Tooth Malformations, DMFT Index, Speech Impairment and Oral Habits in Patients with Fetal Alcohol Syndrome

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Participants
2.2. Variables and Data Sources/Management
- White/cream: 1
- Yellow/brown: 2
- Diffuse-lines: 3
- Diffuse-patchy: 4
- Diffuse-confluent: 5
- Confluent/patchy + staining + loss of enamel: 6
- Pits: 7
- Missing enamel: 8
2.3. Bias
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. There Was No Gender and Age Discrimination among the Participants
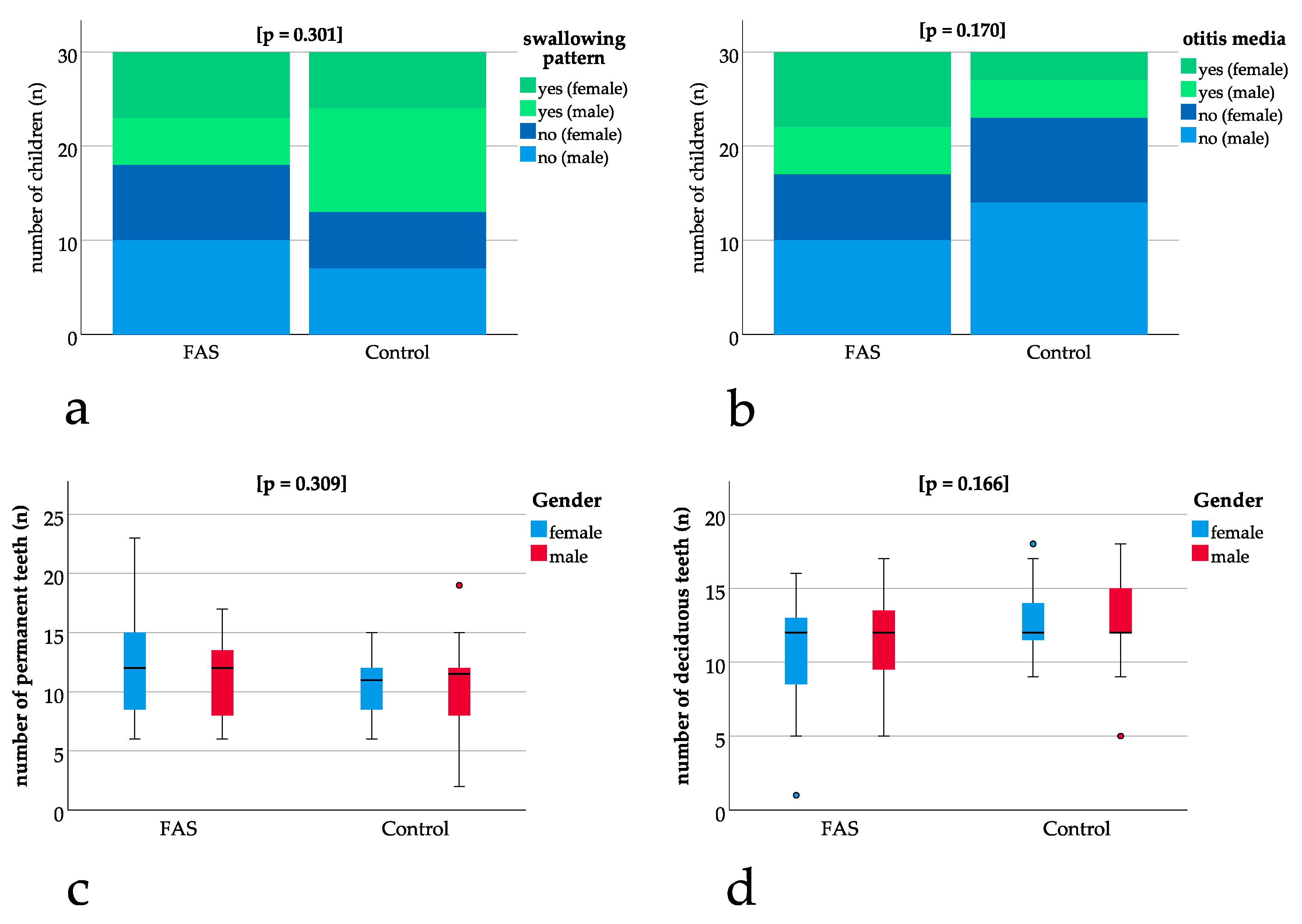
3.2. No Significant Difference for Exfoliation of Teeth, Swallowing Pattern and Otitis Media
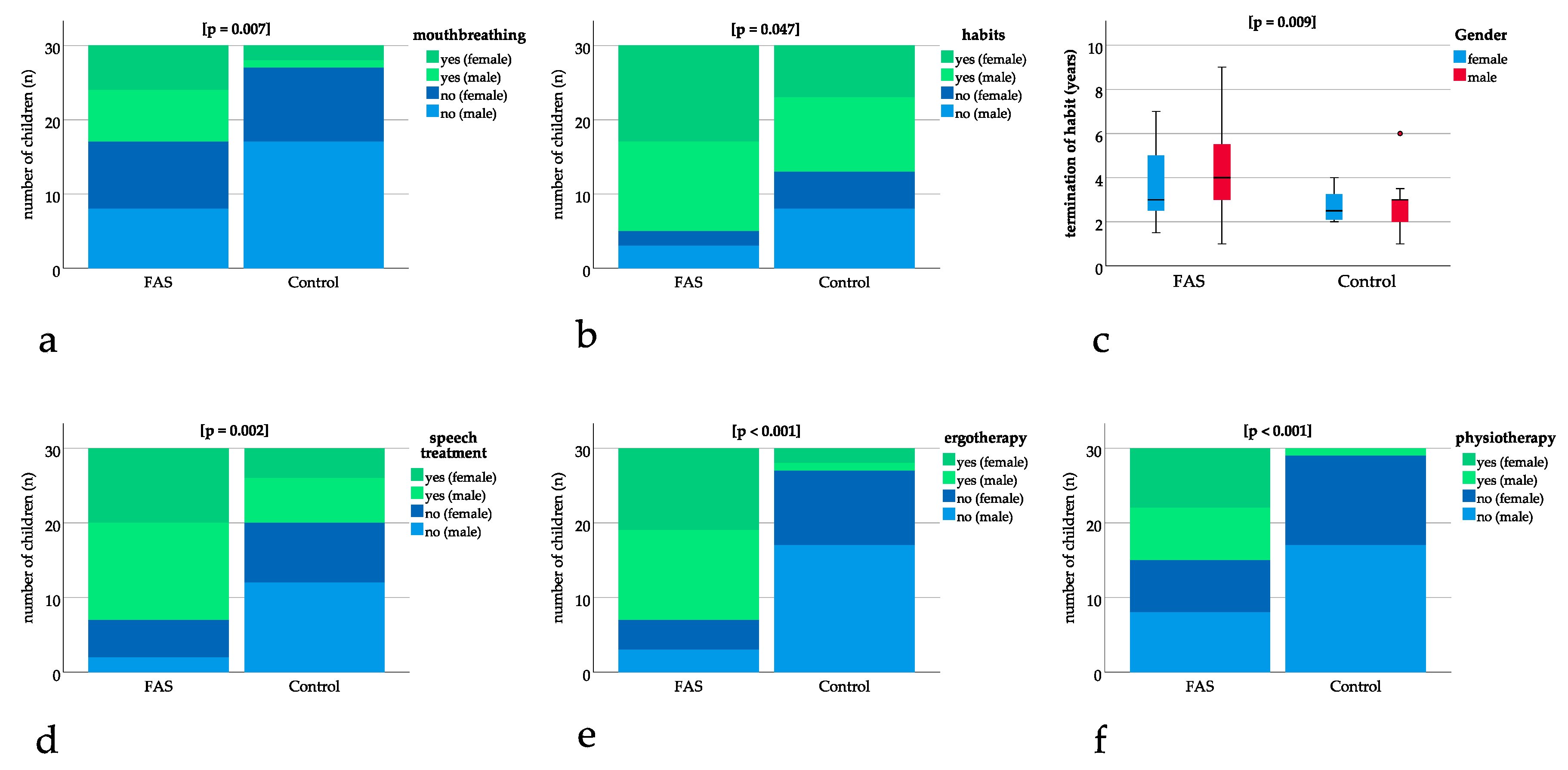
3.3. Mouthbreathing and Age at Termination of Habits was Significantly Higher for Children with FAS
3.4. Speech Treatment, Ergotherapy, and Physiotherapy was Significantly More Frequent in Patients with FAS
3.5. A Significant Difference Could be Found for Breastfeeding
3.6. Modified DDE Index and DMFT Index were Significantly Different in Patients with FAS
4. Discussion
4.1. General Findings
4.2. Significant Differences in Modified DDE Index and DMFT Index May Be Caused by Abnormal Eating Behaviour in Children with FAS
4.3. Reduced Motor Skills Might be a Reason for the Higher DMFT Index in Patients with FAS
4.4. Higher Need for Speech Treatment May be Associated with Hearing Disorders and Otitis Media in Patients with FAS
4.5. Mouthbreathing, Reduced Breastfeeding, and Habits Can be Associated with Malocclusion
4.6. Oral Health Prevention Programs, as Well as Early Interdisciplinary Consultation of Specialists, are Important Measures for Children with FAS
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mukherjee, R. FASD: The current situation in the UK. Adv. Dual Diagn. 2019, 12, 1–5. [Google Scholar] [CrossRef]
- Landgraf, M.N.; Albers, L.; Rahmsdorf, B.; Vill, K.; Gerstl, L.; Lippert, M.; Heinen, F. Fetal alcohol spectrum disorders (FASD)—What we know and what we should know—The knowledge of German health professionals and parents. Eur. J. Paediatr. Neurol. Off. J. Eur. Paediatr. Neurol. Soc. 2018, 22, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Probst, C.; Gmel, G.; Rehm, J.; Burd, L.; Popova, S. Global Prevalence of Fetal Alcohol Spectrum Disorder Among Children and Youth: A Systematic Review and Meta-analysis. JAMA Pediatrics 2017, 171, 948–956. [Google Scholar] [CrossRef] [PubMed]
