A Profile of Injuries Sustained by Firefighters: A Critical Review





Abstract
1. Introduction
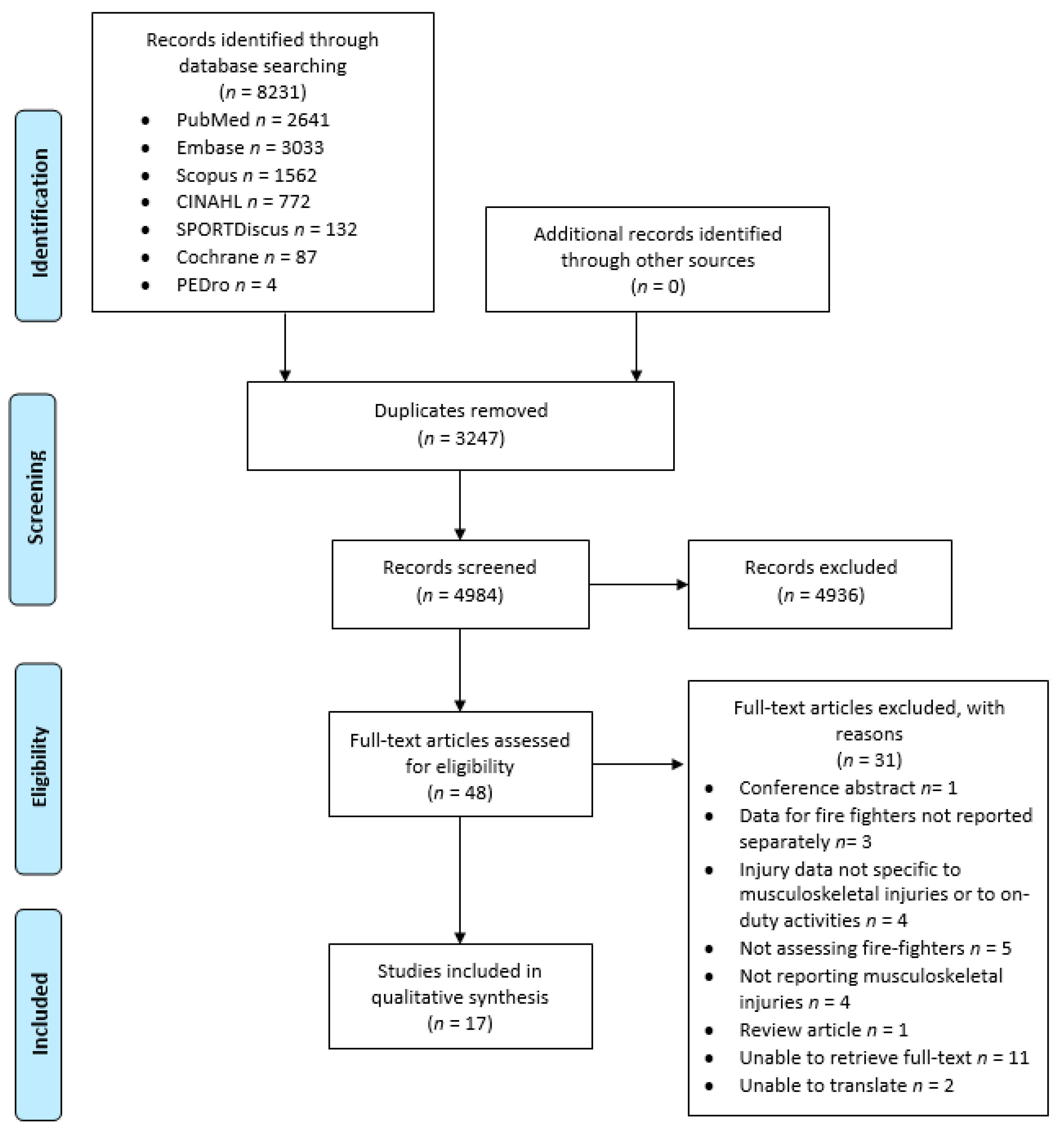
2. Methods
3. Results
4. Discussion
4.1. Musculoskeletal Injury Incidence in Firefighter Populaitons
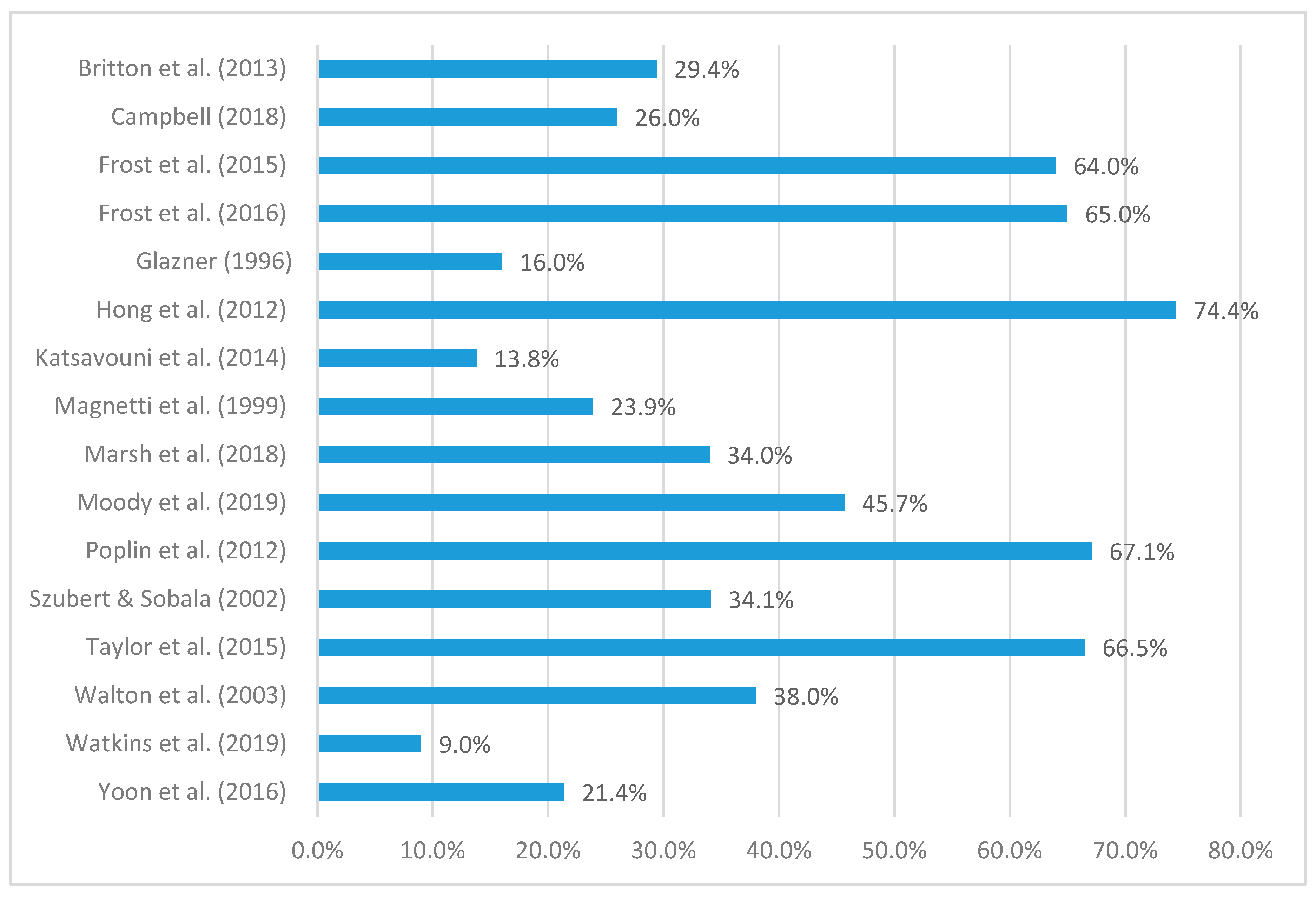
4.2. Commonly Injured Body Site
4.3. Common Nature of Injury
4.4. Common Mechanisms of Injury
4.5. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Seabury, S.A.; McLaren, C.F. The Frequency, Severity, and Economic Consequences of Musculoskeletal Injuries to Firefighters in California. Rand Health Q. 2012, 2, 81572548. [Google Scholar]
- Walker, A.; Pope, R.; Schram, B.; Gorey, R.; Orr, R. The Impact of Occupational Tasks on Firefighter Hydration During a Live Structural Fire. Safety 2019, 5, 36. [Google Scholar] [CrossRef]
- Vu, V.; Walker, A.; Ball, N.; Spratford, W. Ankle restrictive firefighting boots alter the lumbar biomechanics during landing tasks. Appl. Ergon. 2017, 65, 123–129. [Google Scholar] [CrossRef]
- Park, H.; Kakar, R.S.; Pei, J.; Tome, J.M.; Stull, J. Impact of Size of Fire boot and SCBA Cylinder on Firefighters’ Mobility. Cloth. Text. Res. J. 2019, 37, 103–118. [Google Scholar] [CrossRef]
