Persistent Hearing Loss among World Trade Center Health Registry Residents, Passersby and Area Workers, 2006–2007

Abstract
1. Introduction
2. Methods
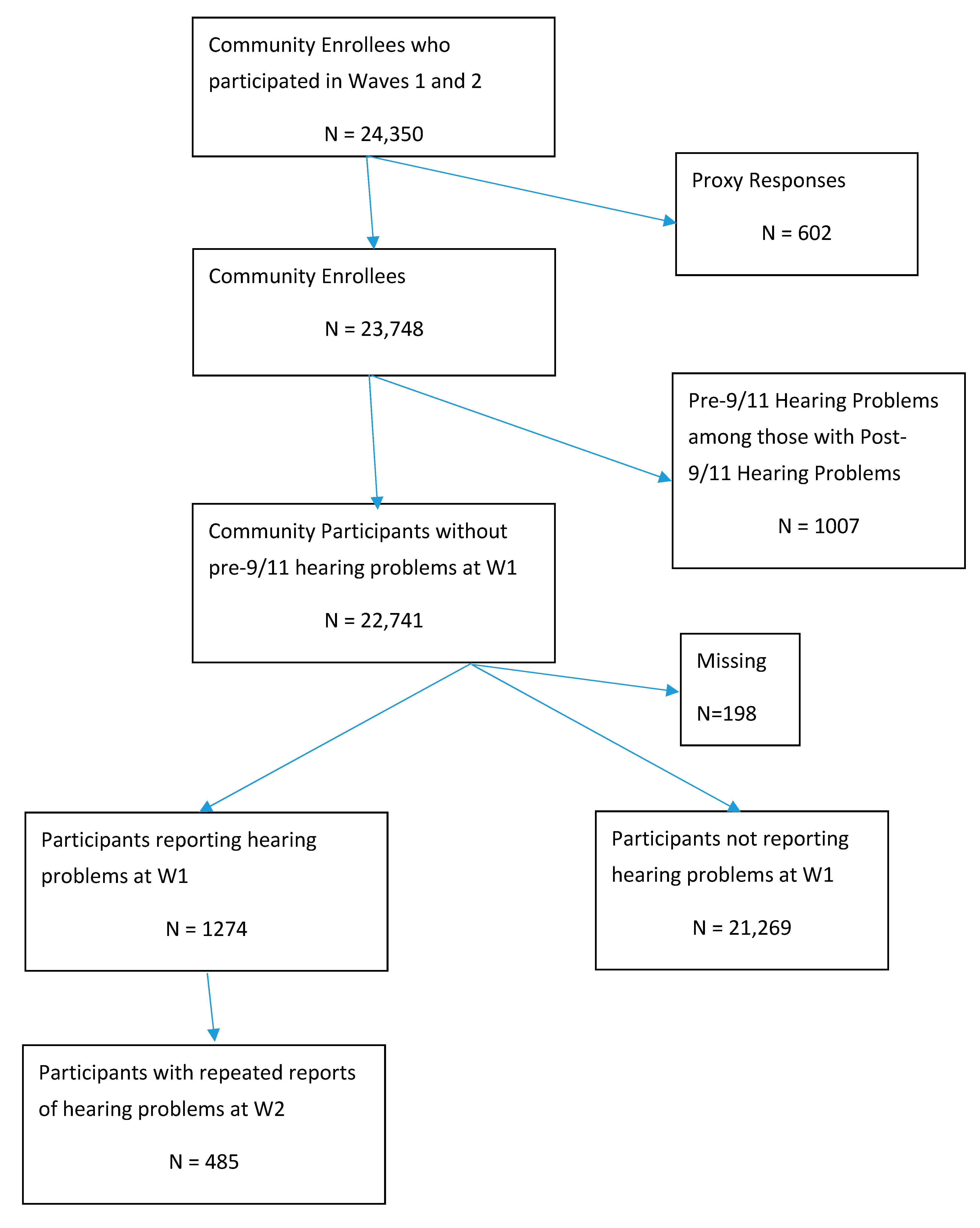
2.1. Study Population
2.2. Exposure Assessment
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- Brackbill, R.M.; Thorpe, L.E.; DiGrande, L.; Perrin, M.; Sapp, J.H., 2nd; Wu, D.; Campolucci, S.; Walker, D.J.; Cone, J.; Pulliam, P.; et al. Surveillance for World Trade Center disaster health effects among survivors of collapsed and damaged buildings. MMWR Surveill. Summ. 2006, 55, 1–18. [Google Scholar] [PubMed]
- Stein, C.R.; Lee, D.J.; Flamme, G.A.; Cone, J.E. Persistent Post-9/11 Hearing Problems Among World Trade Center Health Registry Rescue and Recovery Workers, 2001 to 2007. J. Occup. Environ. Med. 2017, 59, 1229–1234. [Google Scholar] [CrossRef] [PubMed]
- Colbeth, H.L.; Zeig-Owens, R.; Liu, Y.; Webber, M.P.; Schwartz, T.M.; Hall, C.B.; Prezant, D.J. Persistent self-reported ear and hearing problems among World Trade Center-exposed firefighters and emergency service workers, 2001–2007. Am. J. Ind. Med. 2019, 62, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Flamme, G.A.; Goldfarb, D.G.; Zeig-Owens, R.; Hall, C.B.; Vaeth, B.M.; Schwartz, T.; Yip, J.; Vossbrinck, M.; Stein, C.R.; Friedman, L.; et al. Hearing loss among World Trade Center Firefighters and Emergency Medical Service Workers. J. Occup. Environ. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Remenschneider, A.; Lookabaugh, S.; Aliphas, A.; Brodsky, J.R.; Devaiah, A.K.; Dagher, W.; Grundfast, K.M.; Heman-Ackah, S.E.; Rubin, S.; Sillman, J.; et al. Otologic outcomes after blast injury: The Boston Marathon Experience. Otol. Neurotol. 2014, 35, 1825–1834. [Google Scholar] [CrossRef] [PubMed]
- Campo, P.; Morata, T.; Hong, O. Chemical exposure and hearing loss. Dis. Mon. 2013, 59, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Lioy, P.J.; Weisel, C.P.; Millette, J.R.; Eisenreich, S.; Vallero, D.; Offenberg, J.; Buckley, B.; Turpin, B.; Zhong, M.; Cohen, M.D.; et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ. Health Perspect. 2002, 110, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Farfel, M.; DiGrande, L.; Brackbill, R.; Prann, A.; Cone, J.; Friedman, S.; Walker, D.J.; Pezeshki, G.; Thomas, P.; Galea, S.; et al. An overview of 9/11 experiences and respiratory and mental health conditions among World Trade Center Health Registry enrollees. J. Urban Health 2008, 85, 880–909. [Google Scholar] [CrossRef] [PubMed]
- Wave 2 WTCHR Survey; NYC DOHMH: New York, NY, USA, 2006. Available online: https://www1.nyc.gov/assets/911health/downloads/pdf/wtc/adult_survey2006-2007.pdf (accessed on 8 October 2019).
