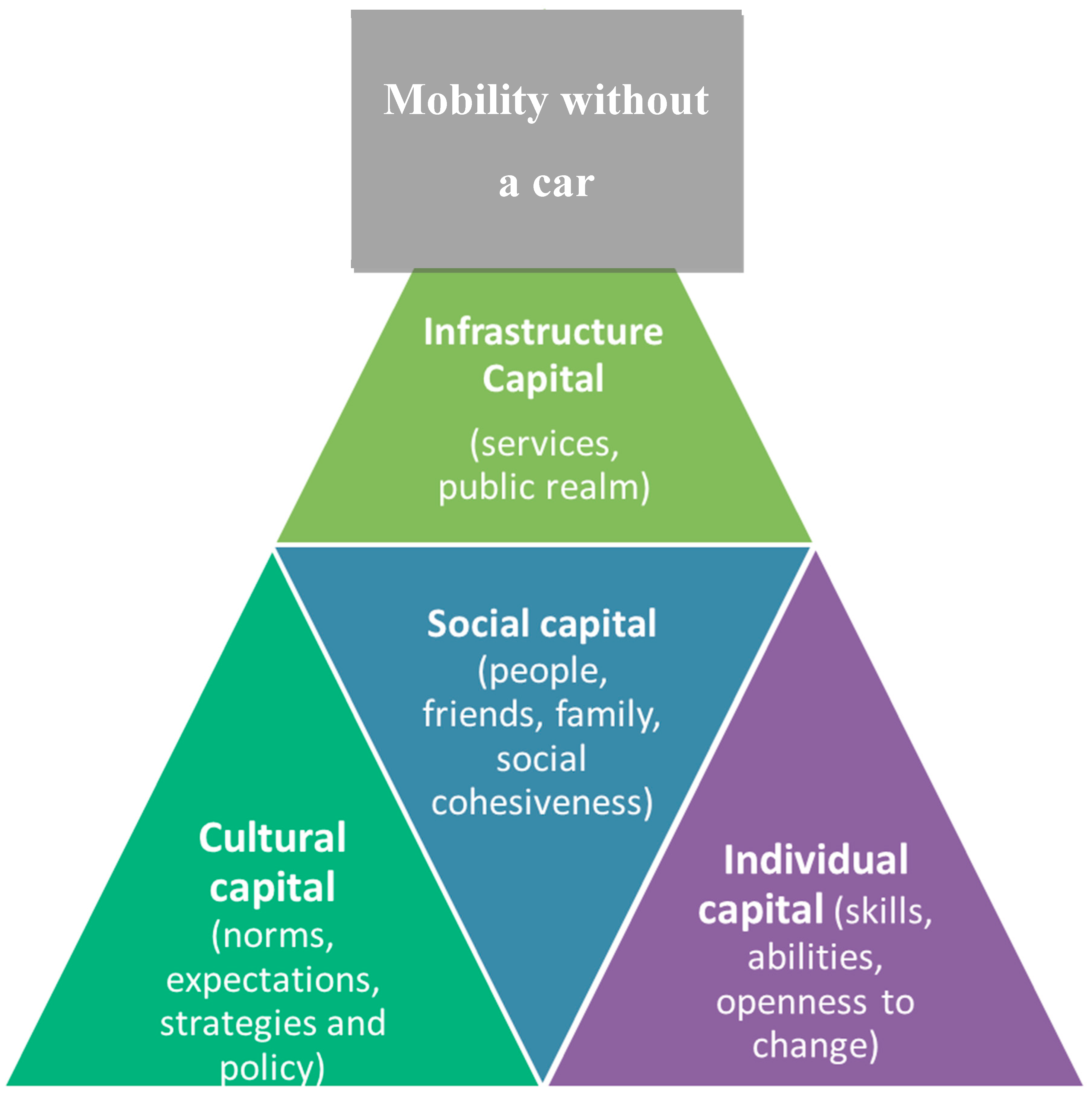
From the initial model of social, cultural and economic capital, the first two categories were distinctly noticeable in the findings. Two additional categories were added, one of which encompasses economic capital in this instance, but goes wider than just being monetary based. The provision of infrastructure and services themselves was frequently mentioned, and it was deemed this could become an additional category that also contained economic capital. Termed infrastructure capital, this was having the necessary resource to carry out the mobility that is provided in the local areas and is somewhat out of the individual’s control. Finally, individual resilience was also described, and this is included in an additional category, as again it does not quite fit the categories of social, cultural, economic or infrastructure.