- Frost, D.M.; Beach, T.A.; Crosby, I.; McGill, S.M. The cost and distribution of firefighter injuries in a large Canadian Fire Department. Work 2016, 55, 497–504. [Google Scholar] [CrossRef]
- Lyons, K.; Radburn, C.; Orr, R.; Pope, R. A profile of injuries sustained by law enforcement officers: A critical review. Int. J. Environ. Res. Public Health 2017, 14, 142. [Google Scholar] [CrossRef]
- MacDonald, D.; Pope, R.; Orr, R.M. A Comparison of Work Health and Safety Incidents and Injuries in Part-time and Full-time Australian Army Personnel. J. Athl. Train. 2016, 51, 880–886. [Google Scholar] [CrossRef]
- Baran, K.; Dulla, J.; Orr, R.M.; Dawes, J.; Pope, R.R. Duty Loads carried by LA Sheriff’s Department Deputies. J. Aust. Strength Cond. 2018, 26, 34–38. [Google Scholar]
- Carlton, S.D.; Carbone, P.D.; Stierli, M.; Orr, R.M. The impact of occupational load carriage on the mobility of the tactical police officer. J. Aust. Strength Cond. 2014, 21, 32–37. [Google Scholar]
- Orr, R.M.; Pope, R.; Coyle, J.; Johnston, V. Occupational loads carried by Australian soldiers on military operations. J. Health Saf. Environ. 2015, 31, 451–467. [Google Scholar]
- Task Force Devil Combined Arms Assessment Team: The Modern Warrior’s Combat. Available online: http://thedonovan.com/archives/modernwarriorload/ModernWarriorsCombatLoadReport.pdf (accessed on 27 March 2019).