- Wave 1 WTCHR Survey; NYC DOHMH: York, NY, USA, 2003. Available online: https://www1.nyc.gov/assets/911health/downloads/pdf/wtc/wtc-questionnaire.pdf (accessed on 8 October 2019).
- Yang, D.; Dalton, J. A Unified Approach to Measuring the Effect Size between Two Groups Using SAS. In SAS Global Forum. 2012. Available online: http://support.sas.com/resources/papers/proceedings12/335-2012.pdf (accessed on 8 October 2019).
- Sherman, L.; Pelter, M.A.; Deamer, R.L.; Duan, L.; Batech, M. Association between encounter frequency and time to blood pressure control among patients with newly diagnosed hypertension. J. Clin. Hypertens. 2017, 20, 429–437. [Google Scholar] [CrossRef]
- Shiue, I. Chronic diseases and life events accounted for 2–18% population attributable risks for adult hearing loss—UK Adult Psychiatric Morbidity Survey, 2007. Eur. Arch. Oto-Rhino-Layrngol. 2016, 273, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Platz, E.; Niparko, J. Risk factors for hearing loss in US Adults—Data from the National Health and Nutrition Examination Survey, 1999–2002. Otol. Neurotol. 2009, 30, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Swan, A.; Nelson, J.T.; Swiger, B.; Jaramillo, C.A.; Eapen, B.C.; Packer, M.; Pugh, M.J. Prevalence of hearing loss and tinnitus in Iraq and Afghanistan Veterans: A chronic effects of neurotrauma consortium study. Hear. Res. 2017, 349, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Lippmann, M.; Cohen, M.D.; Chen, L.C. Health effects of World Trade Center (WTC) Dust: An unprecedented disaster’s inadequate risk management. Crit. Rev. Toxicol. 2015, 45, 492–530. [Google Scholar] [CrossRef] [PubMed]
- Cruickshanks, K.; Dhar, S.; Dinces, E.; Fifer, R.C.; Gonzalez, F., 2nd; Heiss, G.; Hoffman, H.J.; Lee, D.J.; Newhoff, M.; Tocci, L.; et al. Hearing impairment prevalence and associated risk factors in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). JAMA Otolaryngol. Head Neck Surg. 2015, 141, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kari, E.; Friedman, R.A.; Fisher, L.M. Prevalence of hearing loss and hearing care use among Asian Americans—A nationally representative sample. Otol. Neurotol. 2017, 39, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Arslan, Y.; Arslan, İ.B.; Aydin, H.; Yağz, Ö; Tokuçoğlu, F.; Çkurova, İ. The etiological relationship between migraine and sudden hearing loss. Otol. Neurotol. 2017, 38, 1411–1414. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization. Acoustics—Estimation of Noise-Induced Hearing Loss; ISO 1999:2013; ISO: Geneva, Switzerland, 2018. [Google Scholar]
- Preventing Hearing Loss Caused by Chemical (Ototoxicity) and Noise Exposure; National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 2018.