3.1. Infrastructure Capital
The category with the most response within, both in terms of depth and description but also most frequently mentioned belonged to infrastructure. Older people mentioned how important it was that there had to be the right provision of services, support and hard infrastructure for individuals to be able to access transport beyond the car. Economic capital forms part of this, especially with regard to public bus use in the UK, as it includes free use of buses,
“Well luckily the buses are free. Makes a huge difference. I wouldn’t go out half as much as I do.” (female, aged 77, bus user)
Older people who had good-quality bus services were far more likely to be able to give up driving with fewer problems, but there was a noticeable feeling of being lucky to be on a bus route,
“Well we’re lucky, lucky for now at least, we’ve plenty of buses get us into town and that’s where we want to go and the other way they go on to the coast, so we can go there too.” (female, aged 77, bus user)
And that some people were “out of luck” by not being on a bus route, especially if it had had buses taken off that route,
“They reduced the service down and down and then nothing. One day just took it away. We’re on a Sunday only route but I want to use the bus everyday.” (male, aged 81, lifts from friends and family)
Poor services running on routes were noted, especially around the time of the day services ran, sometimes people wanted to travel at very different times and frequencies than the service provided,
“We are on a bus route, but we can’t use it, well not often, in fact we don’t tend to at all, because there is just one service in and one service out of the city. The one service in is like 8am and one service back isn’t until 4pm. We might, well usually we just want to be there for an hour or two you know.” (female, aged 83, lifts from family and friends)
Car users predicted that the provision of services could never match up to their ability to drive when and where they wanted and often this worried them,
“I go loads of places in my car. It’s so convenient. I mean what am I going to do if I have to give-up. The buses won’t go anywhere near where I want them to go! I’ll be stuck.” (male, aged 80, car driver)
The service was also seen as poor if there were concerns about the bus driver, the lowering of the floor of the bus to accommodate easy access and not being enough room on the buses,
“It’s the quality of the buses really. The actual bus service too. Whether it stops low enough to get on without a step. And the driver doesn’t drive off before I sit down. Big barriers to me!” (female, aged 77, bus user)
Similarly, with regard to walking, the importance of having quality infrastructure to be able to walk on is important, including pavement being in good condition,
“There is a pavement, but it is in such bad state of repair, I have to walk on the road but I hate that.” (female, aged 80, walker)
Crossing the road was a frequently mentioned issue for older people,
“There is a busy road I always struggle with, it’s walking round a long way to the crossing or taking your life in your hands. At my age you can’t do that.” (male, aged 77, walker)
Not having enough room to walk was often mentioned too, for example, sharing space with other users or items,
“The pavement is used by so many other things, cyclists, bins, parked cars, it’s just too narrow.” (female, aged 81, walker)
3.2. Social Capital
The next most frequently and vociferously mentioned answers belonged around social capital. Older people relied very much on the support of others to help them with literal mobility, replacing journeys they would have made driving themselves with journeys as passengers in other people’s cars. This was easy when someone was travelling to the same place anyway, and this had a sense of altruism, of helping others associated with it, which was enjoyed by the driver,
“I pick up two people to take them for church on Sunday morning. I don’t mind. I like to provide them with help. Goodness knows they wouldn’t be able to get there without it. And it’s important to them.” (female, aged 73, car driver)
This was not necessarily always from someone well known to the individual, especially if traveling to the same location. Sometimes a neighbour or someone in the community offered this support. It was noted how this created a sense of friendship for some,
“I’m so grateful for [‘name’] for giving me a lift, we’ve become close friends. We realised we lost our husband around the same time from a similar illness. So yes a source of friendship and yes comfort.” (female, aged 82, lifts from family and friends)
However, on other occasions, having family or close friends nearby resulted in providing practical support, which was very welcome,
“Thank goodness I have my daughter living nearby, otherwise I’d go stir crazy not going out.” (female, aged 86, lifts from family and friends)
However, receivers of literal mobility often felt very guilty of being a burden on others and used techniques to deal with that, including reciprocation,
“I pay back my lifts. When my son or daughter-in-law give me lifts, I’ll make sure I’ve baked them a cake or paid my way somehow.” (female, aged 86, lifts from family and friends)
Although usually the support given for mobility was welcomed, people still lamented that their mobility was not as good as it once was when they were drivers,
“Yes I get lifts now all the time, but it isn’t the same, it’s hard to explain, I suppose you can’t go when you want. I don’t go when I want now.” (female, aged 80, lifts from family and friends)
Support was also linked to nonliteral mobility, helping others to get things in that they would have got using their car, but that they can’t now they walk or use the bus. This was often related to a sense of good feeling within a community or neighbourhood,
“What’s lovely ‘round here is the help I get. I mean my neighbour, he makes sure I’m ok. He gets me in a pint of milk, or something I can’t or struggle to carry on the bus.” (male, aged 80, bus user)
This was also noted in that some areas seem to have more support than others, though discussions on this were more anecdotal than discussing people’s own experiences,
“It wouldn’t have happened back where I lived, it wouldn’t. People didn’t know each other, so they didn’t look out for each other at all, didn’t care, here its different.” (female, aged 77, walker)
It was, though, rather rare for the participants to talk about receiving emotional support from others in giving up driving,
“I think I went 6 months through some kind of grieving process when the doc took away my keys. I didn’t seek help but I also didn’t get any sympathy. You’re expected just to get on aren’t you, now you’re old.” (male, aged 80, walker)
It was also rare to find lifts given out for what might be termed discretionary activities, for mobility for its own sake,
“I can’t get out and about so much like I used to. I miss going to the sea for an ice cream by the beach. There is no bus there. I can’t really ask my busy family!” (female, aged 80, bus user)
Much of the social capital stems from “soft” support, within family and friends and within communities, though it was noted by a few participants that social support within informal or even formal groups can help with mobility,
“Having a walking group got me walking again. I’ve always been interested, always enjoyed walking, but I’d got out of it and I thought I was too old and fat, but they, well we, support one another and now I walk everywhere.” (female, aged 76, walker)
3.3. Cultural Capital
The final two categories both received around equal attention from older people and supported the social and infrastructure capital. Cultural capital stems from the surrounding environment, whereas individual capital comes from within.
