Does a Different Household Registration Affect Migrants’ Access to Basic Public Health Services in China?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Main Variables
2.2.1. Dependent Variable
2.2.2. Independent Variables and Control Variables
2.3. Model
3. Results
3.1. Factor Analysis
3.2. Impact Path Analysis
4. Robustness Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Chen, Z.; Lu, M. Hukou social segmentation and trust: Empirical evidence from shanghai. J. World Econ. 2009, 10, 81–96. [Google Scholar]
- Sun, W.; Bai, C.; Xie, P. The effect on rural labor mobility from registration system reform in China. Econ. Res. J. 2011, 1, 28–41. [Google Scholar]
- Du, Y.; Cai, F.; Qu, X.; Cheng, J. Sustain the China miracle:reaping the dividens from Hukou reforms. Econ. Res. J. 2014, 8, 4–13. [Google Scholar]
- Wu, J.; Yao, X.; Zhang, J. Is Hukou discrimination between urban and rural areas vanishing? Evidence from the reform period 1989–2011. Econ. Res. J. 2015, 11, 148–160. [Google Scholar]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- National Research Council Institute of Medicine. From Generation to Generation: The Health and Well-Being of Children in Immigrant Families; National Academy Press: Washington, DC, USA, 1998. [Google Scholar]
- Blewett, L.A.; Johnson, P.J.; Mach, A.L. Immigrant children’s access to health care: Differences by global region of birth. J. Health Care Poor Underserved 2010, 21, 13–31. [Google Scholar] [CrossRef]
- Nielsen, S.S.; Hempler, N.F.; Waldorff, F.B.; Kreiner, S.; Krasnik, A. Is there equity in use of healthcare services among immigrants, their descendents, and ethnic Danes? Scand. J. Public Health 2012, 40, 260–270. [Google Scholar] [CrossRef]
- Garcia-Perez, M. Health care usage and health status of immigrant children: The effects of nativity versus citizenship. Am. Econ. Rev. 2013, 103, 412–417. [Google Scholar] [CrossRef]
- Wang, M. Difference between Job Opportunity and Wage in Urban Labor Market: Research on Migration Labor Employment and Remuneration Social Sciences in China. Soc. Sci. China 2005, 5, 36–46. [Google Scholar]
- Xing, C.; Jia, S.; Li, S. Regional Distribution of the Return to Education for Rural-to-Urban Migrants and Its Impact on Migration. Econ. Res. J. 2013, 11, 114–126. [Google Scholar]
- Zhang, X. Education, Migration and the Urban-Rural Difference in Returns to Education. Econ. Res. J. 2017, 12, 164–178. [Google Scholar]
- Zhou, W.; Zhao, F.; Yang, F.; Li, L. Land transfer, reform of household registration system and urbanization in China: Theoretical and simulation test. Econ. Res. J. 2017, 52, 183–197. [Google Scholar]
- Wang, Y.; Gao, X. The political economy of endogenous dual economy: Public goods, labor market and tax rate. J. World Econ. 2016, 39, 3–22. [Google Scholar]
- Yao, Y.; Liu, B.; Liu, G.; Zang, W. Medical insurance, household registration system and healthcare utilization—Evidence from charls data analysis. Insur. Stud. 2014, 6, 105–117. [Google Scholar]
- Tao, Y.H.; Shen, Y. Spatial difference of medical facility accessibility and influencing factors: A comparative study of registered and floating populations in Shanghai. Prog. Geogr. 2018, 37, 1075–1085. [Google Scholar] [CrossRef]
- Ma, C.; Qu, Z.; Song, Z. Inequality of opportunity of floating population’s health care under the integrated medical insurance system—paradox of the ex-ante or ex-post compensation principle. China Ind. Econ. 2018, 2, 100–117. [Google Scholar]
- Cai, H.; Li, Y. The impact of Hukou on family education expenditure: Analysis based on the CFPS data. Chin. J. Popul. 2019, 1, 76–87. [Google Scholar]
- Sudano, J.J., Jr.; Baker, D.W. Intermittent lack of health insurance coverage and use of preventive services. Am. J. Public Health 2003, 93, 130–137. [Google Scholar] [CrossRef]
- Liu, G.; Cai, C.; Li, L. Medical insurance and medical care demand for the elderly in China. Econ. Res. J. 2011, 3, 95–107. [Google Scholar]
- The Opinions of the State Council on Further Promoting the Reform of the Household Registration System. Available online: http://www.gov.cn/zhengce/content/2014-07/30/content_8944.htm (accessed on 30 July 2014).