- Popova, S.; Lange, S.; Shield, K.; Burd, L.; Rehm, J. Prevalence of fetal alcohol spectrum disorder among special subpopulations: A systematic review and meta-analysis. Addiction 2019, 114, 1150–1172. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Chambers, C.D.; Kalberg, W.O.; Zellner, J.; Feldman, H.; Buckley, D.; Kopald, D.; Hasken, J.M.; Xu, R.; Honerkamp-Smith, G.; et al. Prevalence of Fetal Alcohol Spectrum Disorders in 4 US Communities. Jama 2018, 319, 474–482. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Baete, A.; Russo, J.; Elliott, A.J.; Blankenship, J.; Kalberg, W.O.; Buckley, D.; Brooks, M.; Hasken, J.; Abdul-Rahman, O.; et al. Prevalence and characteristics of fetal alcohol spectrum disorders. Pediatrics 2014, 134, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Astley, S.J.; Clarren, S.K. Diagnosing the full spectrum of fetal alcohol-exposed individuals: Introducing the 4-digit diagnostic code. Alcohol Alcohol. 2000, 35, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Greenbaum, R.; Koren, G. Fetal alcohol spectrum disorder—New diagnostic initiatives. Paediatr. Child Health 2002, 7, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Streissguth, A.P.; Bookstein, F.L.; Barr, H.M.; Sampson, P.D.; O’Malley, K.; Young, J.K. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J. Dev. Behav. Pediatrics 2004, 25, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Astley, S.J.; Clarren, S.K. Measuring the facial phenotype of individuals with prenatal alcohol exposure: Correlations with brain dysfunction. Alcohol Alcohol. 2001, 36, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Blanck-Lubarsch, M.; Dirksen, D.; Feldmann, R.; Sauerland, C.; Hohoff, A. 3D-Analysis of Mouth, Nose and Eye Parameters in Children with Fetal Alcohol Syndrome (FAS). Int. J. Environ. Res. Public Health 2019, 16, 2535. [Google Scholar] [CrossRef] [PubMed]
