The Effectiveness of Cigarette Pack Health Warning Labels with Religious Messages in an Urban Setting in Indonesia: A Cross-Sectional Study

 ,
, 

Abstract
1. Introduction
2. Methods
2.1. Sample and Recruitment
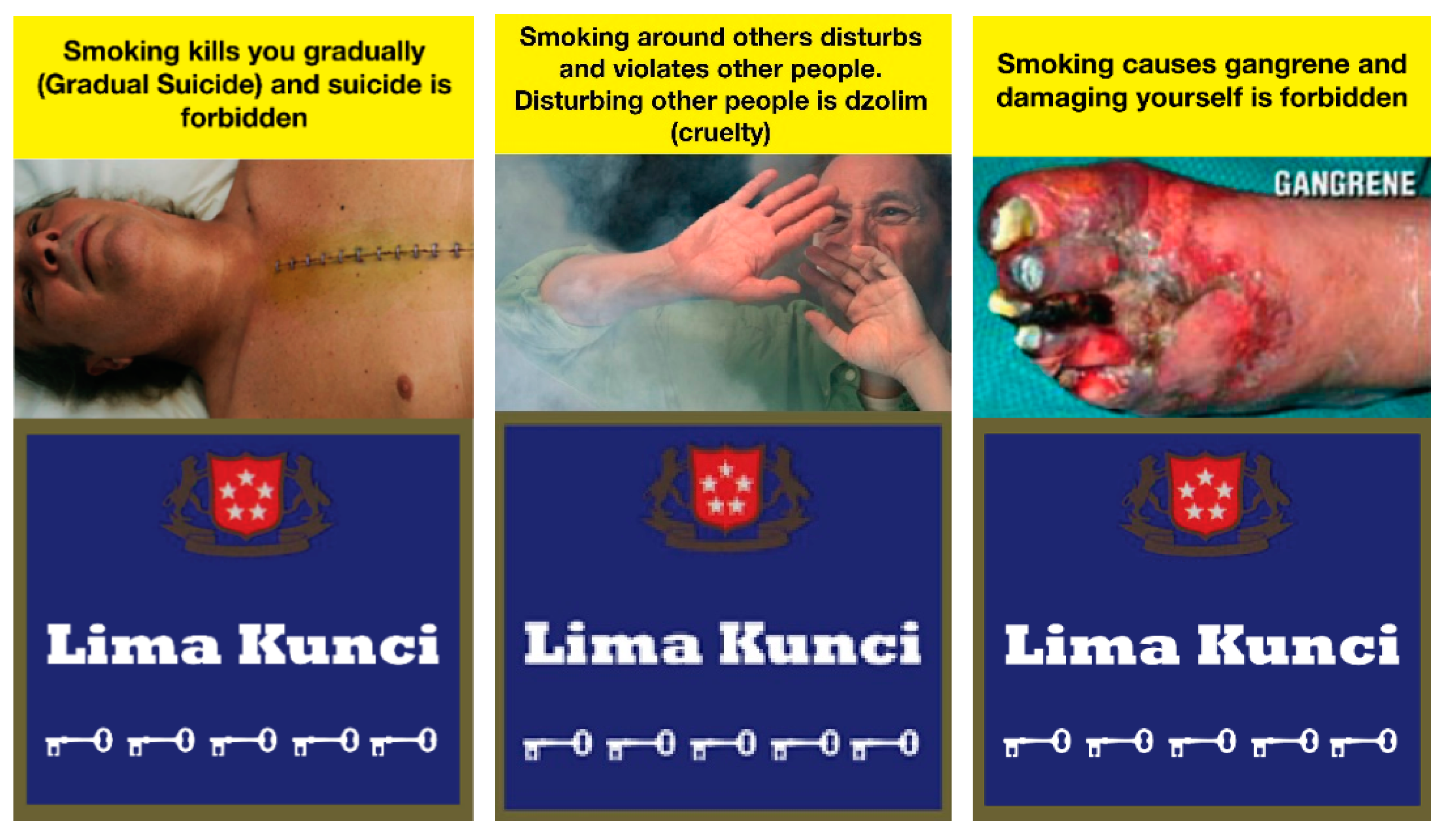
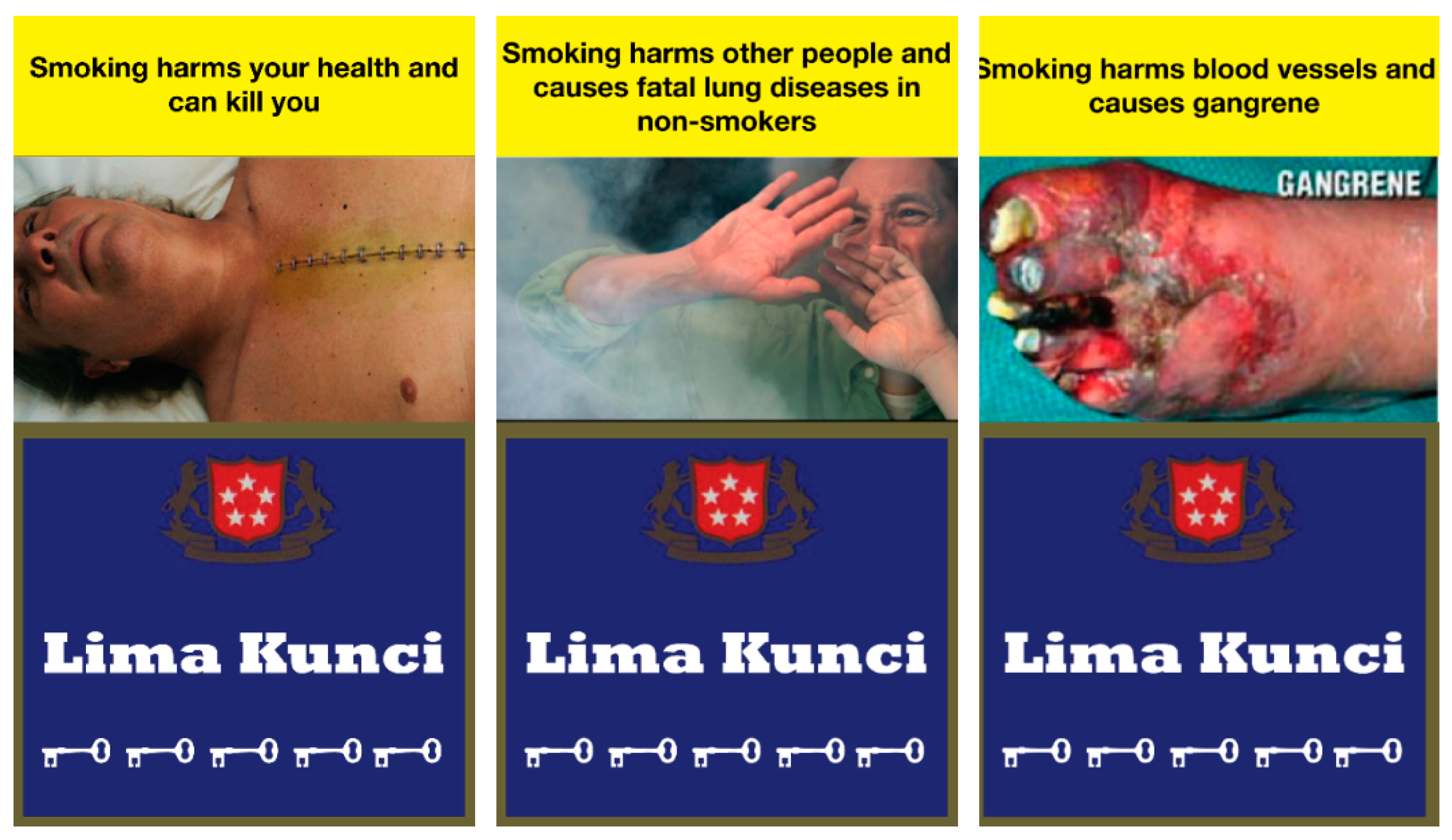
2.2. Health Warning Label Design
2.3. Rating the Effectiveness of HWLs
2.4. Religiosity Level
2.5. Smoking Behavior and Intentions
2.6. Statistical Analysis
2.7. Ethics Approval
3. Results
3.1. Sociodemographic Characteristics of Participants by Religiosity Level
3.2. Rating Scores of Religious and Nonreligious HWLs
3.3. The Association between CRS Score and HWL Rating Scores
4. Discussion
5. Conclusions
Author Contributors
Funding
Conflicts of Interest
References
- Global Adult Tobacco Survey: Indonesia Report 2011. World Health Organization Regional Office for Southeast Asia: New Delhi, India, 2012; Available online: http://www.searo.who.int/tobacco/data/gats_indonesia_2011.pdf (accessed on 22 March 2017).
