Prevalence of Human Papillomavirus (HPV) and Other Sexually Transmitted Infections (STIs) among Italian Women Referred for a Colposcopy

 , ,
, , 
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Collection
2.2. DNA Extraction, HPV and STI Detection
2.3. Statistical Analysis
3. Results
3.1. Study Population
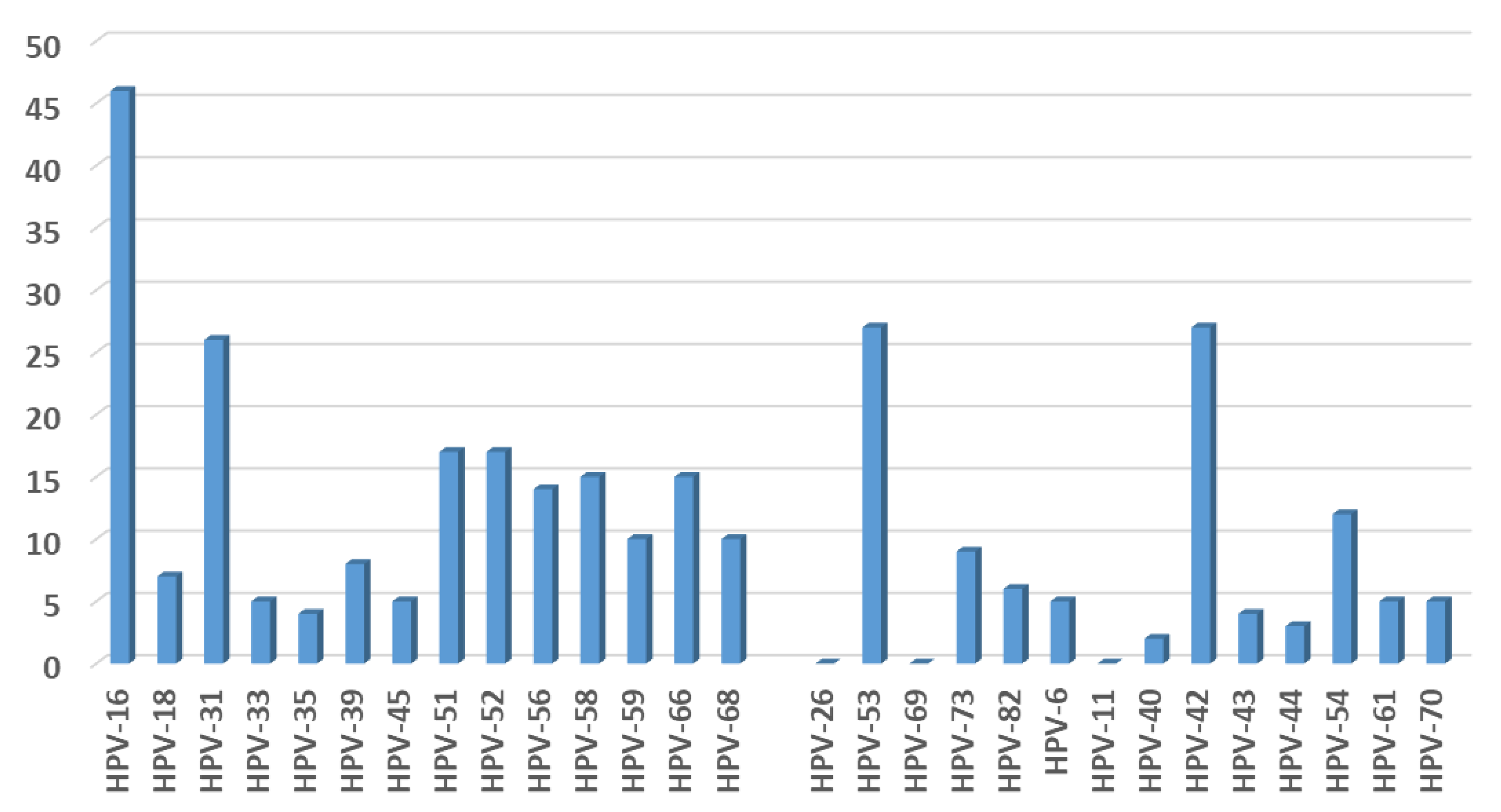
3.2. HPV Detection and Typing
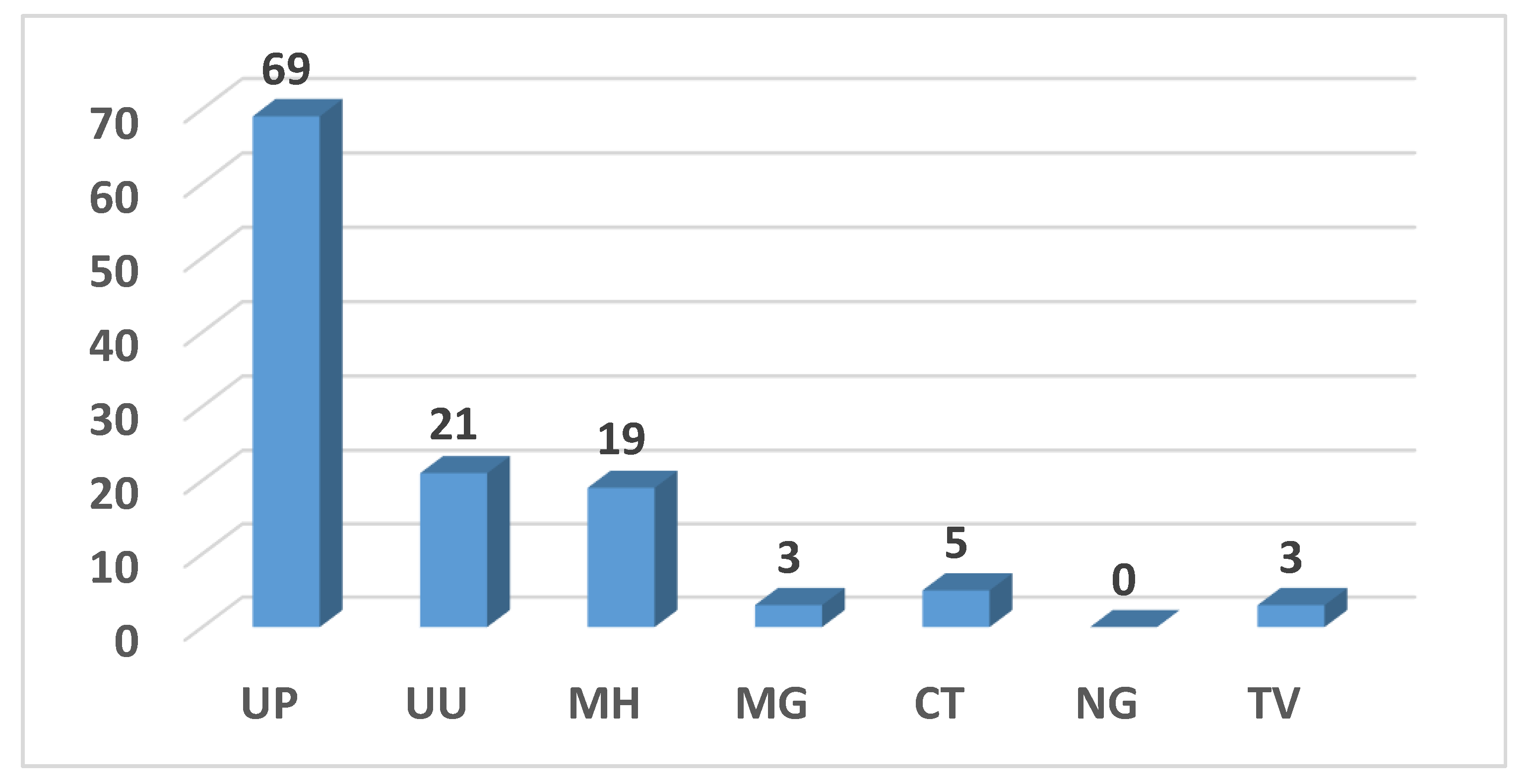
3.3. STI Prevalence
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| STDs | sexually transmitted disease |
| HPV | Human Papillomavirus |
| HSIL | High grade squamous intraepithelial lesion |
| ASCH | Atypical squamous cells-cannot exclude HSIL |
| LSIL | Low-grade squamous intraepithelial lesion |
| AGCUS | Atypical Glandular Cells of undetermined significance |
| ASCUS | Atypical squamous cells of undetermined significance |
| NILM | Negative for Intraepithelial Lesion or Malignancy |
| CIN1 | cervical intraepithelial neoplasia grade 1 |
| CIN2 | cervical intraepithelial neoplasia grade 2 |
| CIN3 | cervical intraepithelial neoplasia grade 3 |
| Ng | Neisseria gonorrhoeae |
| Tv | Trichomonas vaginalis |
| Mh | Mycoplasma hominis |
| Mg | Mycoplasma genitalium |
| Uu | Ureaplasma urealyticum |
| Up | Ureaplasma parvum |
| Ct | Chlamydia trachomatis |
| PCR | polymerase chain reaction |
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar]
- International Agency for Research on Cancer. A review of human carcinogens: Biological agents. IARC Monogr. Eval. Carcinog. Risks Hum. 2009, 10, 321–322. [Google Scholar]
- Walboomers, J.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Burd, E.M. Human papillomavirus and cervical cancer. Clin. Microbiol. Rev. 2003, 16, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavanagh, K.; Pollock, K.G.; Potts, A.; Love, J.; Cuschieri, K.; Cubie, H.; Robertson, C.; Donaghy, M. Introduction and sustained high coverage of the HPV bivalent vaccine leads to a reduction in prevalence of HPV 16/18 and closely related HPV types. Br. J. Cancer 2014, 110, 2804–2811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tota, J.E.; Ramanakumar, A.V.; Jiang, M.; Dillner, J.; Walter, S.D.; Kaufman, J.S.; Coutlée, F.; Villa, L.L.; Franco, E.L. Epidemiologic approaches to evaluating the potential for human papillomavirus type replacement postvaccination. Am. J. Epidemiol. 