- Orr, R.M.; Pope, R.; Johnston, V.; Coyle, J. Soldier occupational load carriage: A narrative review of associated injuries. Int. J. Inj. Control Saf. Promot. 2014, 21, 388–396. [Google Scholar] [CrossRef]
- Taylor, N.A.; Lewis, M.C.; Notley, S.R.; Peoples, G.E. A fractionation of the physiological burden of the personal protective equipment worn by firefighters. Eur. J. Appl. Physiol. 2012, 112, 2913–2921. [Google Scholar] [CrossRef]
- Walton, S.M.; Conrad, K.M.; Furner, S.E.; Samo, D.G. Cause, type, and workers’ compensation costs of injury to fire fighters. Am. J. Ind. Med. 2003, 43, 454–458. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Frost, D.M.; Beach, T.A.; Crosby, I.; McGill, S.M. Firefighter injuries are not just a fireground problem. Work 2015, 52, 835–842. [Google Scholar] [CrossRef]
- Marsh, S.M.; Gwilliam, M.; Konda, S.; Tiesman, H.M.; Fahy, R. Nonfatal Injuries to Firefighters Treated in U.S. Emergency Departments, 2003–2014. Am. J. Prev. Med. 2018, 55, 353–356. [Google Scholar] [CrossRef]
- Poplin, G.S.; Harris, R.B.; Pollack, K.M.; Peate, W.F.; Burgess, J.L. Beyond the fireground: Injuries in the fire service. Inj. Prev. 2012, 18, 228–233. [Google Scholar] [CrossRef]
- Yoon, J.H.; Kim, Y.K.; Kim, K.S.; Ahn, Y.S. Characteristics of Workplace Injuries among Nineteen Thousand Korean Firefighters. J. Korean Med Sci. 2016, 31, 1546–1552. [Google Scholar] [CrossRef]
- Taylor, N.A.S.; Dodd, M.J.; Taylor, E.A.; Donohoe, A.M. A Retrospective Evaluation of Injuries to Australian Urban Firefighters (2003 to 2012): Injury Types, Locations, and Causal Mechanisms. J. Occup. Environ. Med. 2015, 57, 757–764. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Eng, J.J.; Teasell, R.; Miller, W.C.; Wolfe, D.L.; Townson, A.F.; Aubut, J.A.; Abramson, C.; Hsieh, J.T.; Connolly, S.; Konnyu, K.; et al. Spinal Cord Injury Rehabilitation Evidence: Method of the SCIRE Systematic Review. Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.; Pope, R.; Orr, R.M. The impact of fire suppression tasks on firefighter hydration: A critical review with consideration of the utility of reported hydration measures. Ann. Occup. Environ. Med. 2016, 28, 63. [Google Scholar] [CrossRef] [PubMed]
- Cocke, C.; Orr, R. The impact of physical training programs on the fitness of tactical populations: A critical review. J. Strength Cond. 2015, 23, 39–52. [Google Scholar]
- Kennelly, J. Methodological Approach to Assessing the Evidence. In Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes; Springer: Berlin/Heidelberg, Germany, 2011; pp. 7–19. [Google Scholar]
- National Health and Medical Research Centre (NHMRC). NHMRC Additional Levels of Evidence and Grades for Recommendations for Developers of Guidelines; Australian Government NHMRC: Canberra, Australia, 2009. Available online: https://www.nhmrc.gov.au/_files_nhmrc/file/guidelines/developers/nhmrc_levels_grades_evidence_120423.pdf (accessed on 05 August 2019).