- Blanck-Lubarsch, M.; Dirksen, D.; Feldmann, R.; Sauerland, C.; Kirschneck, C.; Hohoff, A. Asymmetry-index and orthodontic facial analysis of children with foetal alcohol syndrome using 3D-facial scans. Pediatric Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Blanck-Lubarsch, M.; Dirksen, D.; Feldmann, R.; Sauerland, C.; Kirschneck, C.; Hohoff, A. 3D Analysis of Philtrum Depth in Children with Fetal Alcohol Syndrome. Alcohol Alcohol. 2019, 54, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Blanck-Lubarsch, M.; Flieger, S.; Feldmann, R.; Kirschneck, C.; Sauerland, C.; Hohoff, A. Malocclusion Can Give Additional Hints for Diagnosis of Fetal Alcohol Spectrum Disorder. Alcohol Alcohol. 2019, 54, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Muggli, E.; Matthews, H.; Penington, A.; Claes, P.; O’Leary, C.; Forster, D.; Donath, S.; Anderson, P.J.; Lewis, S.; Nagle, C.; et al. Association Between Prenatal Alcohol Exposure and Craniofacial Shape of Children at 12 Months of Age. JAMA Pediatrics 2017, 171, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, G.; Malcolm-Smith, S.; Adnams, C.; Stein, D.J.; Donald, K.A.M. Effects of prenatal alcohol exposure on language, speech and communication outcomes: A review longitudinal studies. Acta Neuropsychiatr. 2019, 31, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Terband, H.; Spruit, M.; Maassen, B. Speech Impairment in Boys with Fetal Alcohol Spectrum Disorders. Am. J. Speech Lang. Pathol. 2018, 27, 1405–1425. [Google Scholar] [CrossRef] [PubMed]
- Soxman, J.A.; Wunsch, P.B.; Haberland, C.M. Anomalies of Enamel Formation. In Anomalies of the Developing Dentition: A Clinical Guide to Diagnosis and Management; Springer International Publishing: Cham, Switzerland, 2019; pp. 109–121. [Google Scholar]
- Matthiessen, M.E.; Romert, P. Changes of secretory ameloblasts in mini-pig fetuses exposed to ethanol in vivo. J. Dent. Res. 1988, 67, 1402–1404. [Google Scholar] [CrossRef] [PubMed]
- Sant’Anna, L.B.; Tosello, D.O.; Pasetto, S. Effects of maternal ethanol intake on immunoexpression of epidermal growth factor in developing rat mandibular molar. Arch. Oral Biol. 2005, 50, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, J.; O’Mullane, D. A modified DDE Index for use in epidemiological studies of enamel defects. J. Dent. Res. 1989, 68, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Luz, C.L.; Garib, D.G.; Arouca, R. Association between breastfeeding duration and mandibular retrusion: A cross-sectional study of children in the mixed dentition. