Correlation between Executive Network Integrity and Sarcopenia in Patients with Parkinson’s Disease

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sarcopenia-Associated Measurements
2.3. Diffusion Tensor Imaging (DTI) Acquisition
2.4. Data Preprocessing
2.5. Analysis of Demographic Data Differences between Groups
2.6. Analysis of Body Composition Differences between Groups
2.7. Analysis of Group Comparison of Fractional Anisotropy (FA) Values
2.8. Analysis of Regions of Interest
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Body Composition
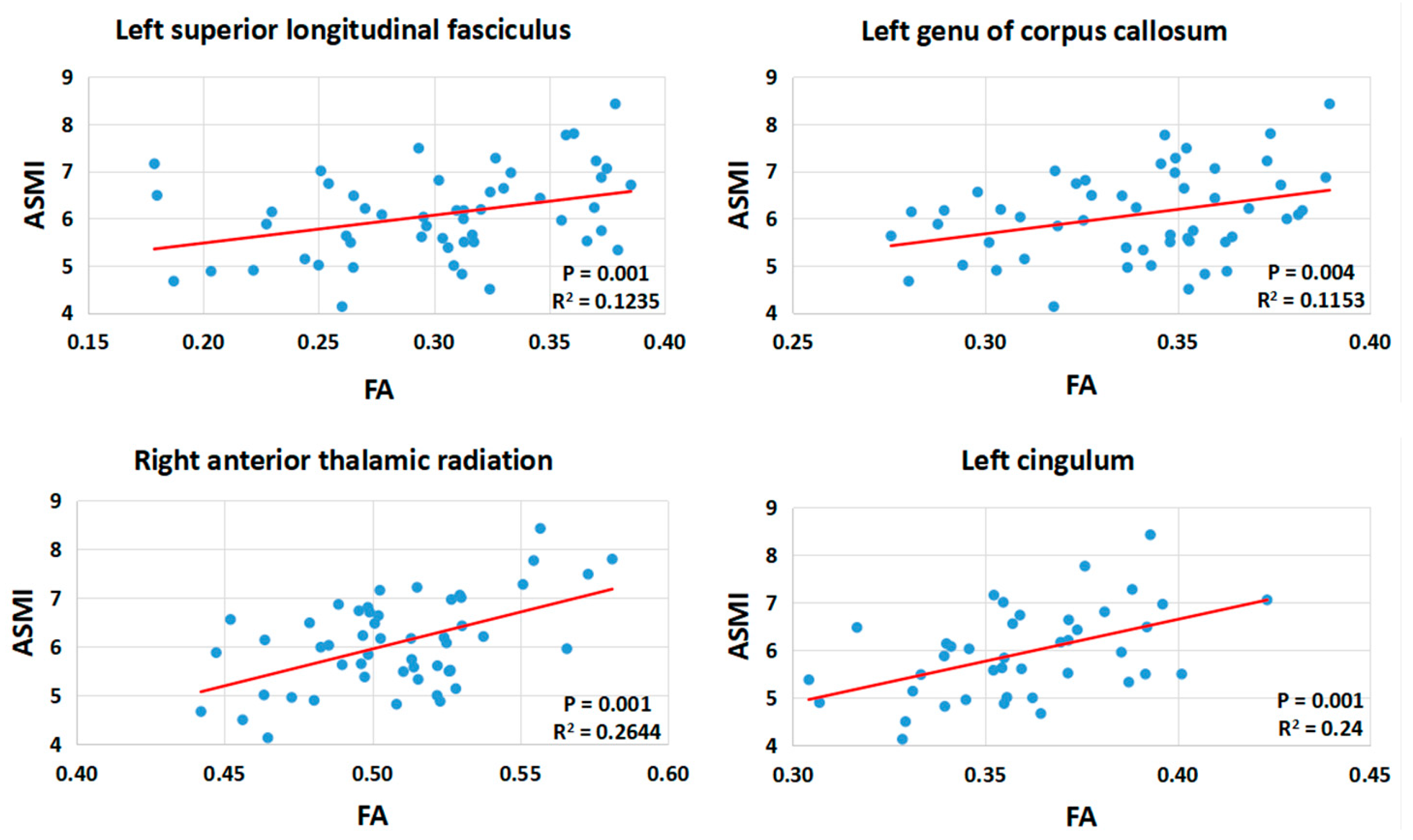
3.3. Brain Alterations in DTI
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| Axial diffusivity | AD |
| Appendicular skeletal muscle mass | ASM |
| Appendicular skeletal muscle mass index | ASMI |
| Body mass index | BMI |
| Corpus callosum | CC |
| Diffusion tensor imaging | DTI |
| Fractional anisotropy | FA |
| Levodopa Equivalent Daily Dose | LEDD |
| Mean diffusivity | MD |
| Normal control | NC |
| Parkinson’s disease | PD |
| PD patients with sarcopenia | PDSa |
| PD patients without sarcopenia | PDNSa |
| Radial diffusivity | RD |
| Regions of interest | ROI |
| Superior longitudinal fasciculus | SLF |
| Unified Parkinson’s Disease Rating Scale | UPDRS |
| White matter | WM |
References
- Goldman, J.G.; Litvan, I. Mild cognitive impairment in Parkinson’s disease. Minerva Med. 2011, 102, 441–459. [Google Scholar] [PubMed]
- Vetrano, D.L.; Pisciotta, M.S.; Laudisio, A.; Lo Monaco, M.R.; Onder, G.; Brandi, V.; Fusco, D.; Di Capua, B.; Ricciardi, D.; Bernabei, R.; et al. Sarcopenia in Parkinson Disease: Comparison of Different Criteria and Association with Disease Severity. J. Am. Med. Dir. Assoc. 2018, 19, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Shiozu, H.; Higashijima, M.; Koga, T. Association of sarcopenia with swallowing problems, related to nutrition and activities of daily living of elderly individuals. J. Phys. Ther. Sci. 2015, 27, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Rae, C.L.; Correia, M.M.; Altena, E.; Hughes, L.E.; Barker, R.A.; Rowe, J.B. White matter pathology in Parkinson’s disease: The effect of imaging protocol differences and relevance to executive function. Neuroimage 2012, 62, 1675–1684. [Google Scholar] [CrossRef] [PubMed]
- Dirnberger, G.; Jahanshahi, M. Executive dysfunction in Parkinson’s disease: A review. J. Neuropsychol. 2013, 7, 193–224. [Google Scholar] [CrossRef]