Sometimes cultural capital created a frustration, rather than a resource to draw upon. The car was seen as a norm in society, and people missed doing the journeys they used to do and had got used to doing and were seen as part of the normal everyday, and this had negative affective consequences for the individual,
“to think I can’t even get to the hospital easily just makes me feel a failure.” (male, aged 80, bus user)
The opposite was true for people who had been less wedded to their car throughout their lifecourse, for example, people who had been highly multimodal,
“Well I’ve been using the bus to get to town now anyway for a while. So I’m used to it.” (female, bus user, aged 81)
Also, there was a feeling among the participants that different locations could have different cultural capital,
“well if I lived in London it would be different. I lived there in the 90s. There is so much public transport. And you know everyone uses it. No one really has a car you know.” (male, aged 86, bus user)
A hierarchy of norms of use appeared among the participants, car use was seen as the most normal everyday form of transport, with driving at the top followed by being a passenger, followed by using a bus, but then walking and cycling were seen as going against the norms of society for older people,
“Yeah walking is still not normal especially for doing things. I mean part of it is the practicalities of carrying stuff but also people don’t walk now do they. Not unless it’s for leisure.” (male, aged 72, walker)
Another gap in cultural capital noted by participants was the lack of being involved in decisions affecting their transport systems,
“Look I don’t know if it is the kind of thing that would do any good, but I, we, don’t have any say in the transport we have around here. We need to know when services are stopping and we need to stop them doing it. It’s odd they ask us our opinion on loads of stuff but not transport. Like a secret brotherhood.” (male, aged 82, bus user)
3.4. Individual Capital
There were incidences where the individual’s own experience, attitude or values supported mobility without a car. Being able to use a mode of transport requires some ability to use it, knowledge of how to use it and understanding of the norms, and older people discussed this with regards to buses,
“Well I’ve always used the bus to go into town, it’s just easier, then when I had to use more buses because we’d given up driving, it wasn’t so much of a shock really.” (female, aged 88, bus).
With regards to walking, there is a similar need to be able to walk but also to be able to be personally resilient in obstacles, such as a feeling of needing good balance or good hearing and observation skills,
“To get over all the cracks in the pavement you need great balance, I haven’t always got that now, I’m worried about falling.”(female, aged 80, walker)
“You need good hearing and need your wits about you. Cyclist come up right behind.” (male, aged 70, walker)
Some older people talked about having a personality that meant they were open to change, which helped when giving up driving, openness to trying new forms of transport,
“I saw it as a challenge, and it was a challenge I can tell you. But I challenged myself to using the bus. I hadn’t used them for years, so I was intrigued, and I’ve actually enjoyed it. Haven’t looked back.” (male, aged 80, bus user)
Similarly, some older people talked about being open to visiting new places,
“Well you can’t actually go on the bus to where I’d normally do my shopping, so I now go somewhere different, somewhere I wouldn’t normally have gone and I actually have enjoyed the change.” (female, aged 75, bus user)
4. Discussion
In terms of importance, infrastructure capital, drawing on provision of services, hard infrastructure and economic costs of transport provision seem to be the highest priority for older people. It was this capital that contained so many barriers and enablers. Where this capital was found in abundance, older people felt able to cope with the loss of giving up driving. The provision of bus services, of good walkable neighbourhoods placated the negative side effects of not driving. These included having good-quality bus services going to a range of places, or at least where people want them to go, on good-quality, easily accessible buses, with driver sympathetic to the needs of older people, as has been suggested as important in previous research [
22,
23]. The provision of quality pavements including well-maintained, continuous surfaces segregated from other users, with good crossing facilities helped people stay mobile, again similar to previous research [
8]. However, these alone are not enough. It is unlikely the same levels of mobility or of need can be accessed through infrastructure alone, and it is likely social capital is needed to plug many gaps in provision. Drawing on friends and family was often cited as plugging mobility gaps by provision of literal mobility, as noted in previous research [
4,
25]. Again, there are noticeable gaps in social capital, especially emotive and discretionary activities not being fulfilled, as have been noted previously by Murray and Musselwhite [
25]. Also, drawing on both these levels of resource can be supported by cultural capital by having norms surrounding use of public transport and of walking, often which were missing, according to the older people in this research. Previous research [
5,
6,
8] noted that the car dominates norms in society, with older people particular excluded, who give up driving. There was also a feeling that outside of major cities, especially outside of London in the UK, having cultural capital in the form of support from age-friendly policies and transport policies in general were lacking. Finally, these levels of resource also require an amount of individual capital, an ability to be able to use public transport, to know how to use it and to understand how to operate it, similarly, an ability in being able to walk and a desire to take part in something new and potential for changing travel behaviour. Having a gap in any of the four levels of capital reduces the ability for older people’s mobility when they give up driving.