2013, 178, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Man, I.; Auranen, K.; Wallinga, J.; Bogaards, J.A. Capturing multiple-type interactions into practical predictors of type replacement following human papillomavirus vaccination. Philos. Trans. R Soc. Lond. B Biol. Sci. 2019, 374, 20180298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, H.; Shen, Z.; Luo, H.; Zhang, W.; Zhu, X. Chlamydia Trachomatis Infection-Associated Risk of Cervical Cancer: A Meta-Analysis. Medicine 2016, 95, e3077. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhu, L.; Li, H.; Ma, N.; Huang, H.; Zhang, X.; Li, Y.; Fang, J. Association between asymptomatic sexually transmitted infections and high-risk human papillomavirus in cervical lesions. J. Int. Med. Res. 2019, 47, 5548–5589. [Google Scholar] [CrossRef] [PubMed]
- Mancini, F.; Vescio, F.; Mochi, S.; Accardi, L.; di Bonito, P.; Ciervo, A. HPV and Chlamydia trachomatis coinfection in women with Pap smear abnormality: Baseline data of the HPV Pathogen ISS study. Infez. Med. 2018, 26, 139–144. [Google Scholar]
- Castle, P.E.; Giuliano, A.R. Chapter 4: Genital tract infections, cervical inflammation, and antioxidant nutrients–assessing their roles as human papillomavirus cofactors. J. Natl. Cancer Inst. Monogr. 2003, 31, 29–34. [Google Scholar] [CrossRef]
- Roeters, A.M.; Boon, M.E.; van Haaften, M.; Vernooij, F.; Bontekoe, T.R.; Heintz, A.P. Inflammatory events as detected in cervical smears and squamous intraepithelial lesions. Diagn. Cytopathol. 2010, 38, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.H. Bethesda 2001—Review. Cytopathology 2002, 13, 4–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baasland, I.; Romundstad, P.R.; Eide, M.L.; Jonassen, C.M. Clinical performance of Anyplex II HPV28 by human papillomavirus type and viral load in a referral population. PLoS ONE 2019, 14, e0210997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, M.; Musumeci, R.; Rizzo, A.; Muresu, N.; Piana, A.; Sotgiu, G.; Landoni, F.; Cocuzza, C. Prevalence of Chlamydia trachomatis Infection, Serovar Distribution and Co-Infections with Seven High-Risk HPV Types among Italian Women with a Recent History of Abnormal Cervical Cytology. Int. J. Environ. Res. Public Health 2019, 16, 3354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocuzza, C.E.; Martinelli, M.; Sina, F.; Piana, A.; Sotgiu, G.; Dell’Anna, T.; Musumeci, R. Human papillomavirus DNA detection in plasma and cervical samples of women with a recent history of low grade or precancerous cervical dysplasia. PLoS ONE 2017, 12, e0188592. [Google Scholar] [CrossRef] [PubMed]