- Moody, V.J.; Purchio, T.J.; Palmer, C.G. Descriptive analysis of injuries and illnesses self-reported by wildland firefighters. Int. J. Wildland Fire 2019, 28, 412–419. [Google Scholar] [CrossRef]
- Britton, C.; Lynch, C.F.; Ramirez, M.; Torner, J.; Buresh, C.; Peek-Asa, C. Epidemiology of injuries to wildland firefighters. Am. J. Emerg. Med. 2013, 31, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Glazner, L.K. Factors related to injury of shiftworking fire fighters in the Northeastern United States. Saf. Sci. 1996, 21, 255–263. [Google Scholar] [CrossRef]
- Hong, O.; Chin, D.L.; Phelps, S.; Feld, J.; Vogel, S. Occupational injuries, duty status, and factors associated with injuries among firefighters. Workplace Health Saf. 2012, 12, 517–523. [Google Scholar] [CrossRef]
- Katsavouni, F.; Bebetsos, E.; Malliou, P.; Beneka, A. The type and causes of injuries in firefighters. Arch. Hell. Med./Arheia Ellenikes Iatr. 2014, 31, 4. [Google Scholar]
- Szubert, Z.; Sobala, W. Work-related injuries among firefighters: Sites and circumstances of their occurrence. Int. J. Occup. Med. Environ. Health 2002, 15, 49–55. [Google Scholar]
- Watkins, E.R.; Walker, A.; Mol, E.; Jahnke, S.; Richardson, A.J. Women Firefighters’ Health and Well-Being: An International Survey. Women’s Health Issues 2019. [Google Scholar] [CrossRef]
- Magnetti, S.M.; Wyant, W.D.; Greenwood, J.; Roder, N.J.; Linton, J.C.; Ducatman, A.M. Injuries to volunteer fire fighters in West Virginia. J. Occup. Environ. Med. 1999, 41, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.U.S. Firefighter Injuries on the Fireground, 2010–2014. Fire Technol. 2018, 54, 461–477. [Google Scholar] [CrossRef]
- Pope, R.; Orr, R. Incidence rates for work health and safety incidents and injuries in Australian Army reserve vs full time soldiers, and a comparison of reporting systems. J. Mil. Veterans Health 2017, 25, 16. [Google Scholar]
- Pope, R.; MacDonald, D.; Orr, R. Incidence rates of reported work health & safety incidents & injuries in part-time & full-time Australian Army personnel. In Proceedings of the Australasian Military Medicine Association (AMMA) Conference, Hobart, Australia, 9–11 October 2015. [Google Scholar]
- Smith, L.; Westrick, R.; Sauers, S.; Cooper, A.; Scofield, D.; Claro, P.; Warr, B. Underreporting of Musculoskeletal Injuries in the US Army: Findings From an Infantry Brigade Combat Team Survey Study. Sports Health 2016, 8, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, M.; Berkowitz, S.M.; Peck, C.A., Jr. Musculoskeletal-related disability in US Army personnel: Prevalence, gender, and military occupational specialties. J. Occup. Environ. Med. 1997, 39, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Hauret, K.G.; Jones, B.H.; Bullock, S.H.; Canham-Chervak, M.; Canada, S. Musculoskeletal Injuries. Am. J. Prev. Med. 2009, 38, S61–S70. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.H.; Cowan, D.N.; Tomlinson, J.P.; Robinson, J.R.; Polly, D.W.; Frykman, P.N. Epidemiology of injuries associated with physical training among young men in the army. Med. Sci. Sports Exerc. 1993, 25, 197–203. [Google Scholar] [CrossRef]
- Knapik, J.; Ang, P.; Reynolds, K.; Jones, B. Physical fitness, age, and injury incidence in infantry soldiers. J. Occup. Environ. Med. 1993, 35, 598–603. [Google Scholar] [CrossRef]
- Rauh, M.J.; Macera, C.A.; Trone, D.W.; Shaffer, R.A.; Brodine, S.K. Epidemiology of stress fracture and lower-extremity overuse injury in female recruits. Med. Sci. Sports Exerc. 2006, 38, 1571–1577. [Google Scholar] [CrossRef]
- Brandl, S.G.; Stroshine, M.S. The Physical Hazards of Police Work Revisited. Police Q. 2012, 15, 262–282. [Google Scholar] [CrossRef]
- Larsen, B.; Aisbett, B.; Silk, A. The Injury Profile of an Australian Specialist Policing Unit. Int. J. Environ. Res. Public Health 2016, 13, 370. [Google Scholar] [CrossRef] [PubMed]
- Defence Health Services Branch. ADF Health Status; The Department of Defence, Commonwealth of Australia: Canberra, Australia, 2000.
- Copley, G.B.; Burnham, B.R.; Shim, M.J.; Kemp, P.A. Using safety data to describe common injury-producing events: Examples from the US Air Force. Am. J. Prev. Med. 2010, 38, S117–S125. [Google Scholar] [CrossRef] [PubMed]
- Le, T.D.; Gurney, J.M.; Nnamani, N.S.; Gross, K.R.; Chung, K.K.; Stockinger, Z.T.; Nessen, S.C.; Pusateri, A.E.; Akers, K.S. A 12-year analysis of nonbattle injury among US service members deployed to Iraq and Afghanistan. JAMA Surg. 2018, 153, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E. Systematic reviews: CRD’s guidance for undertaking reviews in health care. Lancet Infect. Dis. 2010, 10, 226. [Google Scholar] [CrossRef]
- Thiese, M.S. Observational and interventional study design types; an overview. Biochem. Med. 2014, 24, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Schram, B.; Orr, R.; Pope, R. A Profile of Knee Injuries Suffered by Australian Army Reserve Soldiers. Int. J. Environ. Res. Public Health 2019, 16, 12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Database | Search Terms |
|---|---|
| PUBMED | (firefighter OR firefighters OR “fire fighter” OR “fire fighters” OR “Firefighters” [Mesh] OR “first responder” OR “first responders” OR “emergency responder” OR “emergency responders” OR “Emergency Responders” [Mesh] OR “fire and rescue” OR “smoke jumpers” OR fireman OR firemen) AND (injury OR injuries OR “Wounds and Injuries” [Mesh]) |