- Gross, A.L.; Xue, Q.L.; Bandeen-Roche, K.; Fried, L.P.; Varadhan, R.; McAdams-DeMarco, M.A.; Walston, J.; Carlson, M.C. Declines and Impairment in Executive Function Predict Onset of Physical Frailty. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1624–1630. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Wu, I.C.; Lin, C.C.; Hsiung, C.A.; Wang, C.Y.; Wu, C.H.; Chan, D.C.; Li, T.C.; Lin, W.Y.; Huang, K.C.; Chen, C.Y.; et al. Epidemiology of sarcopenia among community-dwelling older adults in Taiwan: A pooled analysis for a broader adoption of sarcopenia assessments. Geriatr. Gerontol. Int. 2014, 14 (Suppl. 1), 52–60. [Google Scholar] [CrossRef]
- Chen, H.L.; Lu, C.H.; Lin, H.C.; Chen, P.C.; Chou, K.H.; Lin, W.M.; Tsai, N.W.; Su, Y.J.; Friedman, M.; Lin, C.P.; et al. White matter damage and systemic inflammation in obstructive sleep apnea. Sleep 2015, 38, 361–370. [Google Scholar] [CrossRef]
- Drey, M.; Hasmann, S.E.; Krenovsky, J.P.; Hobert, M.A.; Straub, S.; Elshehabi, M.; von Thaler, A.K.; Fallgatter, A.J.; Eschweiler, G.W.; Suenkel, U.; et al. Associations between Early Markers of Parkinson’s Disease and Sarcopenia. Front. Aging Neurosci. 2017, 9, 53. [Google Scholar] [CrossRef]
- Ramaker, C.; Marinus, J.; Stiggelbout, A.M.; Van Hilten, B.J. Systematic evaluation of rating scales for impairment and disability in Parkinson’s disease. Mov. Disord. 2002, 17, 867–876. [Google Scholar] [CrossRef] [PubMed]
- Beyer, P.L.; Palarino, M.Y.; Michalek, D.; Busenbark, K.; Koller, W.C. Weight Change and Body Composition in Patients with Parkinson’s Disease. J. Am. Diet. Assoc. 1995, 95, 979–983. [Google Scholar] [CrossRef]
- Revilla, M.; Jiménez-Jiménez, F.; Villa, L.; Hernández, E.; Ortí-Pareja, M.; Gasalla, T.; Rico, H. Body composition in Parkinson’s disease: A study with dual-energy X-ray absorptiometry. Parkinsonism Relat. Disord. 1998, 4, 137–142. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Bernabei, R.; Onder, G.; Marzetti, E. Sarcopenia as the biological substrate of physical frailty. Clin. Geriatr. Med. 2015, 31, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Vikdahl, M.; Carlsson, M.; Linder, J.; Forsgren, L.; Håglin, L. Weight gain and increased central obesity in the early phase of Parkinson’s disease. Clin. Nutr. 2014, 33, 1132–1139. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, S.M.; Hernán, M.A.; Willett, W.C.; Ascherio, A. Weight loss in Parkinson’s disease. Ann. Neurol. 2003, 53, 676–679. [Google Scholar] [CrossRef]