- Tewari, P.; White, C.; Kelly, L.; Pilkington, L.; Keegan, H.; D’Arcy, T.; Toole, S.O.; Sharp, L.; O’Leary, J.J.; Martin, C.M. Clinical performance of the Cobas 4800 HPV test and the Aptima HPV assay in the management of women referred to colposcopy with minor cytological abnormalities. Diagn. Cytopathol. 2018, 46, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Piana, A.; Sotgiu, G.; Cocuzza, C.; Musumeci, R.; Marras, V.; Pischedda, S.; Deidda, S.; Muresu, E.; Castiglia, P. High HPV-51 prevalence in invasive cervical cancers: Results of a pre-immunization survey in North Sardinia, Italy. PLoS ONE 2013, 8, e63395. [Google Scholar] [CrossRef]
- Orlando, G.; Fasolo, M.; Mazza, F.; Ricci, E.; Esposito, S.; Frati, E.; Zuccotti, G.V.; Cetin, I.; Gramegna, M.; Rizzardini, G.; et al. Valhidate Study Group. Risk of cervical HPV infection and prevalence of vaccine-type and other high-risk HPV types among sexually active teens and young women (13–26 years) enrolled in the VALHIDATE study. Hum. Vaccines Immunother. 2014, 10, 986–994. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, S.; Frati, E.R.; Panatto, D.; Martinelli, M.; Amicizia, D.; Zotti, C.M.; Martinese, M.; Bonanni, P.; Boccalini, S.; Coppola, R.C.; et al. Detection and genotyping of human papillomavirus in urine samples from unvaccinated male and female adolescents in Italy. PLoS ONE 2013, 8, e79719. [Google Scholar] [CrossRef]
- Frati, E.R.; Martinelli, M.; Fasoli, E.; Colzani, D.; Bianchi, S.; Binda, S.; Olivani, P.; Tanzi, E. HPV Testing from Dried Urine Spots as a Tool for Cervical Cancer Screening in Low-Income Countries. BioMed Res. Int. 2015, 2015, 1–5. [Google Scholar] [CrossRef]
- Del Prete, R.; Ronga, L.; Lestingi, M.; Addati, G.; Angelotti, U.F.; Di Carlo, D.; Miragliotta, G. Simultaneous detection and identification of STI pathogens by multiplex Real-Time PCR in genital tract specimens in a selected area of Apulia, a region of Southern Italy. Infection 2017, 45, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, T.; Matsumoto, M.; Matsuo, J.; Abe, K.; Minami, K.; Yamaguchi, H. Frequency of Chlamydia trachomatis in Ureaplasma-positive healthy women attending their first prenatal visit in a community hospital in Sapporo, Japan. BMC Infect. Dis. 2012, 12, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foschi, C.; Nardini, P.; Banzola, N.; D’Antuono, A.; Compri, M.; Cevenini, R.; Marangoni, A. Chlamydia trachomatis infection prevalence and serovar distribution in a high-density urban area in the north of Italy. J. Med. Microbiol. 