| CINAHL | (firefighter OR firefighters OR “fire fighter” OR “fire fighters” OR (MM “Firefighters+”) OR “first responder” OR “first responders” OR “emergency responder” OR “emergency responders” OR “fire and rescue” OR “smoke jumpers” OR fireman OR firemen) AND (injury OR injuries OR (MM “Wounds and Injuries+”)) |
| EMBASE | (‘firefighter’/exp OR firefighter OR firefighters OR ‘fire fighter’/exp OR ‘fire fighter’ OR ‘fire fighters’/exp OR ‘fire fighters’ OR ‘firefighters’/exp OR ‘firefighters’ OR ‘first responder’ OR ‘first responders’ OR ‘emergency responder’/exp OR ‘emergency responder’ OR ‘emergency responders’/exp OR ‘emergency responders’ OR ‘fire and rescue’ OR ‘smoke jumpers’ OR ‘fireman’/exp OR fireman OR firemen) AND (‘injury’/exp OR injury OR ‘injuries’/exp OR injuries OR ‘wounds and injuries’/exp) |
| COCHRANE | (firefighter OR firefighters OR “fire fighter” OR “fire fighters” OR [mh Firefighters] OR “first responder” OR “first responders” OR “emergency responder” OR “emergency responders” OR [mh “Emergency Responders”] OR “fire and rescue” OR “smoke jumpers” OR fireman OR firemen) AND (injury OR injuries OR [mh “Wounds and Injuries”]) |
| SCOPUS | ( TITLE-ABS-KEY(“firefighter”) OR TITLE-ABS-KEY(“firefighters”) OR TITLE-ABS-KEY(“fire fighter”) OR TITLE-ABS-KEY(“fire fighters”) OR INDEXTERMS(“Firefighters”) OR TITLE-ABS-KEY(“first responder”) OR TITLE-ABS-KEY(“first responders”) OR TITLE-ABS-KEY(“emergency responder”) OR TITLE-ABS-KEY(“emergency responders”) OR INDEXTERMS(“Emergency Responders”) OR TITLE-ABS-KEY(“fire and rescue”) OR TITLE-ABS-KEY(“smoke jumpers”) OR TITLE-ABS-KEY(“fireman”) OR TITLE-ABS-KEY(“firemen”) ) AND ( TITLE-ABS-KEY(“injury”) OR TITLE-ABS-KEY(“injuries”) OR INDEXTERMS(“Wounds and Injuries”) ) |
| SPORTDISCUS | (firefighter OR firefighters OR “fire fighter” OR “fire fighters” OR “first responder” OR “first responders” OR “emergency responder” OR “emergency responders” OR OR “fire and rescue” OR “smoke jumpers” OR fireman OR firemen) AND (injury OR injuries OR DE “WOUNDS & injuries”) |
| PEDRO | “firefighter*” AND “injur*” |
| Inclusion Criteria | Example/s |
| Study was focused on firefighters | Studies involving wildland firefighters, urban firefighters, career firefighters, volunteer firefighters, fire service personnel |
| Study examined musculoskeletal injuries occurring to, or in, a firefighter population while on duty | Studies examining musculoskeletal injuries, musculoskeletal disability, injury epidemiology, injury rates, injury incidence |
| Exclusion Criteria | Example/s |
| Study involved participants who were not firefighters | Studies involving emergency medical responders, first responders, or other population, without data specific for firefighters |
| Study included only injuries that were not musculoskeletal injuries while on duty | Studies which only examined occupational injuries without data for musculoskeletal injuries, or studies which examined, recreational injuries, sporting injuries, fatalities, chemical hazards, mortality, homicide, suicide, mental illness |
| Review article, or study reported as an abstract only |
| Database | Identified Studies (n) |
|---|---|
| PUBMED | 2641 |
| CINAHL | 772 |
| EMBASE | 3033 |
| COCHRANE | 87 |
| SCOPUS | 1562 |
| SPORTDISCUS | 132 |
| PEDRO | 4 |
| Authors (Year) and [Reference] | Title | Aim/Objective/Hypothesis | Study Design | Data Collection Method | Downs and Black Score | Level of Evidence * |
|---|---|---|---|---|---|---|
| Britton et al. (2013) [28] | Epidemiology of injuries to wildland firefighters | Examine nonfatal wildland firefighter injuries reported to the US Department of Interior (DOI) from 2003 to 2007. | Retrospective Cohort | Database | 70% | III-2 |
| Campbell (2018) [35] | US Firefighter Injuries on the Fireground, 2010–2014 | Profile US firefighter injuries occurring on the fireground from 2010 to 2014. | Retrospective Cohort | Database | 45% | III-2 |
| Frost et al. (2015) [16] | Firefighter injuries are not just a fireground problem | Characterise the injuries sustained by members of a large Canadian metropolitan fire department over a 5-year span (2007–2011) | Retrospective Cohort | Database | 50% | III-2 |
| Frost et al. (2016) [5] | The cost and distribution on firefighter injuries in a large Canadian Fire Department | Categorise the cost of injuries filed in 2012 by firefighters from a large department by job duty, injury type, body part affected, and the general motion pattern employed at the time of injury. | Retrospective Cohort | Database | 60% | III-2 |
| Glazner (1996) [29] | Factors related to injury of shiftwork fire fighters in the Northeastern United States | Identify factors involved in injuries sustained by fire fighters in three different municipal fire departments. | Retrospective Cohort | Database | 60% | III-2 |
| Hong et al. (2012) [30] | Occupational Injuries, Duty Status, and Factors Associated With Injuries Among Firefighters | Assess the type of occupational injuries, duty status, and factors associated with injuries among firefighters. | Cross-sectional | Self-report/Internet-based survey | 60% | IV |