- Hain, T.; Micco, A. Cranial Nerve 8: Vistobulocohlear Nerve. In Textbook of Neurology, 2nd ed.; Goetz, C.D., Ed.; Saunders: Philadelphia, PA, USA, 2003. [Google Scholar]
- Zhang, X.; Ni, Y.; Liu, Y.; Zhang, L.; Zhang, M.; Fang, X.; Yang, Z.; Wang, Q.; Li, H.; Xia, Y.; et al. Screening of noise-induced hearing loss-associated SNPs and the assessment of its genetic susceptibility. Environ. Health 2019, 18, 30. [Google Scholar] [CrossRef] [PubMed]
- Gargano, L.M.; Ni, Y.; Liu, Y.; Zhang, L.; Zhang, M.; Fang, X.; Yang, Z.; Wang, Q.; Li, H.; Xia, Y.; et al. Review of Non-Respiratory, Non-Cancer Physical Health Conditions from Exposure to the World Trade Center Disaster. Int. J. Environ. Res. Public Health 2018, 15, 253. [Google Scholar] [CrossRef] [PubMed]
- Wisnivesky, J.P.; Teitelbaum, S.L.; Todd, A.C.; Boffetta, P.; Crane, M.; Crowley, L.; de la Hoz, R.E.; Dellenbaugh, C.; Harrison, D.; Herbert, R.; et al. Persistence of multiple illnesses in World Trade Center rescue and recovery workers: A cohort study. Lancet 2011, 378, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Hong, O.; Chin, D.L.; Samo, D.G. Hearing loss and use of hearing protection among career firefighters in the United States. JOEM 2013, 55, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Van Haesendonck, G.; Van Rompaey, V.; Gilles, A.; Topsakal, V.; Van de Heyning, P. Otologic outcomes after blast injury: The Brussels Bombing experience. Otol. Neurotol. 2018, 39, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Kleber, R.J. Trauma and Public Mental Health: A Focused Review. Front. Psychiatr. 2019, 10, 451. [Google Scholar] [CrossRef] [PubMed]
- Murdock, K.W.; Stowe, R.P.; Peek, M.K.; Lawrence, S.L.; Fagundes, C.P. An Evaluation of Perceived Health Risk and Depressive Symptoms Before a Disaster in Predicting Postdisaster Inflammation. Psychosom. Med. 2018, 80, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Ozbay, F.; Auf der Heyde, T.; Reissman, D.; Sharma, V. The enduring mental health impact of the September 11th terrorist attacks: Challenges and lessons learned. Psychiatr. Clin. N. Am. 2013, 36, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S.E.; Friedman, S.; Galea, S.; Nair, H.P.; Eros-Sarnyai, M.; Stellman, S.D.; Hon, J.; Greene, C.M. Short-term and medium-term health effects of 9/11. Lancet 2011, 378, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Canlon, B.; Theorell, T.; Hasson, D. Associations between stress and hearing problems in humans. Hear. Res. 2013, 295, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Herr, R.M.; Bosch, J.A.; Theorell, T.; Loerbroks, A. Bidirectional associations between psychological distress and hearing problems: An 18-year longitudinal analysis of the British Household Panel Survey. Int. J. Audiol. 2018, 57, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Horner, K.C. The emotional ear in stress. Neurosci. Biobehav. Rev. 2003, 27, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Herranen, A.; Ikäheimo, K.; Virkkala, J.; Pirvola, U. The Stress Response in the Non-Sensory Cells of the Cochlea Under Pathological Conditions-Possible Role in Mediating Noise Vulnerability. J. Assoc. Res. Otolaryngol. 2018, 19, 637–652. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; West, M.B.; Cai, Q.; Cheng, W.; Ewert, D.L.; Li, W.; Floyd, R.A.; Kopke, R.D. Antioxidants reduce neurodegeneration and accumulation of pathologic Tau proteins in the auditory system after blast exposure. Free Radic. Biol. Med. 2017, 108, 627–643. [Google Scholar] [CrossRef] [PubMed]
- Forman-Hoffman, V.; West, M.B.; Cai, Q.; Cheng, W.; Ewert, D.L.; Li, W.; Floyd, R.A.; Kopke, R.D. Psychological and Pharmacological Treatments for Adults with Posttraumatic Stress Disorder: A Systematic Review Update; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2018.