- Chen, H.; Zhao, C.; Yang, L. Reverse discrimination mystery of the household registration: An explanation based on income compensation. J. World Econ. 2017, 40, 173–192. [Google Scholar]
- Manning, W.G.; Newhouse, J.P.; Duan, N.; Keeler, E.B.; Leibowitz, A. Health Insurance and the Demand for Medical Care. Am. Econ. Rev. 1987, 77, 251–277. [Google Scholar] [PubMed]
- Wei, T. Decentralization and development of smal and medium-sized cities—An analysis based on the policy of county-to-city upgrade in China. China Econ. Q. 2019, 18, 123–150. [Google Scholar]
- Abadie, A.; Imbens, G.W. Large sample properties of matching estimators for average treatment effects. Econometrica 2006, 74, 235–267. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Variable Definitions | Total Sample | Agricultural Household Registration | Non-Agricultural Household Registration | Difference between the Two Groups of Samples | |||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |||
| y1 | Health record established (= 1; else = 0) | 0.36 | 0.481 | 0.36 | 0.48 | 0.38 | 0.486 | −0.024 *** |
| y2 | Health knowledge learned in the inflow area (= 1; else = 0) | 0.95 | 0.214 | 0.95 | 0.215 | 0.96 | 0.207 | −0.004 * |
| Gender | Male (= 1,female = 0) | 0.58 | 0.494 | 0.58 | 0.494 | 0.57 | 0.495 | 0.008 *** |
| Marital status | Marital status (married = 1; other = 0) | 0.80 | 0.4 | 0.81 | 0.394 | 0.75 | 0.431 | 0.053 *** |
| Age | Age (15–60) | 34.98 | 9.279 | 34.92 | 9.343 | 35.32 | 8.875 | −0.399 *** |
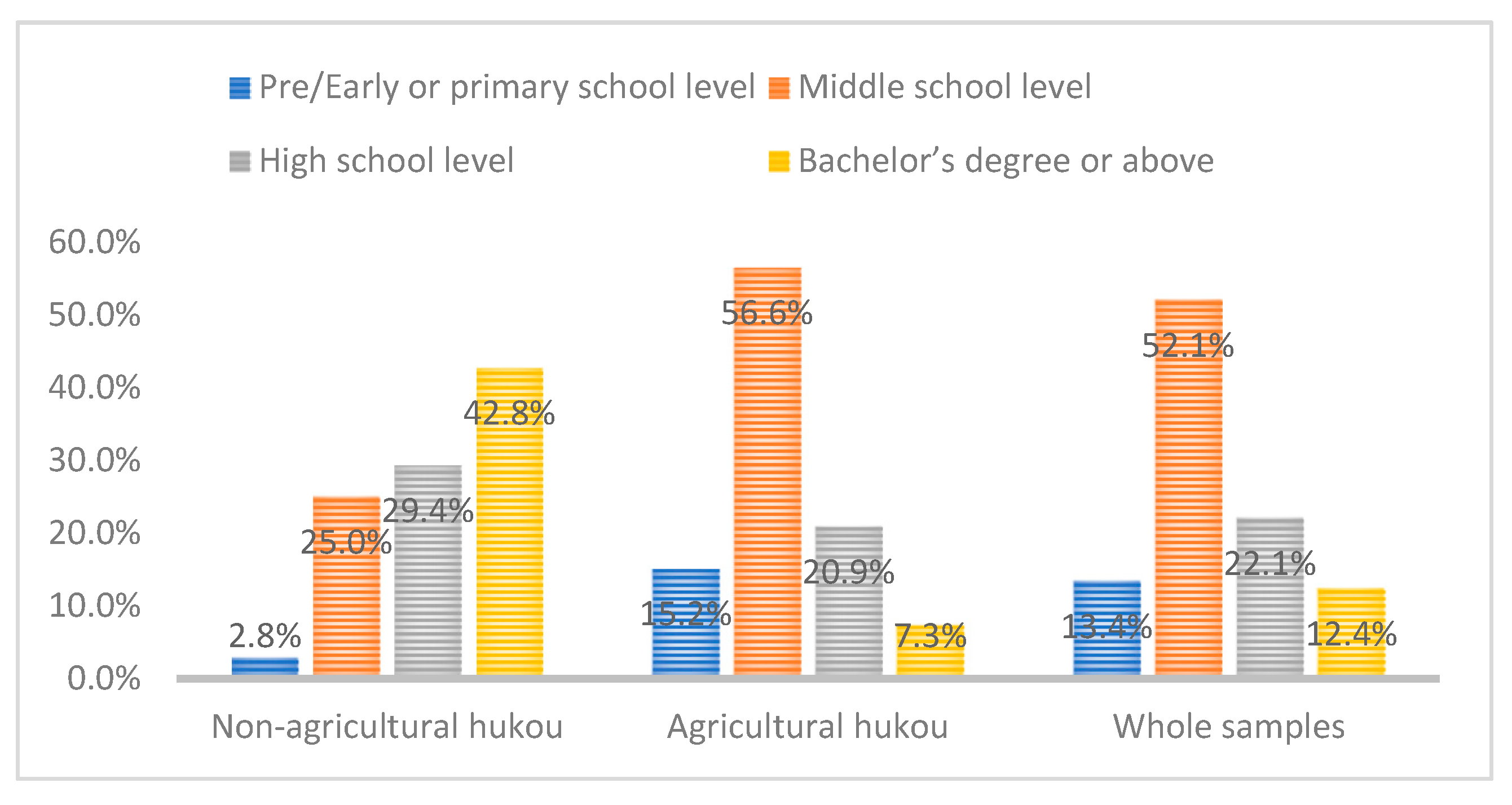