2016, 65, 510–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salfa, M.C.; Suligoi, B.; Italian STI Laboratory-based Surveillance Working Group. Prevalence of Chlamydia trachomatis, Trichomonas vaginalis and Neisseria gonorrhoeae Based on Data Collected by a Network of Clinical Microbiology Laboratories, in Italy. Adv. Exp. Med. Biol. 2016, 901, 47–57. [Google Scholar] [PubMed]
- Bianchi, S.; Boveri, S.; Igidbashian, S.; Amendola, A.; Urbinati, A.M.; Frati, E.R.; Bottari, F.; Colzani, D.; Landoni, F.; Tanzi, E.; et al. Chlamydia trachomatis infection and HPV/Chlamydia trachomatis co-infection among HPV-vaccinated young women at the beginning of their sexual activity. Arch. Gynecol. Obstet. 2016, 294, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Frati, E.R.; Fasoli, E.; Martinelli, M.; Colzani, D.; Bianchi, S.; Carnelli, L.; Amendola, A.; Olivani, P.; Tanzi, E. Sexually Transmitted Infections: A Novel Screening Strategy for Improving Women’s Health in Vulnerable Populations. Int. J. Mol. Sci. 2017, 18, 1311. [Google Scholar] [CrossRef] [Green Version]
- Marovt, M.; Kese, D.; Kotar, T.; Kmet, N.; Miljkovic, J.; Soba, B.; Maticic, M. Ureaplasma parvum and Ureaplasma urealyticum detected with the same frequency among women with and without symptoms of urogenital tract infection. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1237–1245. [Google Scholar] [CrossRef]
- Leli, C.; Mencacci, A.; Latino, M.A.; Clerici, P.; Rassu, M.; Perito, S.; Castronari, R.; Pistoni, E.; Luciano, E.; De Maria, D.; et al. Prevalence of cervical colonization by Ureaplasma parvum, Ureaplasma urealyticum, Mycoplasma hominis and Mycoplasma genitalium in childbearing aged women by a commercially available multiplex real-time PCR: An Italian observational multicentre study. J. Microbiol. Immunol. Infect. 2018, 51, 220–225. [Google Scholar] [CrossRef]
- Horner, P.; Donders, G.; Cusini, M.; Gomberg, M.; Jensen, J.S.; Unemo, M. Should we be testing for urogenital Mycoplasma hominis, Ureaplasma parvum and Ureaplasma urealyticum in men and women?—A position statement from the European STI Guidelines Editorial Board. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1845–1851. [Google Scholar] [CrossRef] [Green Version]