- Tan, A.H.; Hew, Y.C.; Lim, S.Y.; Ramli, N.M.; Kamaruzzaman, S.B.; Tan, M.P.; Grossmann, M.; Ang, B.H.; Tan, J.Y.; Manap, M.A.A.A. Altered body composition, sarcopenia, frailty, and their clinico-biological correlates, in Parkinson’s disease. Parkinsonism Relat. Disord. 2018, 56, 58–64. [Google Scholar] [CrossRef]
- Noh, H.M.; Oh, S.; Song, H.J.; Lee, E.Y.; Jeong, J.Y.; Ryu, O.H.; Hong, K.S.; Kim, D.H. Relationships between cognitive function and body composition among community-dwelling older adults: A cross-sectional study. BMC Geriatr. 2017, 17, 259. [Google Scholar] [CrossRef]
- Tikhonoff, V.; Casiglia, E.; Guidotti, F.; Giordano, N.; Martini, B.; Mazza, A.; Spinella, P.; Palatini, P. Body fat and the cognitive pattern: A population-based study. Obesity 2015, 23, 1502–1510. [Google Scholar] [CrossRef]
- Tekin, S.; Cummings, J.L. Frontal-subcortical neuronal circuits and clinical neuropsychiatry: An update. J. Psychosom. Res. 2002, 53, 647–654. [Google Scholar] [CrossRef]
- Lin, W.C.; Chen, H.L.; Hsu, T.W.; Hsu, C.C.; Huang, Y.C.; Tsai, N.W.; Lu, C.H. Correlation between Dopamine Transporter Degradation and Striatocortical Network Alteration in Parkinson’s Disease. Front. Neurol. 2017, 8, 323. [Google Scholar] [CrossRef] [PubMed]
- Mamah, D.; Conturo, T.E.; Harms, M.P.; Akbudak, E.; Wang, L.; McMichael, A.R.; Gado, M.H.; Barch, D.M.; Csernansky, J.G. Anterior Thalamic Radiation Integrity in Schizophrenia: A Diffusion-Tensor Imaging Study. Psychiatry Res. Neuroimaging 2010, 183, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Kamali, A.; Flanders, A.E.; Brody, J.; Hunter, J.V.; Hasan, K.M. Tracing superior longitudinal fasciculus connectivity in the human brain using high resolution diffusion tensor tractography. Brain Struct. Funct. 2014, 219, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Fabri, M.; Pierpaoli, C.; Barbaresi, P.; Polonara, G. Functional topography of the corpus callosum investigated by DTI and fMRI. World J. Radiol. 2014, 6, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Bast, T. Toward an integrative perspective on hippocampal function: From the rapid encoding of experience to adaptive behavior. Rev. Neurosci. 2007, 18, 253–282. [Google Scholar] [CrossRef] [PubMed]