| Education level | Pre/early or primary school level (= 1; other = 0) | 0.13 | 0.341 | 0.15 | 0.359 | 0.03 | 0.165 | 0.124 *** |
| Middle school level (= 1; else = 0) | 0.52 | 0.50 | 0.57 | 0.496 | 0.25 | 0.433 | 0.315 *** | |
| High school level (= 1; else = 0) | 0.22 | 0.415 | 0.21 | 0.407 | 0.29 | 0.455 | −0.085 *** | |
| Bachelor’s degree or above (= 1; else = 0) | 0.12 | 0.33 | 0.07 | 0.261 | 0.43 | 0.495 | −0.355 *** | |
| Flow pattern | Intercountry within the city (= 1; other = 0) | 0.2 | 0.398 | 0.20 | 0.396 | 0.21 | 0.407 | −0.014 *** |
| Intercity within the province (= 1; other = 0) | 0.31 | 0.462 | 0.31 | 0.461 | 0.32 | 0.468 | −0.02 *** | |
| Trans-provincial (= 1; other = 0) | 0.49 | 0.5 | 0.50 | 0.500 | 0.47 | 0.499 | 0.034 *** | |
| Attend medical insurance | Medical insurance (= 1; other = 0) | 0.94 | 0.243 | 0.94 | 0.231 | 0.90 | 0.301 | 0.044 *** |
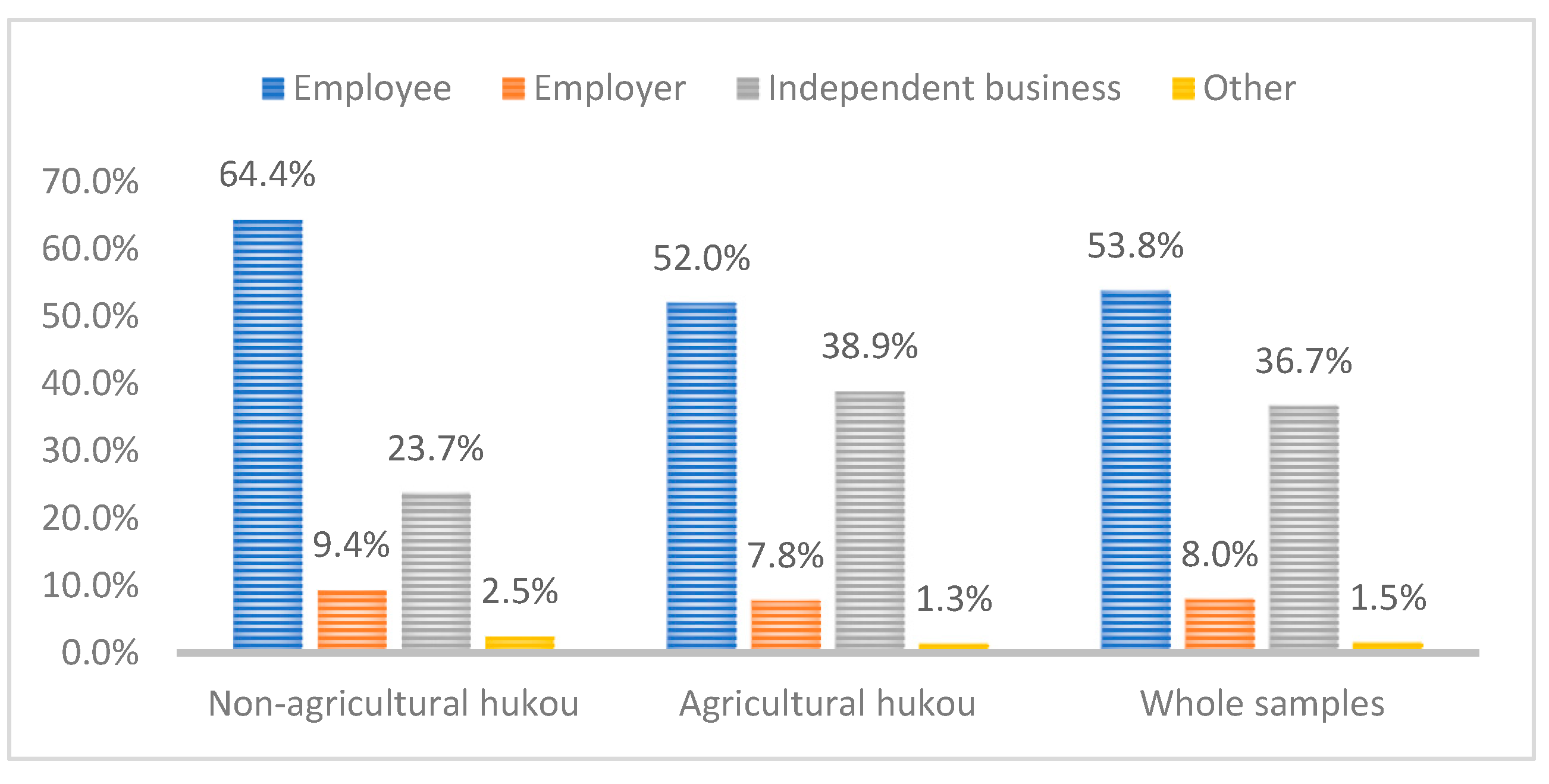
| Employment status | Employee (= 1; other = 0) | 0.54 | 0.499 | 0.52 | 0.500 | 0.64 | 0.479 | −0.124 *** |
| Employer (= 1; other = 0) | 0.08 | 0.272 | 0.08 | 0.268 | 0.09 | 0.292 | −0.016 *** | |
| Independent Business (= 1; other = 0) | 0.37 | 0.482 | 0.39 | 0.488 | 0.24 | 0.425 | −0.153 *** | |
| Other (= 1; other = 0) | 0.01 | 0.12 | 0.01 | 0.113 | 0.03 | 0.157 | −0.013 *** | |
| Long-term residence willingness (5 years) | Intend (= 1; other = 0) | 0.6 | 0.491 | 0.58 | 0.493 | 0.67 | 0.471 | −0.082 *** |
| No plan (= 1; other = 0) | 0.12 | 0.331 | 0.13 | 0.333 | 0.11 | 0.312 | 0.018 *** | |
| No idea (= 1; other = 0) | 0.28 | 0.448 | 0.29 | 0.453 | 0.22 | 0.417 | 0.064 *** | |
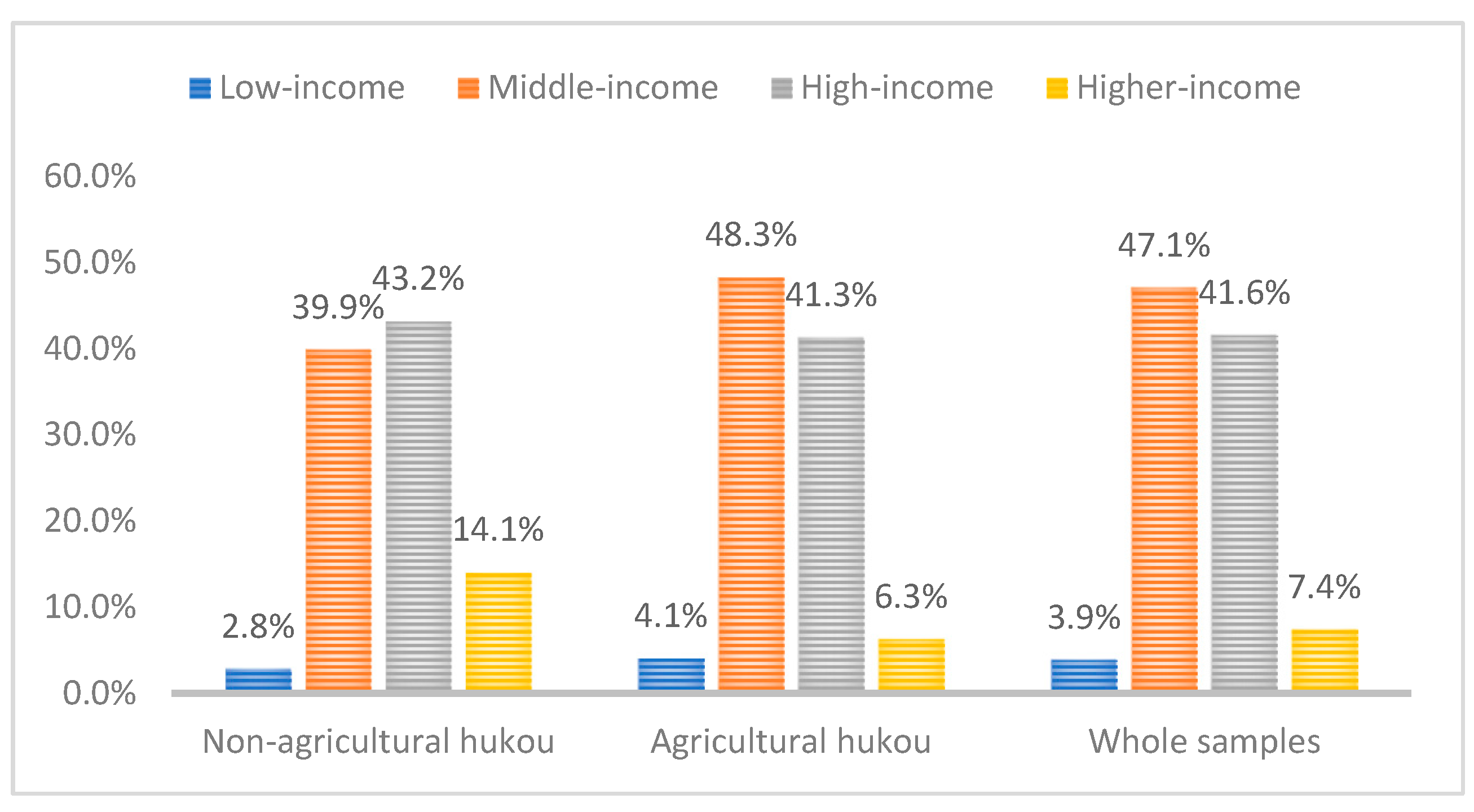