- Campaign for Tobacco-Free Kids, Indonesia Tobacco Control Policy Status Fact Sheet. c2016. Available online: http://www.tobaccocontrollaws.org/legislation/factsheet/policy_status/indonesia (accessed on 19 January 2017).
- Hellendorf, B.; Schmitz, M.; Group for Research and Information on Peace and Security. Indonesia, From Regional to Global Power? Available online: http://www.grip.org/sites/grip.org/files/NOTES_ANALYSE/2014/na_2014-05-07_en_b-hellendorff.pdf (accessed on 26 May 2017).
- University of Southern California. Religion, Social Interactions, and Cooperative Attitudes: Evidence from Indonesia. Gaduh, A. (Preliminary draft). Available online: http://pacdev.ucdavis.edu/files/conference-schedule/session/papers/religion_social_interactions_and_cooperative_attitudes.pdf (accessed on 30 May 2017).
- Religion, Power and Politics in Indonesia. Available online: https://www.bbc.com/news/world-asia-39650150 (accessed on 1 January 2019).
- How Religion Shapes Elections in Indonesia. Available online: https://www.economist.com/asia/2018/04/12/how-religion-shapes-elections-in-indonesia (accessed on 1 January 2019).
- New World Encyclopedia. Religion in Indonesia. Available online: http://www.newworldencyclopedia.org/entry/Religion_in_Indonesia (accessed on 26 May 2017).
- Boston University School of Public Health, Dean’s Note: On Religion and Public Health. Available online: https://www.bu.edu/sph/2016/07/24/on-religion-and-public-health/ (accessed on 12 November 2018).
- Idler, E. Religion as a Social Determinant of Public Health. Oxford Scholarship Online: September 2014. Available online: http://www.oxfordscholarship.com/view/10.1093/acprof:oso/9780199362202.001.0001/acprof-9780199362202-chapter-1 (accessed on 12 November 2018).
- Garrusi, B.; Nakhaee, N. Religion and smoking: A review of recent literature. Int. J. Psychiatry Med. 2012, 3, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, R.M.; Koenig, H.G. Mental disorders, religion and spirituality 1990 to 2010: A systematic evidence-based review. J. Relig. Health 2013, 2, 657–673. [Google Scholar] [CrossRef] [PubMed]
- Behere, P.B.; Das, A.; Yadav, R.; Behere, A.P. Religion and mental health. Indian J. Psychiatry 2013, 55 (Suppl. 2), 187–194. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.A.; Hill, T.D. Religiosity and adolescent substance use: Evidence from the national survey on drug use and health. Subst. Use Misuse 2012, 7, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Ramahi, I.; Seidenberg, A.B.; Kennedy, R.D.; Rees, V.W. Secondhand smoke emission levels in enclosed public places during Ramadan. Eur. J. Public Health 2013, 23, 789–791. [Google Scholar] [CrossRef] [PubMed]
- El Awa, F. The role of religion in tobacco control interventions. Bull. World Health Organ. 2014, 12, 894. [Google Scholar]
- Byron, M.J.; Cohen, J.E.; Gittelsohn, J.; Frattaroli, S.; Nuryunawati, R.; Jernigan, D.H. Influence of religious organizations’ statements on compliance with a smoke free law in Bogor, Indonesia: A qualitative study. BMJ Open 2015, 12, 1–7. [Google Scholar]
- WHO Islamic Ruling on Smoking. The Right Path to Health, Health Education Through Religion, 2nd ed.; World Health Organization Regional Office for Eastern Mediterranean.: Alexandria, Egypt; Available online: http://apps.who.int/iris/bitstream/handle/10665/119631/dsa46.pdf?sequence=1&isAllowed=y (accessed on 2 December 2016).