| Katsavouni et al. (2014) [31] | The type and causes of injuries in firefighters | Investigate the nature and causes of occupational injuries in firefighters. | Cross-sectional | Self-report | 55% | IV |
| Magnetti et al. (1999) [34] | Injuries to Volunteer Fire Fighters in West Virginia | Describe the distribution of occupational injuries to volunteer fire fighters (VFFs) by demographic characteristics, presenting history, time, and geographic location, using the West Virginia State Worker’s Compensation database. | Retrospective Cohort | Database | 50% | III-2 |
| Marsh et al. (2018) [17] | Nonfatal Injuries to Firefighters Treated in U.S. Emergency Departments, 2003–2014 | Enhance current knowledge by providing national estimates of nonfatal injuries to firefighters treated in US emergency departments | Retrospective Cohort | Database | 55% | III-2 |
| Moody et al. (2019) [27] | Descriptive analysis of injuries and illnesses self-reported by wildland firefighters | Understand types of injuries and illnesses wildland firefighters (WLFFs) sustain during the fire season. | Cross-sectional | Web-based self-reported questionnaire | 75% | IV |
| Poplin et al. (2012) [18] | Beyond the fireground: injuries in the fire service | Explore injuries not only on the fireground but also during other fire service activities. | Retrospective Cohort | Database | 55% | III-2 |
| Seabury and McLaren (2012) [1] | The Frequency, Severity, and Economic Consequences of Musculoskeletal Injuries to Firefighters in California | # Describe the average frequency and severity of work-related musculoskeletal disorders (MSDs) experienced by firefighters in California. # Study the impact of work-related MSDs on the earnings and employment of firefighters several years after injury. # Evaluate the impact of reforms to the disability rating system on the ratings of firefighters with permanently disabling MSDs. # Assess whether reforms to the medical delivery system affected the employment outcomes of firefighters with MSDs. | Retrospective Cohort | Database | 20% | III-2 |
| Szubert and Sobala (2002) [32] | Work-related injuries among firefighters: sites and circumstances | Determine the injury ratio, causes and duration of temporal work disability from on-duty injuries among firefighters, taking into account the site and circumstances of their occurrence. | Retrospective Cohort | Database | 55% | III-2 |
| Taylor et al. (2015) [20] | A Retrospective Evaluation of Injuries to Australian Urban Firefighters (2003 to 2012): Injury Types, Locations, and Causal Mechanisms | Evaluate injury trends within Australian firefighters. | Retrospective Cohort | Database | 50% | III-2 |
| Walton et al. (2003) [14] | Cause, Type, and Workers’ Compensation Costs of Injury to Fire Fighters | A better understanding of the costs of injury to firefighters, and how those costs relate to the cause and the nature of those injuries can help inform policy decisions regarding the occupational health of firefighters (Musich et.al., 2001). Such information can serve to document financial incentives to infuse dollars into firefighter injury prevention and suggest priority areas for further study. | Retrospective Cohort | Database | 55% | III-2 |
| Watkins et al. (2019) [33] | Women Firefighters’ Health and Well-Being: An International Survey | Identify specific health and well-being issues that women firefighters may experience as part of their daily working practices. Issues identified from this under-represented population can drive future research, education, and strategy to guide safety and health practices. | Cross-sectiona | Self-report | 60% | IV |
| Yoon et al. (2016) [19] | Characteristics of Workplace Injuries among Nineteen Thousand Korean Firefighters | Provide as comprehensive an evaluation as possible to aid in improving safety strategies for firefighters, as well as to improve their health and well-being. | Cross-sectional | Self-report | 85% | IV |
| Authors [Reference] | Year | Title | Injury Definition | Participant Details | Main Findings |
|---|---|---|---|---|---|
| Britton et al. [28] | 2013 | Epidemiology of injuries to wildland firefighters | No Injury definition | # Over 200,000 wildland firefighters (USA) in the 5-year period from 2003 to 2007 # Age at injury = 17 to 65 years # Total occupational injuries = 1301 | # Slips/trips/falls were the mechanism for almost half of all sprains and strains (49%) and fractures and dislocations (43%). # Of all injuries: - Fractures/dislocations = 51 (3.9%). - Sprains/strains = 382 (29.4%, most common type). # Almost two-thirds of all injuries (65%) occurred during the peak season. # For all injuries, the lower extremity was the most common body part involved (35%). # Back injuries represented slightly less than 10% of all injuries reported but comprised 21% of all injuries caused by equipment/tools/machinery. # Of the 121 back injuries reported, 29 (16%) were considered severe (data not shown). |
| Campbell [35] | 2018 | US Firefighter Injuries on the Fireground, 2010-2014 | No Injury definition | # 1,121,630 Firefighters from USA (2010–2014) - Carrer = 345,180 - Volunteers = 776,450 - Career males = 334,050 - Career females = 20,590 - Volunteer males = 717,800 - Volunteer females = 70,450 # Total 30,290 injuries/year | # Leading cause of injuries = overexertion or strain (26%) # Strain or sprain was the leading primary symptom (28%) |