| Income | Low-income (= 1; other = 0) | 0.04 | 0.194 | 0.04 | 0.198 | 0.03 | 0.166 | 0.013 *** |
| Middle-income (=1; other = 0) | 0.47 | 0.499 | 0.48 | 0.500 | 0.40 | 0.490 | 0.084 *** | |
| High-income (= 1; other = 0) | 0.42 | 0.493 | 0.41 | 0.492 | 0.43 | 0.495 | −0.019 *** | |
| Higher-income (= 1; other = 0) | 0.07 | 0.263 | 0.06 | 0.244 | 0.14 | 0.348 | −0.077 *** | |
| Residence time (year) | Less than 3 years (= 1; other = 0) | 0.43 | 0.496 | 0.44 | 0.496 | 0.42 | 0.493 | 0.023 *** |
| 3 to 6years (= 1; other = 0) | 0.26 | 0.441 | 0.26 | 0.440 | 0.28 | 0.448 | −0.016 *** | |
| More than 6 years (= 1; other = 0) | 0.3 | 0.458 | 0.30 | 0.458 | 0.31 | 0.461 | −0.007 | |
| Sample area | East (= 1; other = 0) | 0.43 | 0.495 | 0.43 | 0.495 | 0.41 | 0.492 | 0.018 *** |
| Central (= 1; other = 0) | 0.18 | 0.386 | 0.19 | 0.391 | 0.15 | 0.356 | 0.039 *** | |
| West (= 1; other = 0) | 0.32 | 0.468 | 0.32 | 0.468 | 0.33 | 0.472 | −0.012 ** | |
| Northeast (= 1; other = 0) | 0.07 | 0.249 | 0.06 | 0.237 | 0.11 | 0.307 | −0.045 *** | |
| N | 59,443 | 50,937 | 8506 | |||||
| Dependent Variable | Y1 | Y2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Independent Variable | Factor | OR | OR 95% Confidence Interval | Factor | OR | OR 95% Confidence Interval | |||
| Minimum | Maximum | Minimum | Maximum | ||||||
| Hou | 0.066 ** (0.027) | 1.068 | 1.012 | 1.126 | 0.014 (0.063) | 1.014 | 0.896 | 1.147 | |
| Gender | −0.081 *** (0.018) | 0.922 | 0.891 | 0.955 | −0.404 *** (0.041) | 0.667 | 0.615 | 0.724 | |
| Age | 0.021 *** (0.008) | 1.022 | 1.006 | 1.038 | 0.064 *** (0.015) | 1.066 | 1.035 | 1.099 | |