- Huber, S.; Huber, O.W. The Centrality of Religiosity Scale (CRS). Religion 2012, 3, 710–724. [Google Scholar] [CrossRef]
- Wardhani, N.; Rintana, D. Studi Validitas ISI CRS-15 (The Centrality of Religiosity Scale—Untuk Suasana Tradisi Keberagamaan Islam di Indonesi). Sosial Ekonomi dan Humaniora 2015, 4, 749–754. [Google Scholar]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Rickert, W.; Robinson, J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br. J. Addict. 1989, 84, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Bowie, J.V.; Parker, L.J.; Beadle-Holder, M.; Ezema, A.; Bruce, M.A.; Thorpe, R.J., Jr. The influence of religious attendance on smoking among Black men. Subst. Use Misuse 2017, 2, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Yong, H.H.; Savvas, S.; Borland, R.; Thrasher, J.; Sirirassamee, B.; Omar, M. Secular versus religious norms against smoking: Which is more important as a driver of quitting behaviour among Muslim Malaysian and Buddhist Thai smokers? Int. J. Behav. Med. 2013, 20, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Tahlil, T.; Woodman, R.J.; Coveney, J.; Ward, P.R. The impact of education programs on smoking prevention: A randomized controlled trial among 11 to 14 years olds in Aceh, Indonesia. BMC Public Health 2013, 4, 367. [Google Scholar] [CrossRef]
- Saeed, A.A.; Khoja, T.A.; Khan, S.B. Smoking behaviour and attitudes among adult Saudi nationals in Riyadh City, Saudi Arabia. Tob. Control 1996, 5, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Yong, H.H.; Fong, G.T.; Driezen, P.; Borland, R.; Quah, A.C.; Sirirassamee, B.; Hamann, S.; Omar, M. Adult Smokers’ Reactions to Pictorial Health Warning Labels on Cigarette Packs in Thailand and Moderating Effects of Type of Cigarette Smoked: Findings from the International Tobacco Control Southeast Asia Survey. Nicotine Tob. Res. 2013, 15, 1339–1347. [Google Scholar] [CrossRef] [PubMed]
- El Awa, F. Middle East: Religion against tobacco. Tob. Control 2003, 12, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Petticrew, M.; Lee, K.; Ali, H. “Fighting a Hurricane”: Tobacco industry efforts to counter the perceived threat of Islam. Am. J. Public Health 2015, 105, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Martin Haley Companies Inc. An Arriving Issue: Smoking and Morality. 14 August 1985. Roswell Park Cancer Institute (RPCI) Collection. Bates no. TI50570718. Available online: http://legacy.library.ucsf.edu/tid/psv28b00 (accessed on 7 January 2019).
- Couple Calls for Tobacco Shut Down after Baby Dies. Available online: https://indonesiaexpat.biz/news/couple-calls-tobacco-shut-baby-dies/ (accessed on 31 January 2019).
- Southeast Asia Tobacco Control Alliance. Baby’s Death Sparks Call for Indonesia to Crack Down on Big Tobacco. Available online: https://seatca.org/babys-death-sparks-call-for-indonesia-to-crack-down-on-big-tobacco/ (accessed on 31 January 2019).