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Caramez da Silva, F.; Justo Giugliani, E.R.; Capsi Pires, S. Duration of breastfeeding and distoclusion in the deciduous dentition. Breastfeed. Med. 2012, 7, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Romero, C.C.; Scavone-Junior, H.; Garib, D.G.; Cotrim-Ferreira, F.A.; Ferreira, R.I. Breastfeeding and non-nutritive sucking patterns related to the prevalence of anterior open bite in primary dentition. J. Appl. Oral Sci. 2011, 19, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Adair, S.M.; Milano, M.; Lorenzo, I.; Russell, C. Effects of current and former pacifier use on the dentition of 24- to 59-month-old children. Pediatric Dent. 1995, 17, 437–444. [Google Scholar]
- Duncan, K.; McNamara, C.; Ireland, A.J.; Sandy, J.R. Sucking habits in childhood and the effects on the primary dentition: Findings of the Avon Longitudinal Study of Pregnancy and Childhood. Int. J. Paediatr. Dent. Br. Paedodontic Soc. Int. Assoc. Dent. Child. 2008, 18, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.P.W. Auswirkung von Schnullern auf das Gebiss-eine Literaturübersicht. Inf. Orthod. Kieferorthop. 2009, 41, 191–198. [Google Scholar] [CrossRef]
- Grippaudo, C.; Paolantonio, E.G.; Antonini, G.; Saulle, R.; La Torre, G.; Deli, R. Association between oral habits, mouth breathing and malocclusion. Acta Otorhinolaryngol. Ital. 2016, 36, 386–394. [Google Scholar] [PubMed]
- Miller, J.; Hobson, P.; Gaskell, T.J. A serial study of the chronology of exfoliation of deciduous teeth and eruption of permanent teeth. Arch. Oral Biol. 1965, 10, 805–818. [Google Scholar] [CrossRef]
- WHO Oral Health Surveys: Basic Methods. Available online: https://www.who.int/oral_health/publications/9789241548649/en/ (accessed on 17 June 2019).
- Klein, H.; Palmer, C. Dental Caries in American Indian Children. J. Am. Dent. Assoc. 1938, 25, 996–998. [Google Scholar]
- Eslamipour, F.; Borzabadi-Farahani, A.; Asgari, I. The relationship between aging and oral health inequalities assessed by the DMFT index. Eur. J. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2010, 11, 193–199. [Google Scholar]