| Age* age | 0.000 ** (0.000) | 1 | 1 | 1 | −0.001 *** (0.000) | 0.999 | 0.998 | 0.999 | |
| Marriage | 0.114 *** (0.029) | 1.121 | 1.06 | 1.186 | 0.593 *** (0.058) | 1.81 | 1.614 | 2.03 | |
| Education level | Middle school level | 0.113 *** (0.028) | 1.12 | 1.06 | 1.183 | 0.111 * (0.059) | 1.117 | 0.995 | 1.254 |
| High school level | 0.206 *** (0.033) | 1.229 | 1.153 | 1.31 | 0.240 *** (0.071) | 1.272 | 1.106 | 1.463 | |
| Bachelor’s degree or above | 0.16 *** (0.04) | 1.174 | 1.086 | 1.269 | 0.239 *** (0.09) | 1.27 | 1.065 | 1.514 | |
| Flow mode | Cross-city within the province | 0.057 ** (0.024) | 1.059 | 1.01 | 1.11 | 0.23 *** (0.058) | 1.259 | 1.123 | 1.41 |
| Cross-province | −0.515 *** (0.023) | 0.598 | 0.571 | 0.626 | 0.112 ** (0.056) | 1.119 | 1.003 | 1.248 | |
| Employment status | Employer | 0.124 *** (0.034) | 1.132 | 1.06 | 1.209 | −0.25 *** (0.075) | 0.779 | 0.673 | 0.901 |
| Self-employed workers | 0.115 *** (0.02) | 1.121 | 1.079 | 1.165 | −0.026 (0.046) | 0.974 | 0.89 | 1.066 | |
| Other | −0.025 (0.073) | 0.976 | 0.845 | 1.126 | 0.259 (0.179) | 1.296 | 0.913 | 1.839 | |
| Intended long-term residence in the local area (5 years) | No | −0.401 *** (0.029) | 0.669 | 0.632 | 0.709 | −0.126 ** (0.06) | 0.881 | 0.783 | 0.992 |
| Not yet | −0.17 *** (0.021) | 0.844 | 0.81 | 0.879 | −0.204 *** (0.045) | 0.816 | 0.747 | 0.891 | |
| Take part in health insurance | 0.167 *** (0.037) | 1.182 | 1.099 | 1.271 | 0.245 *** (0.071) | 1.278 | 1.113 | 1.468 | |
| Length of residence | 3-6 years | 0.116 *** (0.022) | 1.123 | 1.077 | 1.172 | 0.101 ** (0.05) | 1.106 | 1.004 | 1.22 |