- Cima, R.F.; Andersson, G.; Schmidt, C.J.; Henry, J.A. Cognitive-behavioral treatments for tinnitus: A review of the literature. J. Am. Acad. Audiol. 2014, 25, 29–61. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, D.; Lucas, J.; Clarke, T. Summary health statistics for U.S. Adults: National Health Interview Survey, 2012. Vital Health Stat. 2014, 260, 1–161. [Google Scholar]
- Li, C.; Zhang, X.; Hoffman, H.J.; Cotch, M.F.; Themann, C.L.; Wilson, M.R. Hearing impairment associated with depression in US adults, National Health and Nutrition Examination Survey 2005–2010. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Mick, P.; Kawachi, I.; Lin, F. The association between hearing loss and social isolation in older adults. Otolaryngol. Head Neck Surg. 2014, 150, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.; Gilham, B.; Cardinal, B. Association between accelerometer assessed physical activity and objectively measured hearing sensitivity among U.S. adults with diabetes. Res. Q. Exerc. Sport 2014, 85, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Souza, P.; Hoover, E. The physiologic and psychophysical consequences of severe-to-profound hearing Loss. Semin. Hear. 2018, 39, 349–363. [Google Scholar]


{kind=link}
| Full Population (n = 22,741) | ||||
|---|---|---|---|---|
| Persistent Hearing Loss | ||||
| Characteristic | Yes N (row percent) | No N (row percent) | Standardized Difference a | Statistical Significance |
| Total (missing = 679) | 485 (2.2) | 21,577 (97.8) | ||
| Dust Cloud Exposure | 0.47 | p < 0.0001 | ||
| Not in dust cloud | 116 (1.3) | 8626 (98.6) | ||
| In dust cloud, able to hear | 242 (2.2) | 10,870 (97.8) | ||
| In dust cloud, not able to hear | 102 (5.7) | 1687 (94.3) | ||
| Survey Mode, Wave 2 | 0.26 | p < 0.0001 | ||
| Web | 167(1.6) | 9989 (98.4) | ||
| Phone | 62 (2.2) | 2751 (97.8) | ||
| Paper | 256 (2.8) | 8837 (97.2) | ||
| Age at Wave 2, years (mean, Standard Deviation) | 53.2 (11.7) | 47.4 (12.0) | 0.49 | p < 0.0001 |
| Sex | 0.08 | p = 0.08 | ||
| Female | 280 (2.4) | 11,602 (97.6) | ||
| Male | 205 (2.0) | 9975 (98.0) | ||
| Race/Ethnicity | 0.44 | p < 0.0001 | ||
| Non-Hispanic White | 227 (1.6) | 14,135 (98.4) | ||
| Non-Hispanic Black | 72 (2.6) | 2749 (97.5) | ||
| Hispanic | 122 (5.1) | 2283 (94.9) | ||
| Asian | 46 (2.7) | 1667 (97.3) | ||
| Other | 18 (2.4) | 743 (97.6) | ||
| Education | 0.34 | p < 0.0001 | ||
| Less than high school | 35 (6.2) | 553 (93.8) | ||
| High school graduate | 207 (2.9) | 6890 (97.1) | ||
| College graduate | 242 (1.7) | 14,033 (98.3) | ||
| Smoking History, Wave 2 | 0.06 | p = 0.38 | ||
| Never | 259 (2.1) | 12,154 (97.9) | ||
| Former | 153 (2.3) | 6533 (97.7) | ||
| Current | 69 (2.5) | 2725 (97.5) | ||
| Sinus Symptoms b | 0.65 | p < 0.0001 | ||
| No | 176 (1.2) | 14,487 (98.8) | ||
| Yes | 300 (4.2) | 6842 (95.8) | ||