- Dabiri, D.; Eckert, G.J.; Li, Y.; Seow, K.; Schroth, R.J.; Warren, J.; Wright, J.T.; Zhao, S.; Fontana, M. Diagnosing Developmental Defects of Enamel: Pilot Study of Online Training and Accuracy. Pediatric Dent. 2018, 40, 105–109. [Google Scholar]
- Naidoo, S.; Chikte, U.; Laubscher, R.; Lombard, C. Fetal alcohol syndrome: Anthropometric and oral health status. J. Contemp. Dent. Pract. 2005, 6, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Amos-Kroohs, R.M.; Fink, B.A.; Smith, C.J.; Chin, L.; Van Calcar, S.C.; Wozniak, J.R.; Smith, S.M. Abnormal Eating Behaviors Are Common in Children with Fetal Alcohol Spectrum Disorder. J. Pediatrics 2016, 169, 194–200.e1. [Google Scholar] [CrossRef] [PubMed]
- Duval-White, C.J.; Jirikowic, T.; Rios, D.; Deitz, J.; Olson, H.C. Functional handwriting performance in school-age children with fetal alcohol spectrum disorders. Am. J. Occup. Ther. 2013, 67, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Lucas, B.R.; Doney, R.; Latimer, J.; Watkins, R.E.; Tsang, T.W.; Hawkes, G.; Fitzpatrick, J.P.; Oscar, J.; Carter, M.; Elliott, E.J. Impairment of motor skills in children with fetal alcohol spectrum disorders in remote Australia: The Lililwan Project. Drug Alcohol Rev. 2016, 35, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Lucas, B.R.; Latimer, J.; Pinto, R.Z.; Ferreira, M.L.; Doney, R.; Lau, M.; Jones, T.; Dries, D.; Elliott, E.J. Gross motor deficits in children prenatally exposed to alcohol: A meta-analysis. Pediatrics 2014, 134, e192–e209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellomo, F.; de Preux, F.; Chung, J.P.; Julien, N.; Budtz-Jorgensen, E.; Muller, F. The advantages of occupational therapy in oral hygiene measures for institutionalised elderly adults. Gerodontology 2005, 22, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Church, M.W.; Eldis, F.; Blakley, B.W.; Bawle, E.V. Hearing, language, speech, vestibular, and dentofacial disorders in fetal alcohol syndrome. Alcohol. Clin. Exp. Res. 1997, 21, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Church, M.W.; Kaltenbach, J.A. Hearing, speech, language, and vestibular disorders in the fetal alcohol syndrome: A literature review. Alcohol. Clin. Exp. Res. 1997, 21, 495–512. [Google Scholar] [PubMed]