- Lukic, A.; Canzio, C.; Patella, A.; Giovagnoli, M.; Cipriani, P.; Frega, A.; Moscarini, M. Determination of cervicovaginal microorganisms in women with abnormal cervical cytology: The role of Ureaplasma urealyticum. Anticancer Res. 2006, 26, 4843–4849. [Google Scholar]
- Parthenis, C.; Panagopoulos, P.; Margari, N.; Kottaridi, C.; Spathis, A.; Pouliakis, A.; Konstantoudakis, S.; Chrelias, G.; Chrelias, C.; Papantoniou, N.; et al. The association between sexually transmitted infections, human papillomavirus, and cervical cytology abnormalities among women in Greece. Int. J. Infect. Dis. 2018, 73, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Biernat-Sudolska, M.; Szostek, S.; Rojek-Zakrzewska, D.; Klimek, M.; Kosz-Vnenchak, M. Concomitant infections with human papillomavirus and various mycoplasma and ureaplasma species in women with abnormal cervical cytology. Adv. Med. Sci. 2011, 56, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Li, T.; Chen, L.; Zhang, X.; Zhao, G.; Liu, Z. Epidemiological investigation of the relationship between common lower genital tract infections and high-risk human papillomavirus infections among women in Beijing, China. PLoS ONE 2017, 12, e0178033. [Google Scholar] [CrossRef] [PubMed]
- Amorim, A.T.; Marques, L.M.; Campos, G.B.; Lobão, T.N.; de Souza Lino, V.; Cintra, R.C.; Andreoli, M.A.; Villa, L.L.; Boccardo, E.; Braga, A.C.R., Jr.; et al. Co-infection of sexually transmitted pathogens and Human Papillomavirus in cervical samples of women of Brazil. BMC Infect. Dis. 2017, 17, 769. [Google Scholar] [CrossRef]
- Mendoza, L.; Mongelos, P.; Paez, M.; Castro, A.; Rodriguez-Riveros, I.; Gimenez, G.; Araujo, P.; Echagüe, G.; Diaz, V.; Laspina, F.; et al. Human papillomavirus and other genital infections in indigenous women from Paraguay: A cross-sectional analytical study. BMC Infect. Dis. 2013, 13, 531. [Google Scholar] [CrossRef] [Green Version]
- Ye, H.; Song, T.; Zeng, X.; Li, L.; Hou, M.; Xi, M. Association between genital mycoplasmas infection and human papillomavirus infection, abnormal cervical cytopathology, and cervical cancer: A systematic review and meta‑analysis. Arch. Gynecol. Obstet. 2018, 297, 1377–1387. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytology | n | % |
|---|---|---|
| HSIL | 25 | 14.1% |
| ASCH | 14 | 7.9% |
| LSIL | 76 | 42.9% |
| AGCUS | 9 | 5.1% |
| ASCUS | 43 | 24.3% |
| NILM | 10 | 5.6% |
| Total | 177 |