- Dreher, J.C.; Kohn, P.; Kolachana, B.; Weinberger, D.R.; Berman, K.F. Variation in dopamine genes influences responsivity of the human reward system. Proc. Natl. Acad. Sci. USA 2009, 106, 617–622. [Google Scholar] [CrossRef]
- Daly, M.; McMinn, D.; Allan, J.L. A bidirectional relationship between physical activity and executive function in older adults. Front. Hum. Neurosci. 2015, 8, 1044. [Google Scholar] [CrossRef]
- Jones, T.E.; Stephenson, K.W.; King, J.G.; Knight, K.R.; Marshall, T.L.; Scott, W.B. Sarcopenia-mechanisms and treatments. J. Geriatr. Phys. Ther. 2009, 32, 83–89. [Google Scholar] [CrossRef]
- Zeki Al Hazzouri, A.; Haan, M.N.; Whitmer, R.A.; Yaffe, K.; Neuhaus, J. Central obesity, leptin and cognitive decline: The Sacramento Area Latino Study on Aging. Dement. Geriatr. Cogn. Disord. 2012, 33, 400–409. [Google Scholar] [CrossRef]
- Scalzo, P.; Kümmer, A.; Cardoso, F.; Teixeira, A.L. Serum levels of interleukin-6 are elevated in patients with Parkinson’s disease and correlate with physical performance. Neurosci. Lett. 2010, 468, 56–58. [Google Scholar] [CrossRef]
- Bian, A.L.; Hu, H.Y.; Rong, Y.D.; Wang, J.; Wang, J.X.; Zhou, X.Z. A study on relationship between elderly sarcopenia and inflammatory factors IL-6 and TNF-α. Eur. J. Med. Res. 2017, 22, 25. [Google Scholar] [CrossRef] [PubMed]
- Marsland, A.L.; Gianaros, P.J.; Kuan, D.C.; Sheu, L.K.; Krajina, K.; Manuck, S.B. Brain morphology links systemic inflammation to cognitive function in midlife adults. Brain Behav. Immun. 2015, 48, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Bagger, Y.Z.; Tankó, L.B.; Alexandersen, P.; Qin, G.; Christiansen, C. The implications of body fat mass and fat distribution for cognitive function in elderly women. Obes. Res. 2004, 12, 1519–1526. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| NC (n = 19) | PDNSa (n = 31) | PDSa (n = 21) | p | |
|---|---|---|---|---|
| Age (year) a | 60.3 ± 7.6 | 60.3 ± 9.8 | 63.7 ± 11.6 | 0.430 |
| Gender (Male) b | 10 (52.6%) | 9 (29.0%) | 12 (57.1%) | 0.088 |
| ASMI (ASM/ht2) a | 7.0 ± 1.1 | 6.5 ± 0.8 | 5.5 ± 0.7 | <0.001 * |
| BMI a | 25.0 ± 2.6 | 26.1 ± 3.1 | 21.4 ± 3.5 | <0.001 * |
| Height(cm) a | 163.0 ± 7.5 | 158.4 ± 7.0 | 160.1 ± 7.2 | 0.089 |
| MMSE a | 27.0 ± 2.3 | 26.0 ± 4.6 | 25.5 ± 4.2 | 0.519 |
| Disease duration (year) c | ― | 2.4 ± 2.4 | 1.9 ± 2.0 | 0.453 |