- Hammond, D.; Fong, G.T.; McNeill, A.; Borland, B.; Cummings, K.M. Effectiveness of cigarette warning labels in informing smokers about the risks of smoking: Findings from the International Tobacco Control (ITC) Four Country Survey. Tob. Control 2006, 15 (Suppl. 3), iii9–iii25. [Google Scholar] [CrossRef] [PubMed]
- Bilir, N.; Kaplan, B.; Kucuk-Bicer, B.; Ararat, E.; Akyol, M.; Arslan, A.; Yuksek, H.F. Opinions of a Group of High School Students in Ankara on Pictorial Warnings on Cigarette Packages. Turk. Thorac. J. 2013, 14, 127–133. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gender | n | % |
| Male | 644 | 78.8 |
| Female | 173 | 21.2 |
| Age (Year) | ||
| 18–24 | 421 | 51.5 |
| 25–34 | 236 | 28.9 |
| 35–44 | 103 | 12.6 |
| ≥45 | 50 | 6.1 |
| Education Level | ||
| Primary/Secondary | 76 | 9.3 |
| High School | 510 | 62.7 |
| College | 228 | 28.0 |
| Having Children | ||
| No | 538 | 66.4 |
| Yes | 272 | 33.6 |
| Monthly Income (IDR) | ||
| ≤3 million IDR | 420 | 54.9 |
| >3 million and ≤5 million IDR | 217 | 28.4 |
| >5 million IDR | 128 | 16.7 |
| Smoking Status | ||
| Daily | 642 | 78.6 |
| Occasionally | 46 | 5.6 |
| Not at all | 129 | 15.8 |
| Health Status | ||
| Poor/Fair | 123 | 15.6 |
| Good | 430 | 54.6 |
| Very Good/Excellent | 234 | 29.7 |
| Religiosity Level (n = 665) | ||
| Quite a bit/very much so (4 or 5) | 706 | 86.6 |
| Moderately (3) | 93 | 11.4 |
| Not at all (1 or 2) | 16 | 2.0 |
| Daily Practice | ||
| 5 or more | 497 | 60.8 |
| 1–4 times in a day | 280 | 34.3 |
| Never | 40 | 4.9 |
| Time to First Cigarette (n = 633) | ||
| Within 5 min | 189 | 29.9 |
| 6–30 min | 253 | 40.0 |
| More than 30 min | 191 | 30.2 |
| Quit Attempt in the Past Year (n = 635) | ||
| Yes | 324 | 51.0 |
| No | 311 | 49.0 |
| Plan to Quit (n = 634) | ||
| Within next month | 119 | 18.8 |
| Within next 6 months | 136 | 21.5 |
| Beyond next 6 months | 149 | 23.5 |
| Not at all | 230 | 36.3 |
| Motivation to Quit (n = 635) * | ||
| 1–5 | 287 | 45.2 |
| 6–10 | 348 | 54.8 |
| Motivation to Stay Smoke Free (n = 172) * | ||
| 1–7 | 80 | 46.5 |
| 8–10 | 92 | 53.5 |
| Total | 817 | 100.0 |
| Characteristics | Religiosity Level | p | |||
|---|---|---|---|---|---|
| Score 1–3 | Score 4–5 | ||||
| n | % | n | % | ||
| Gender | |||||
| Male | 84 | 13.0 | 560 | 87.0 | 0.590 |
| Female | 25 | 14.6 | 146 | 85.4 | |
| Age (Year) | |||||
| 18–24 | 65 | 15.5 | 354 | 84.5 | 0.065 |
| ≥25 | 44 | 11.1 | 352 | 88.9 | |
| Education Level | |||||
| Primary/Secondary | 16 | 21.1 | 60 | 78.9 | 0.049 |
| High School | 69 | 13.6 | 440 | 86.4 | |
| College | 23 | 10.1 | 205 | 89.9 | |
| Having Children | |||||
| No | 74 | 13.8 | 462 | 86.2 | 0.606 |
| Yes | 34 | 12.5 | 238 | 87.5 | |
| Monthly Income (IDR) | |||||
| ≤3 million | 67 | 16.0 | 352 | 84.0 | 0.040 |
| >3 million and ≤5 million | 19 | 8.8 | 198 | 91.2 | |
| >5 million | 17 | 13.3 | 111 | 86.7 | |
| Smoking Status | |||||
| Daily | 97 | 15.2 | 543 | 84.8 | 0.004 |
| Occasionally/Not at all | 12 | 6.9 | 163 | 93.1 | |