| More than 6 years | 0.076 *** (0.022) | 1.079 | 1.033 | 1.127 | 0.026 (0.05) | 1.027 | 0.932 | 1.131 | |
| Income level | Middle | −0.009 (0.046) | 0.991 | 0.905 | 1.085 | 0.288 *** (0.086) | 1.334 | 1.127 | 1.578 |
| High | −0.099 ** (0.048) | 0.905 | 0.825 | 0.994 | 0.427 *** (0.091) | 1.533 | 1.283 | 1.833 | |
| Higher | −0.123 ** (0.057) | 0.884 | 0.791 | 0.988 | 0.664 *** (0.122) | 1.943 | 1.53 | 2.467 | |
| Region | Central | 0.316 *** (0.059) | 1.372 | 1.222 | 1.541 | ||||
| West | 0.775 *** (0.053) | 2.171 | 1.958 | 2.408 | |||||
| Northeast | −0.008 (0.073) | 0.992 | 0.86 | 1.144 | |||||
| Dependent Variable | Y1 | Y2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Independent Variable | Factor | Index of Regression Coefficients | OR 95% Confidence Interval | Factor | Index of Regression Coefficients | OR 95% Confidence Interval | ||
| Minimum | Maximum | Minimum | Maximum | |||||
| Middle school*Hou | 0.204 (0.148) | 1.227 | 0.918 | 1.639 | 0.097 (0.302) | 1.102 | 0.609 | 1.993 |
| High school*Hou | 0.098 (0.148) | 1.103 | 0.826 | 1.474 | 0.004 (0.304) | 1.004 | 0.554 | 1.821 |
| Undergraduate/Specialist or above *Hou | −0.005 (0.149) | 0.995 | 0.743 | 1.333 | −0.001 (0.309) | 0.999 | 0.545 | 1.829 |
| Cross-city in the province *Hou | −0.13 * (0.067) | 0.878 | 0.77 | 1.001 | −0.037 (0.169) | 0.964 | 0.692 | 1.341 |
| Cross-provincial *Hou | 0.056 (0.065) | 1.057 | 0.931 | 1.201 | −0.169 (0.154) | 0.844 | 0.624 | 1.142 |
| Middle income*Hou | 0.232 (0.15) | 1.261 | 0.94 | 1.691 | −0.294 (0.311) | 0.745 | 0.405 | 1.371 |