- Popova, S.; Lange, S.; Shield, K.; Mihic, A.; Chudley, A.E.; Mukherjee, R.A.; Bekmuradov, D.; Rehm, J. Comorbidity of fetal alcohol spectrum disorder: A systematic review and meta-analysis. Lancet 2016, 387, 978–987. [Google Scholar] [CrossRef]
- Thomaz, E.; Alves, C.M.C.; Gomes, E.S.L.F.; Ribeiro de Almeida, C.C.C.; Soares de Britto, E.A.M.T.S.; Hilgert, J.B.; Wendland, E.M. Breastfeeding Versus Bottle Feeding on Malocclusion in Children: A Meta-Analysis Study. J. Hum. Lact. 2018, 34, 768–788. [Google Scholar] [CrossRef] [PubMed]
- Schmid, K.M.; Kugler, R.; Nalabothu, P.; Bosch, C.; Verna, C. The effect of pacifier sucking on orofacial structures: A systematic literature review. Prog. Orthod. 2018, 19, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Investigated Parameters | Total | FAS-Group | Control-Group | p Value |
|---|---|---|---|---|
| Gender (n) | 0.604 2 | |||
| Female | 27 | 15 | 12 | |
| Male | 33 | 15 | 18 | |
| Age at examination (years) | 0.122 1 | |||
| Mean (SD) | 8.5 (1.6) | 8.8 (1.4) | 8.2 (1.8) | |
| Median (Range) | 8.3 (5.8–11.9) | 8.6 (6.6–11.2) | 7.6 (5.8–11.9) | |
| Swallowing pattern (n) | 0.301 2 | |||
| Adult | 29 | 12 | 17 | |
| Infantile | 31 | 18 | 13 | |
| Mouthbreathing (n) | 0.007 2 | |||
| Yes | 16 | 13 | 3 | |
| No | 44 | 17 | 27 | |
| Oral habits (n) | 0.047 2 | |||
| Yes | 42 | 25 | 17 | |
| No | 18 | 5 | 13 | |
| Age at habit termination (years) | 0.009 1 | |||
| Mean (SD) | 3.6 (1.8) | 4.1 (1.9) | 2.8 (1.1) | |
| Median (Range) | 3.0 (1.0–9.0) | 4.0 (1.0–9.0) | 2.8 (1.0–6.0) | |
| Speech therapy (n) | 0.002 2 | |||
| Treatment | 33 | 23 | 10 | |
| No treatment | 27 | 7 | 20 | |
| Ergotherapy (n) | < 0.001 2 | |||
| Treatment | 26 | 23 | 3 | |
| No treatment | 34 | 7 | 27 | |
| Physiotherapy (n) | < 0.001 2 | |||
| Treatment | 16 | 15 | 1 | |
| No treatment | 44 | 15 | 29 | |
| Breastfeeding (n) | < 0.001 2 | |||
| Yes | 24 | 0 | 24 | |
| No | 36 | 30 | 6 | |
| Duration of breastfeeding (months) | < 0.001 1 | |||
| Mean (SD) | - | 0 | 6.1 (5.1) | |
| Median (Range) | - | 0 | 6 (0–24) | |
| Exfoliation of teeth (n) | 1.000 2 | |||
| Normal | 59 | 29 | 30 | |
| Dentitio praecox/tarda | 1 | 1 | 0 | |
| Otitis media (n) | 0.170 2 | |||
| Yes | 20 | 13 | 7 | |
| No | 40 | 17 | 23 | |
| Ratio permanent teeth with enamel defect/number of permanent teeth | 0.001 1 | |||