| Health Status | |||||
| Poor/Fair | 29 | 23.6 | 94 | 76.4 | 0.001 |
| Good | 48 | 11.2 | 380 | 88.8 | |
| Very Good/Excellent | 26 | 11.1 | 208 | 88.9 | |
| Total | 109 | 13.4 | 706 | 86.6 | |
| Rating Questions | n | Nonreligious Death | Religious Death | Nonreligious SHS | Religious SHS | Nonreligious Gangrene | Religious Gangrene | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Med | Mean ± SD | Med | Mean ± SD | Med | Mean ± SD | Med | Mean ± SD | Med | Mean ± SD | Med | ||||
| Grabs My Attention | 810 | 6.9 ± 3.3 | 8.0 | 6.8 ± 3.3 | 8.0 | 7.3 ± 3.0 | 8.0 | 7.2 ± 3.1 | 8.0 | 7.0 ± 3.3 | 8.0 | 7.0 ± 3.2 | 8.0 | ||
| p* | 0.080 | 0.492 | 0.528 | ||||||||||||
| Easy to Understand | 810 | 7.4 ± 3.0 | 8.0 | 7.4 ± 3.0 | 8.0 | 7.8 ± 2.8 | 9.0 | 7.6 ± 2.8 | 9.0 | 7.1 ± 3.1 | 8.0 | 7.1 ± 3.1 | 8.0 | ||
| p* | 0.577 | 0.131 | 0.489 | ||||||||||||
| Credible | 804 | 7.4 ± 3.0 | 9.0 | 7.1 ± 3.1 | 8.0 | 8.0 ± 2.7 | 9.0 | 7.7 ± 2.8 | 9.0 | 7.0 ± 3.1 | 8.0 | 7.0 ± 3.2 | 8.0 | ||
| p* | 0.001 | <0.001 | 0.704 | ||||||||||||
| Makes Me Feel More Concerned about Smoking | 807 | 6.7 ± 3.4 | 8.0 | 6.7 ± 3.3 | 8.0 | 6.8 ± 3.2 | 8.0 | 6.7 ± 3.3 | 8.0 | 6.7 ± 3.3 | 7.0 | 6.8 ± 3.4 | 8.0 | ||
| p* | 0.436 | 0.011 | 0.086 | ||||||||||||
| Makes Me Think about the Health Risks of Smoking | 804 | 6.9 ± 3.3 | 8.0 | 6.8 ± 3.2 | 8.0 | 7.0 ± 3.2 | 8.0 | 6.8 ± 3.2 | 8.0 | 6.9 ± 3.3 | 8.0 | 7.0 ± 3.2 | 8.0 | ||
| p* | 0.141 | 0.002 | 0.042 | ||||||||||||
| Motivates Me to Stay Smoke-Free (Non-Smokers) | 175 | 8.5 ± 2.5 | 10.0 | 8.6 ± 2.4 | 10.0 | 8.6 ± 2.4 | 10.0 | 8.6 ± 2.4 | 10.0 | 8.7 ± 2.3 | 10.0 | 8.7 ± 2.3 | 10.0 | ||
| p* | 0.229 | 0.805 | 0.911 | ||||||||||||
| Makes Me Think about Quitting (Smokers) | 628 | 6.1 ± 3.4 | 6.0 | 5.9 ± 3.4 | 6.0 | 6.1 ± 3.4 | 6.0 | 5.9 ± 3.4 | 6.0 | 6.1 ± 3.4 | 7.0 | 6.1 ± 3.4 | 7.0 | ||
| p* | 0.076 | 0.027 | 0.431 | ||||||||||||
| Motivates Me to Quit Smoking (Smokers) | 624 | 6.1 ± 3.5 | 6.0 | 6.0 ± 3.4 | 6.0 | 6.1 ± 3.4 | 6.0 | 5.9 ± 3.4 | 6.0 | 6.1 ± 3.4 | 7.0 | 6.1 ± 3.4 | 7.0 | ||
| p* | 0.219 | 0.001 | 0.490 | ||||||||||||
| Makes Me Avoid Looking at the Warning Label | 799 | 5.9 ± 3.5 | 6.0 | 5.9 ± 3.5 | 6.0 | 5.8 ± 3.5 | 6.0 | 5.7 ± 3.5 | 6.0 | 6.1 ± 3.5 | 7.0 | 6.2 ± 3.5 | 7.0 | ||
| p* | 0.842 | 0.040 | 0.985 | ||||||||||||
| In General, How Effective is This Warning | 797 | 7.1 ± 3.1 | 8.0 | 6.9 ± 3.2 | 8.0 | 7.2 ± 3.0 | 8.0 | 7.1 ± 3.0 | 8.0 | 7.0 ± 3.2 | 8.0 | 7.1 ± 3.1 | 8.0 | ||
| p* | 0.016 | 0.007 | 0.714 | ||||||||||||
| Overall Rating Score | Average Rating Score of All RELIGIOUS HWLs | Average Rating Score of All NONRELIGIOUS HWLs | |||||||||||||
| Mean ± SD | Median | Mean ± SD | Median | ||||||||||||
| 815 | 6.8 ± 2.6 | 7.2 | 6.9 ± 2.6 | 7.3 | |||||||||||
| p* | 0.005 | ||||||||||||||
| Rating Questions | n | Nonreligious Death | Religious Death | Nonreligious SHS | Religious SHS | Nonreligious Gangrene | Religious Gangrene |
|---|---|---|---|---|---|---|---|