| Frost et al. [16] | 2015 | Firefighter injuries are not just a fireground problem | A reportable injury was defined in accordance with the Occupational Health and Safety regulations for Alberta, namely medical treatment, restricted work duties or lost time. | # Calgary Fire Department (western Canada) #1311 injuries (2007–2011) # In 2011:- 1363 personnel - 37 stations - Age = 38 (SD 9) years - Height = 1.80 (SD 0.06) m - Body mass = 89 (SD 11) kg - 2% were women - 100,695 responses to 50,520 incidences - 204 injuries | # Musculoskeletal disorders (MSD) = 845 (64% of all injuries, 2007-2011): - Ankle = 9.5% - Back = 20.1% - Knee = 10.6% - Shoulder = 8% - Other (neck, hip, elbow, wrist, hand, foot, abdomen, chest, arm, leg, and groin) = 15.3% # Job site/occupation: - Fire station = 37.9% - Physical training = 26.6% # Mechanism: - Bending/Lifting/Squatting = 23.2% - Slipping/Tripping/Falling = 21.3% |
| Frost et al. [5] | 2016 | The cost and distribution on firefighter injuries in a large Canadian Fire Department | A reportable injury was defined in accordance with the Occupational Health and Safety regulations for Alberta, namely medical treatment, restricted work duties or lost time, which was defined as missing one or more shifts because of an occurrence. | # Calgary Fire Department (western Canada) # 1289 personnel# 38 stations # 102,632 responses to 52,918 incidences # 244 injuries | # Musculoskeletal disorders (MSD) = 159 (65% of all injuries): - Ankle = 10.7% - Back = 32.1% - Knee = 22.6% - Shoulder = 14.5% - Other (neck, hip, elbow, wrist, hand, foot, abdomen, chest, arm, leg, and groin) = 20.1 # Job site/occupation: - Fire station = 31% - Physical training = 28%# Mechanism: - Bending/Lifting/Squatting = 23% - Slipping/Tripping/Falling = 18% # MSD = 77% of medical and compesation costs: - 28% = knee - 18% = back |
| Glazner [29] | 1996 | Factors related to injury of shiftwork fire fighters in the Northeastern United States | No Injury definition | # 447 career fire fighters of 3 fire departments (USA) # 171 injuries | # Sprains, strains, or pain = 16% # Back, neck, or knee injuries = 4% # Fractures = 4% |
| Hong et al. [30] | 2012 | Occupational Injuries, Duty Status, and Factors Associated With Injuries Among Firefighters | No Injury definition | # 437 fire fighters from 34 fire departments (USA), from 2010 to 2011 # 92.4% male # 80% Caucasian # Mean age = 44.9 (SD 8.1) years # Years worked in fire services = 17.4 (SD 8.2) years # Occupational accidents/injuries n = 285 | # Muscle strains/sprains = 212 (74.4%) # Back injury = 153 # Broken bones = 35 |
| Katsavouni et al. [31] | 2014 | The type and causes of injuries in firefighters | No Injury definition | # 3289 full-time firefighters (Greece) # Age = 24 to 60 years (mean 36.4, SD 6.19) # 96.3% males # 502 individuals reported injury at work | # Lumbar injuries = 107 # Muscle strains = 69 (13.8%) # Foot injuries = 41 # Knee injuries = 41 # Leg injuries = 28 # Shoulder injuries = 19 # Chest-rib injuries = 14 # Neck injuries = 11 # Main mechanism = slip/trip/fall |
| Magnetti et al. [34] | 1999 | Injuries to Volunteer Fire Fighters in West Virginia | No Injury definition | # Volunteer fire fighters (VFFs) of West Virginia (USA) # Age = 27.6 (SD 9.96) years # 343 workers’ compensation claims for occupational injuries for the fiscal year 1992 # Injury rate = 36.07 per 1000 responses | # Lacerations and contusions = 28.9% # Strains and sprains = 23.9% |
| Marsh et al. [17] | 2018 | Nonfatal Injuries to Firefighters Treated in U.S. Emergency Departments, 2003-2014 | The term “injury” was used to refer to injuries, illnesses, and exposures | # USA # 95% male # 35% aged between 30-39 years # 351,800 injuries (2003–2014) | # Sprain/Strain = 34% # Fracture/dislocation = 5% # Training and patient care activities both most often resulted in sprains and strains |
| Moody et al. [27] | 2019 | Descriptive analysis of injuries and illnesses self-reported by wildland firefighters | No Injury definition | # 284 wildland firefighters (WLFFs) (USA) # Of 254 WLFFs who reported at least one injury: - 87.4% Male - 38.1% aged 35–44 years # 453 injuries and illnesses (over 5 years) | # Joint sprain = 25.4% # Muscle strain = 15.2% # Fracture/dislocation = 7.1% # Tendinitis = 5.1% # Muscle cramp, spasm = 1.8% |
| Poplin et al. [18] | 2007 | Beyond the fireground: injuries in the fire service | A reportable injury is defined in accordance with Occupational Safety and Health Administration (OSHA) regulations (29 CFR, 1904.7) (i.e., medical treatment, restricted work time, or lost work time), in addition to any injury that occurred to specific body regions. The surveillance database includes internally documented injuries (i.e., those deemed non-OSHA reportable, but recorded in the Tucson Fire Department system), which had no immediate loss of job function or capabilities, but are documented in the event the injury later progresses to a point requiring a report and or treatment (e.g., due to cumulative or repeated trauma) | # Approximately 650 fire service personnel (USA), including firefighters, paramedics, engineers, inspectors, battalion chiefs # Average of 41 years of age # 5% were women # 76.4% non-Hispanic white # 902 injuries in 409 individuals (2004–2009) # Annual incidence rates ranging between 13.6 and 21.5 injuries per 200,000 h (equivalent to 100 full-time employees) # Mean age of those injured = 37.9 years (20–64 y) | # Sprain, strain = 605 (67.1%) - 44.6% = lower extremity- 32.2% = back/spine - 65.3% = no lost time - 100% = minor - 25.6 % = firefighters - 22.2% = paramedics - 41.8% during physical exercise # Fireground operations = 92 injuries - 40.2% = sprain/strain - 2.2% = fracture/dislocation |