Figure 1 outlines the relationship between the capitals, showing how infrastructure is of highest importance to older people, followed by social capital, supported by cultural and individual capital.
Capitals are not always a resource to draw upon in a positive sense. The norms of a society geared around the car, in line with previous research [
8], mean not using a car in later life leaves a big gap in cultural resource. It is a particular concern to older people in that mobility through driving a car represents a feeling of youthfulness and belonging and being part of society [
5,
6]. In terms of social capital, it cannot always be drawn upon in full due to feelings of being a burden and difficulties or challenges in reciprocation, which has been documented in previous research [
4,
25]. In addition, the social capital does not always deliver exactly the levels of mobility expected and wanted. In particular, emotional support of social capital is not always evident, despite being in demand, as has been found similarly in previous research, practical support is easier to provide than emotional support [
25]. Also, how social capital does not plug the gap of journeys for discretionary purposes or for their own sake, as previous research has found, people felt they can ask for a journey to a hospital but not to a coffee shop or to the seaside, and older people really miss such journeys [
38,
39].
In terms of the gap in cultural capital where transport policies and practice do not cover ageing populations well, there is a need perhaps for more involvement in social capital. Older people generally felt they would like more involvement in the shaping of mobility services in their local areas. There is a chance to utilise social capital and move it in the direction of cultural capital, to create transport action groups among older people to feed into transport planning. Public involvement in services, through co-development for example, is beginning to take shape in redesigning urban areas, for example, collaborative, redistributive urbanism and intergenerational urbanism [
40,
41], and transport needs to follow suit.
Capitals not only vary between people, but vary from place to place. This is very much in evidence for cultural capital, where norms can help people be more mobile in some places than in others. In cities, use of public transport, especially buses, is higher than in rural areas, some of this is provision, but it also effects norms through ownership of cars. Those who have got used to using alternative transport to the car have higher levels of individual capital in skills and knowledge, but also this is greater if cultural capital in terms of norms supports these skills and abilities. This is similar to being “public transport” ready, as noted through motility [
34]. Women tend to have higher levels of public transport knowledge, having been more multimodal throughout life than men, who are more wedded to their car [
8]. This helps them in later life when giving up driving. There did not seem to be any social capital differences between men and women and support groups. Both groups were equally able to use social capital to help when driving had ceased, both drawing on family and friends if they could, but also on local community support. People attributed the ability to draw on wider community support from people outside of their family and friend networks on having a cohesive and friendly local area to live in. This links to a social cohesive element on social capital. It is beyond the scope of this paper to be able to identify if some areas have higher social cohesion than others, but it is certainly noted as a thread stemming from the participants themselves.
Although this was a project carried out with relatively few people in one geographic location in the UK, making it hard to generalise to different contexts, the in-depth nature of the research adds extra dimensions to the findings, noting variance between and within individuals and their capitals. It would be useful to now ascertain if this model is present in other contexts, especially in places where it might be assumed capital might vary hugely, for example different geographical locations and in different cultures. It might also be useful to enumerate some of the findings to address how to overcome gaps in capital, helping to prioritise the best interventions. How far the capitals might change in future ageing populations will also be interesting. How will an increase in older people who are more wedded to their cars than ever cope with giving up driving in later life, as will be found in western societies over the next 20–30 years? How will changes in transport provision, mobility as a service, potential of increased sharing mobility services or the promise of increasingly automated vehicles alter the capitals, for example? Finally, changes in the nature of work for older people, potentially working later on in life, will alter the need for mobility and transport, and in turn affect how people will draw on capitals.





{kind=link}