| GMR * (95%CI) | GMR * (95%CI) | GMR* (95%CI) | GMR* (95%CI) | GMR* (95%CI) | GMR* (95%CI) | ||
| Grabs My Attention | 810 | 1.01 (0.98–1.04) | 1.04 (1.01–1.07) | 1.04 (1.01–1.06) | 1.03 (0.99–1.05) | 1.01 (0.97–1.03) | 1.02 (0.99–1.05) |
| Easy to Understand | 810 | 1.02 (0.99–1.05) | 0.99 (0.96–1.02) | 0.99 (0.97–1.02) | 0.97 (0.95–0.99) | 0.99 (0.97–1.02) | 1.03 (0.99–1.06) |
| Credible | 804 | 1.05 (1.01–1.09) | 1.07 (1.02–1.12) | 1.05 (1.02–1.09) | 1.07 (1.03–1.11) | 1.06 (1.02–1.11) | 1.08 (1.04–1.13) |
| Makes Me Feel More Concerned about Smoking | 807 | 1.02 (0.99–1.06) | 1.04 (1.01–1.07) | 1.04 (0.99–1.07) | 1.04 (1.01–1.08) | 1.02 (0.99–1.05) | 1.02 (0.99–1.05) |
| Makes Me Think about the Health Risks of Smoking | 804 | 1.03 (0.99–1.06) | 1.04 (1.01–1.07) | 1.05 (1.02–1.09) | 1.03 (0.99–1.07) | 1.02 (0.98–1.05) | 1.02 (0.98–1.05) |
| Motivates Me to Stay Smoke-Free (Non-Smokers) | 175 | 0.98 (0.91–1.05) | 1.02 (0.96–1.09) | 1.03 (0.96–1.11) | 0.97 (0.91–1.04) | 1.04 (0.97–1.12) | 0.99 (0.93–1.05) |
| Makes Me Think about Quitting (Smokers) | 628 | 1.04 (0.99–1.08) | 1.05 (1.01–1.09) | 1.03 (0.99–1.07) | 1.05 (1.02–1.11) | 1.03 (0.99–1.07) | 1.02 (0.98–1.06) |
| Motivates Me to Quit Smoking (Smokers) | 624 | 1.03 (0.99–1.08) | 1.04 (1.01–1.08) | 1.03 (0.99–1.07) | 1.04 (0.99–1.09) | 1.03 (0.98–1.07) | 1.01 (0.97–1.04) |
| Makes Me Avoid Looking at the Warning Label | 799 | 1.02 (0.98–1.07) | 1.01 (0.96–1.05) | 1.02 (0.97–1.07) | 1.01 (0.95–1.05) | 1.01 (0.96–1.05) | 0.99 (0.95–1.04) |
| In General, How Effective is This Warning | 797 | 1.01 (0.98–1.03) | 1.02 (0.99–1.05) | 1.02 (0.99–1.05) | 0.99 (0.96–1.02) | 1.01 (0.97–1.03) | 0.99 (0.96–1.02) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaplan, B.; Hardesty, J.J.; Martini, S.; Megatsari, H.; Kennedy, R.D.; Cohen, J.E. The Effectiveness of Cigarette Pack Health Warning Labels with Religious Messages in an Urban Setting in Indonesia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 4287. https://doi.org/10.3390/ijerph16214287
Kaplan B, Hardesty JJ, Martini S, Megatsari H, Kennedy RD, Cohen JE. The Effectiveness of Cigarette Pack Health Warning Labels with Religious Messages in an Urban Setting in Indonesia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(21):4287. https://doi.org/10.3390/ijerph16214287
Chicago/Turabian StyleKaplan, Bekir, Jeffrey J. Hardesty, Santi Martini, Hario Megatsari, Ryan D. Kennedy, and Joanna E. Cohen. 2019. "The Effectiveness of Cigarette Pack Health Warning Labels with Religious Messages in an Urban Setting in Indonesia: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 21: 4287. https://doi.org/10.3390/ijerph16214287
APA StyleKaplan, B., Hardesty, J. J., Martini, S., Megatsari, H., Kennedy, R. D., & Cohen, J. E. (2019). The Effectiveness of Cigarette Pack Health Warning Labels with Religious Messages in an Urban Setting in Indonesia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 16(21), 4287. https://doi.org/10.3390/ijerph16214287