| Headache Symptoms b | 0.65 | p < 0.0001 | ||
| No | 293 (1.5) | 19,023 (98.5) | ||
| Yes | 178 (7.0) | 2382 (93.1) | ||
| PTSD Symptoms b | 0.75 | |||
| No | 260 (1.4) | 18,510 (98.6) | ||
| Yes | 170 (8.3) | 1883 (91.7) | ||
| Chronic Disease History c | 0.43 | |||
| No | 191 (1.4) | 13,126 (98.5) | ||
| Yes | 277 (3.3) | 8132 (96.7) | ||
| Unadjusted OR (95% CI) | Adjusted OR (95% CI) | |
|---|---|---|
| 9/11 Exposure | ||
| Not in dust cloud | 1.0 | 1.0 |
| In dust cloud, able to hear | 1.7 (1.3, 2.1) | 1.4 (1.1, 1.7) |
| In dust cloud, not able to hear | 4.5 (3.4, 5.9) | 3.0 (2.2, 4.0) |
| Mode Paper vs. web | 1.7 (1.4, 2.1) | 1.1 (0.9, 1.4) |
| Mode Phone vs. web | 1.3 (1.0, 1.8) | 1.2 (0.9, 1.7) |
| Age (years) | 1.0 (1.0, 1.0) | 1.04 (1.03,1.05) |
| Sex Male vs. Female | 0.9 (0.7, 1.0) | 1.1 (0.9, 1.4) |
| Race/ethnicity | ||
| Non-Hispanic Black vs. Non-Hispanic White | 1.6 (1.2, 2.1) | 1.0 (0.73,1.4) |
| Asian vs. Non-Hispanic White | 1.7 (1.2, 2.4) | 1.6 (1.1, 2.2) |
| Hispanic vs. Non-Hispanic White | 3.3 (2.7, 4.2) | 2.3 (1.7, 3.0) |
| Other vs. Non-Hispanic White | 1.5 (0.9, 2.5) | 0.9 (0.5, 1.6) |
| Education < High School vs. College Graduate | 3.8 (2.6, 5.5) | 1.3 (0.8, 1.3) |
| Education High School Graduate vs. College Graduate | 1.7 (1.4, 2.1) | 1.0 (0.8, 1.3) |
| Smoking History-Current vs. Never | 1.2 (0.9, 1.6) | 1.0 (0.8, 1.3) |
| Smoking History-Former vs. Never | 1.1 (0.9, 1.3) | 1.0 (0.8, 1.3) |
| Sinusitis History | 3.6 (3.0, 4.4) | 2.3 (1.9, 2.9) |
| Headache History | 4.9 (4.0, 5.9) | 3.2 (2.5, 4.0) |
| Chronic Disease History | 2.3 (1.9, 2.8) | 1.3 (1.1, 1.6) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cone, J.E.; Stein, C.R.; Lee, D.J.; Flamme, G.A.; Brite, J. Persistent Hearing Loss among World Trade Center Health Registry Residents, Passersby and Area Workers, 2006–2007. Int. J. Environ. Res. Public Health 2019, 16, 3864. https://doi.org/10.3390/ijerph16203864
Cone JE, Stein CR, Lee DJ, Flamme GA, Brite J. Persistent Hearing Loss among World Trade Center Health Registry Residents, Passersby and Area Workers, 2006–2007. International Journal of Environmental Research and Public Health. 2019; 16(20):3864. https://doi.org/10.3390/ijerph16203864
Chicago/Turabian StyleCone, James E., Cheryl R. Stein, David J. Lee, Gregory A. Flamme, and Jennifer Brite. 2019. "Persistent Hearing Loss among World Trade Center Health Registry Residents, Passersby and Area Workers, 2006–2007" International Journal of Environmental Research and Public Health 16, no. 20: 3864. https://doi.org/10.3390/ijerph16203864
APA StyleCone, J. E., Stein, C. R., Lee, D. J., Flamme, G. A., & Brite, J. (2019). Persistent Hearing Loss among World Trade Center Health Registry Residents, Passersby and Area Workers, 2006–2007. International Journal of Environmental Research and Public Health, 16(20), 3864. https://doi.org/10.3390/ijerph16203864