| Mean (SD) | 0.28 (0.27) | 0.39 (0.27) | 0.17 (0.20) | |
| Median (Range) | 0.23 (0–1) | 0.36 (0–1) | 0.12 (0–0.6) | |
| Ratio DDE index/number of permanent teeth with enamel defect | 0.005 1 | |||
| Mean (SD) | 1.2 (1.2) | 1.6 (1.2) | 0.9 (1) | |
| Median (Range) | 1.0 (0–4.8) | 1.4 (0–4.8) | 1 (0–4.3) | |
| Ratio DMFT index/number of permanent and deciduous teeth | < 0.001 1 | |||
| Mean (SD) | 0.07 (0.1) | 0.13 (0.1) | 0.01 (0.03) | |
| Median (Range) | 0 (0–0.42) | 0.11 (0–0.42) | 0 (0–0.1) | |
| DMFT index | < 0.001 1 | |||
| Mean (SD) | 1.6 (2.2) | 2.8 (2.4) | 0.3 (0.6) | |
| Median (Range) | 0 (0–10) | 2.5 (0–10) | 0 (0–2) | |
| modified DDE index | 0.001 1 | |||
| Mean (SD) | 6.1 (8.1) | 9.5 (9.8) | 2.7 (3.6) | |
| Median (Range) | 3 (0–40) | 6.5 (0–40) | 1.5 (0–13) | |
| Number of permanent teeth with enamel defect (n) | 0.001 1 | |||
| Mean (SD) | 3.3 (3.2) | 4.7 (3.5) | 1.9 (2.2) | |
| Median (Range) | 2 (0–12) | 4 (0–12) | 1 (0–7) | |
| Number of deciduous teeth (n) | 0.166 1 | |||
| Mean (SD) | 11.8 (3.8) | 11 (4.1) | 12.6 (3.3) | |
| Median (Range) | 12 (1–18) | 12 (1–17) | 12 (5–18) | |
| Number of permanent teeth (n) | 0.309 1 | |||
| Mean (SD) | 11.3 (3.9) | 11.9 (4.2) | 10.6 (3.4) | |
| Median (Range) | 12 (2–23) | 12 (6–23) | 11.5 (2–19) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanck-Lubarsch, M.; Dirksen, D.; Feldmann, R.; Sauerland, C.; Hohoff, A. Tooth Malformations, DMFT Index, Speech Impairment and Oral Habits in Patients with Fetal Alcohol Syndrome. Int. J. Environ. Res. Public Health 2019, 16, 4401. https://doi.org/10.3390/ijerph16224401
Blanck-Lubarsch M, Dirksen D, Feldmann R, Sauerland C, Hohoff A. Tooth Malformations, DMFT Index, Speech Impairment and Oral Habits in Patients with Fetal Alcohol Syndrome. International Journal of Environmental Research and Public Health. 2019; 16(22):4401. https://doi.org/10.3390/ijerph16224401
Chicago/Turabian StyleBlanck-Lubarsch, Moritz, Dieter Dirksen, Reinhold Feldmann, Cristina Sauerland, and Ariane Hohoff. 2019. "Tooth Malformations, DMFT Index, Speech Impairment and Oral Habits in Patients with Fetal Alcohol Syndrome" International Journal of Environmental Research and Public Health 16, no. 22: 4401. https://doi.org/10.3390/ijerph16224401