| High income*Hou | 0.328 ** (0.15) | 1.388 | 1.034 | 1.863 | −0.272 (0.315) | 0.762 | 0.411 | 1.411 |
| Higher income*Hou | −0.009 (0.164) | 0.991 | 0.718 | 1.367 | −0.444 (0.356) | 0.641 | 0.319 | 1.289 |
| Variable | Sample | Treated | Controls | Difference | S.E. | T-stat |
|---|---|---|---|---|---|---|
| y1 | Unmatched | 0.38349 | 0.35946 | 0.02403 | 0.0056 | 4.27 |
| ATT | 0.38349 | 0.37036 | 0.01313 | 0.0076 | 1.73 | |
| y2 | Unmatched | 0.95532 | 0.95127 | 0.00405 | 0.0025 | 1.62 |
| ATT | 0.95532 | 0.95518 | 0.00015 | 0.0032 | 0.05 |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meng, X. Does a Different Household Registration Affect Migrants’ Access to Basic Public Health Services in China? Int. J. Environ. Res. Public Health 2019, 16, 4615. https://doi.org/10.3390/ijerph16234615
Meng X. Does a Different Household Registration Affect Migrants’ Access to Basic Public Health Services in China? International Journal of Environmental Research and Public Health. 2019; 16(23):4615. https://doi.org/10.3390/ijerph16234615
Chicago/Turabian StyleMeng, Xia. 2019. "Does a Different Household Registration Affect Migrants’ Access to Basic Public Health Services in China?" International Journal of Environmental Research and Public Health 16, no. 23: 4615. https://doi.org/10.3390/ijerph16234615
APA StyleMeng, X. (2019). Does a Different Household Registration Affect Migrants’ Access to Basic Public Health Services in China? International Journal of Environmental Research and Public Health, 16(23), 4615. https://doi.org/10.3390/ijerph16234615