| UPDRS c | ||||
| I | ― | 3.4 ± 2.1 | 3.8 ± 3.0 | 0.637 |
| II | ― | 7.2 ± 4.3 | 9.9 ± 5.4 | 0.057 |
| III | ― | 17.6 ± 12.5 | 29.1 ± 12.4 | 0.002 * |
| total | ― | 28.2 ± 17.0 | 42.7 ± 17.5 | 0.005 * |
| Modified H&Y stage c | ― | 1.6 ± 1.1 | 1.6 ± 1.0 | 0.923 |
| S&E c | ― | 83.6 ± 16.8 | 83.5 ± 10.4 | 0.991 |
| LEDD c | ― | 439.3 ± 373.6 | 602.5 ± 367.8 | 0.126 |
| Treatment duration (month) c | ― | 21.9 ± 26.5 | 17.8 ± 22.7 | 0.568 |
| NC (n = 19) | PDNSa (n = 31) | PDSa (n = 21) | p | |
|---|---|---|---|---|
| Fat (g) | ||||
| Arms | 2932.1 ± 907.0 | 3742.4 ± 1457.9 △ | 2337.8 ± 802.2 △ | <0.001 |
| Legs | 6503.6 ± 1885.4 | 8303.3 ± 3236.6 △ | 5601.2 ± 1673.6 △ | 0.001 |
| Four limbs | 9435.7 ± 2638.3 * | 12,045.7 ± 4571.4 *△ | 7938.9 ± 2422.1 △ | 0.001 |
| Fat of total a (%) | ||||
| Arms | 35.7 ± 10.3 * | 43.6 ± 12.0 *△ | 36.9 ± 11.5 △ | 0.035 |
| Legs | 31.4 ± 8.4 * | 38.1 ± 10.1 * | 33.7 ± 8.5 | 0.039 |
| Four limbs | 32.6 ± 8.7 * | 39.7 ± 10.4 * | 34.6 ± 9.2 | 0.035 |
| Muscle mass (g) | ||||
| Arms | 5093.7 ± 1405.5 ◆ | 4346.0 ± 1366.4 | 3731.9 ± 984.3 ◆ | 0.006 |
| Legs | 13,644.7 ± 2937.4 ◆ | 12,817.8 ± 5261.4 | 10,350.6 ± 1848.1 ◆ | 0.028 |
| Four limbs | 18,738.4 ± 4294.7 ◆ | 17,163.8 ± 6276.4 | 14,082.5 ± 2781.8 ◆ | 0.015 |
| Muscle mass of total a (%) | ||||
| Arms | 60.6 ± 9.8 * | 51.3 ± 12.8 * | 59.2 ± 11.0 | 0.011 |
| Legs | 65.1 ± 8.3 | 58.9 ± 9.8 | 62.8 ± 8.2 | 0.056 |
| Four limbs | 63.8 ± 8.5 * | 56.6 ± 10.0 * | 61.8 ± 8.6 | 0.024 |
| Cluster | MNI Atlas coordinates | Voxel Size | WM Tract | Near Cortical Area | FA, mean ± SD | Tmax | Diffusivity Values (PDNSa−PDSa) (×10−6 mm2/s) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| x | y | z | PDNSa | PDSa | MD | AD | RD | |||||
| 1 | −5 | −89 | 14 | 353 | Left occipital WM | Left cuneus | 0.254 ± 0.048 | 0.196 ± 0.023 | 5.82 | −131.25 ** | −92.18 | −150.79 ** |
| 2 * | −47 | −7 | 45 | 394 | Left SLF | Left precentral gyrus | 0.328 ± 0.045 | 0.258 ± 0.042 | 4.81 | −131.04 ** | −70.45 | −161.34 ** |
| 3 * | −6 | 30 | −11 | 409 | Left genu of CC | Left anterior cingulate | 0.350 ± 0.024 | 0.321 ± 0.031 | 4.76 | −62.01 | −42.95 | −71.54 ** |
| 4 | 48 | −31 | 5 | 459 | Right temporal WM | Right superior temporal gyrus | 0.383 ± 0.042 | 0.346 ± 0.037 | 4.52 | −25.31 | −13.59 | −44.76 ** |
| 5 | 48 | −34 | −20 | 227 | Right temporal WM | Right fusiform gyrus | 0.245 ± 0.051 | 0.195 ± 0.036 | 4.23 | −63.53 ** | −22.84 | −83.89 ** |