| Seabury and McLaren [1] | 2012 | The Frequency, Severity, and Economic Consequences of Musculoskeletal Injuries to Firefighters in California | No Injury definition | # Firefighters from California | # Firefighters are 3.5 times more likely to suffer a workplace injury and 3.8 times more likely to suffer a work-related MSD than a private-sector worker. # Firefighters take 1.4 times longer to return to work than workers in the private sector for all injuries; this difference skyrockets for MSDs, as firefighters take twice as long to return to work. # The median number of days away from work after an MSD is 1.8 times greater for an MSD than for any other injury for firefighters, whereas this ratio is only 1.25 for private-sector workers. # Both the frequency and the severity of injuries, particularly MSDs, are worse for older firefighters than for younger firefighters. # Older firefighters are 10.4 times more likely to suffer an MSD than are private-sector workers, and they take more than four times longer to return to work. |
| Szubert and Sobala [32] | 2002 | Work-related injuries among firefighters: sites and circumstances | No Injury definition | # 1503 firefighters from 29 fire stations in Poland # In 1994: - Mean age = 32 (SD 6.5) years # 352 injuries (1994–1997) | # 25% were on-duty: - 10.2% = Fractures - 6.8% = Fractures of lower limb - 34.1% = Dislocation, sprains, and strains |
| Taylor et al. [20] | 2015 | A Retrospective Evaluation of Injuries to Australian Urban Firefighters (2003 to 2012): Injury Types, Locations, and Causal Mechanisms | Work-related injuries were defined as physical and psychological (mental health) conditions that arose during, or as a consequence of, employment as a firefighter. | # 6998 Australian firefighters # In 2012: - 95.9% males # 1,225,218 callouts, 6997 injuries (2003 to 2012) | # Joint and muscle sprains and strains = 66.5%: - 177 cases per annum per 1000 full-time firefighters (FTE) |
| Walton et al. [14] | 2003 | Cause, Type, and Workers’ Compensation Costs of Injury to Fire Fighters | Injury was defined as any mild physical harm (e.g., bruises), or any major physical harm involving outpatient or inpatient treatment | # 13,680 firefighters (USA) # Average age = 35 years # 96% male # 1343 injuries (1992 to 1999) | # Strains and sprains account for 38% of the injuries claimed by firefighters # 83% of injuries with a cause of overexertion have a nature of injury of strain or sprain # Mean costs related to strain/sprain: - Medical = $3023 - Total = $8031 |
| Watkins et al. [33] | 2019 | Women Firefighters’ Health and Well-Being: An International Survey | No injury definition | # 840 women firefighters from 14 countries (UK, Ireland, North America, Australasia, mainland Europe) # Age = 40 years (SD 9) # Time as firefighter = 13 years (SD 8) | # Musculoskeletal injuries, including work-related upper and lower limb and back injuries, were reported by 9–23% of women firefighters. |
| Yoon et al. [19] | 2016 | Characteristics of Workplace Injuries among Nineteen Thousand Korean Firefighters | The occurrence of workplace injuries was defined when the injuries required hospital care: if the injuries did not require hospital care, they were not counted. These criteria were applied to all types of injuries and events including car accidents. | # 19,119 Korean firefighters # Age 20 to 59 years # 2230 injured firefighters | # Most prevalent = wound, cut, bleeding, bruise (n = 1728; 42.3% of all injuries) # Fracture n = 368 (9% of all injuries) # Strain, sprain, muscular pain n = 876 (21.4% of all injuries) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orr, R.; Simas, V.; Canetti, E.; Schram, B. A Profile of Injuries Sustained by Firefighters: A Critical Review. Int. J. Environ. Res. Public Health 2019, 16, 3931. https://doi.org/10.3390/ijerph16203931
Orr R, Simas V, Canetti E, Schram B. A Profile of Injuries Sustained by Firefighters: A Critical Review. International Journal of Environmental Research and Public Health. 2019; 16(20):3931. https://doi.org/10.3390/ijerph16203931
Chicago/Turabian StyleOrr, Robin, Vinicius Simas, Elisa Canetti, and Ben Schram. 2019. "A Profile of Injuries Sustained by Firefighters: A Critical Review" International Journal of Environmental Research and Public Health 16, no. 20: 3931. https://doi.org/10.3390/ijerph16203931
APA StyleOrr, R., Simas, V., Canetti, E., & Schram, B. (2019). A Profile of Injuries Sustained by Firefighters: A Critical Review. International Journal of Environmental Research and Public Health, 16(20), 3931. https://doi.org/10.3390/ijerph16203931