| 6 | 32 | −30 | −17 | 287 | Right parahippocampal gyrus | Right parahippocampal gyrus | 0.264 ± 0.031 | 0.222 ± 0.024 | 4.19 | −40.19 ** | −9.10 | −55.73 ** |
| 7 * | 10 | −2 | 3 | 661 | Right ATR | Right thalamus | 0.520 ± 0.028 | 0.489 ± 0.028 | 4.14 | −25.84 | −3.06 | −37.24 ** |
| 8 | 6 | −26 | 36 | 594 | Right cingulum | Right cingulate gyrus | 0.373 ± 0.031 | 0.347 ± 0.042 | 4.06 | −34.91 ** | −18.61 | −43.05 ** |
| 9 | 4 | 26 | −12 | 240 | Right anterior cingulate | Right anterior cingulate | 0.268 ± 0.034 | 0.219 ± 0.041 | 4.01 | −37.89 | −2.19 | −57.93 |
| 10 * | −7 | −39 | 31 | 429 | Left cingulum | Left cingulate gyrus | 0.373 ± 0.026 | 0.348 ± 0.020 | 3.96 | −24.30 ** | −3.12 | −34.89 ** |
| 11 | −32 | −10 | 22 | 271 | Left SLF | Left insula | 0.459 ± 0.026 | 0.424 ± 0.033 | 3.67 | −29.46 | −4.67 | −41.86 ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-Y.; Chen, H.-L.; Chen, P.-C.; Chen, Y.-S.; Chiang, P.-L.; Wang, C.-K.; Lu, C.-H.; Chen, M.-H.; Chou, K.-H.; Huang, Y.-C.; et al. Correlation between Executive Network Integrity and Sarcopenia in Patients with Parkinson’s Disease. Int. J. Environ. Res. Public Health 2019, 16, 4884. https://doi.org/10.3390/ijerph16244884
Lee C-Y, Chen H-L, Chen P-C, Chen Y-S, Chiang P-L, Wang C-K, Lu C-H, Chen M-H, Chou K-H, Huang Y-C, et al. Correlation between Executive Network Integrity and Sarcopenia in Patients with Parkinson’s Disease. International Journal of Environmental Research and Public Health. 2019; 16(24):4884. https://doi.org/10.3390/ijerph16244884
Chicago/Turabian StyleLee, Chih-Ying, Hsiu-Ling Chen, Pei-Chin Chen, Yueh-Sheng Chen, Pi-Ling Chiang, Cheng-Kang Wang, Cheng-Hsien Lu, Meng-Hsiang Chen, Kun-Hsien Chou, Yu-Chi Huang, and et al. 2019. "Correlation between Executive Network Integrity and Sarcopenia in Patients with Parkinson’s Disease" International Journal of Environmental Research and Public Health 16, no. 24: 4884. https://doi.org/10.3390/ijerph16244884
APA StyleLee, C.-Y., Chen, H.-L., Chen, P.-C., Chen, Y.-S., Chiang, P.-L., Wang, C.-K., Lu, C.-H., Chen, M.-H., Chou, K.-H., Huang, Y.-C., & Lin, W.-C. (2019). Correlation between Executive Network Integrity and Sarcopenia in Patients with Parkinson’s Disease. International Journal of Environmental Research and Public Health, 16(24), 4884. https://doi.org/10.3390/ijerph16244884