| Women with Available Colposcopy Result (n = 175) | Positive Colposcopy n (%) | Negative Colposcopy n (%) | p-Value * |
|---|---|---|---|
| Single HPV 16 (n = 22) | 15 (34.0%) | 7 (5.3%) | <0.0001 |
| Single HPV 18 (n = 1) | 1 (2.3%) | 0 (0.0%) | 0.31 |
| HPV 16 + other hrHPV (n = 24) | 5 (11.4%) | 19 (14.5%) | 0.59 |
| HPV 18 + other hrHPV (n = 6) | 2 (4.6%) | 4 (3.1%) | 0.67 |
| Single other hrHPV (n = 39) | 10 (22.7%) | 29 (22.1%) | 0.93 |
| Multiple other hrHPV (n = 23) | 6 (13.6%) | 17 (13.0%) | 0.92 |
| hrHPV Negative (n = 60) | 5 (11.4%) | 55 (42.0%) | <0.0001 |
| 44 (25.1%) | 131 (74.9%) |
| Women with Available Colposcopy Result (n = 175) | Positive Colposcopy n. (%) | Negative Colposcopy n. (%) | p-Valhue * |
|---|---|---|---|
| Single STI (n = 64) | 18 (40.1%) | 46 (35.1%) | 0.56 |
| Multiple STI (n = 23) | 6 (13.6%) | 17 (13.0%) | 0.92 |
| Negative (n = 88) | 20 (45.5%) | 68 (51.9%) | 0.46 |
| hrHPV positive women infected also with (n = 114): | |||
| Up (n = 37) | 12 (30.8%) | 25 (33.3%) | 0.79 |
| Uu (n = 6) | 4 (10.3%) | 2 (2.7%) | 0.09 |
| Mh (n = 2) | 0 (0.0%) | 2 (2.7%) | 0.30 |
| Mg (n = 0) | 0 (0.0%) | 0 (0.0%) | - |
| Ct (n = 0) | 0 (0.0%) | 0 (0.0%) | - |
| Ng (n = 0) | 0 (0.0%) | 0 (0.0%) | - |
| Tv (n = 0) | 0 (0.0%) | 0 (0.0%) | - |
| Multiple STIs (n = 20) | 6 (15.4%) | 14 (18.7%) | 0.66 |
| Negative (n = 49) | 17 (43.6%) | 32 (42.7%) | 0.93 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinelli, M.; Musumeci, R.; Sechi, I.; Sotgiu, G.; Piana, A.; Perdoni, F.; Sina, F.; Fruscio, R.; Landoni, F.; Cocuzza, C.E. Prevalence of Human Papillomavirus (HPV) and Other Sexually Transmitted Infections (STIs) among Italian Women Referred for a Colposcopy. Int. J. Environ. Res. Public Health 2019, 16, 5000. https://doi.org/10.3390/ijerph16245000
Martinelli M, Musumeci R, Sechi I, Sotgiu G, Piana A, Perdoni F, Sina F, Fruscio R, Landoni F, Cocuzza CE. Prevalence of Human Papillomavirus (HPV) and Other Sexually Transmitted Infections (STIs) among Italian Women Referred for a Colposcopy. International Journal of Environmental Research and Public Health. 2019; 16(24):5000. https://doi.org/10.3390/ijerph16245000
Chicago/Turabian StyleMartinelli, Marianna, Rosario Musumeci, Illari Sechi, Giovanni Sotgiu, Andrea Piana, Federica Perdoni, Federica Sina, Robert Fruscio, Fabio Landoni, and Clementina E. Cocuzza. 2019. "Prevalence of Human Papillomavirus (HPV) and Other Sexually Transmitted Infections (STIs) among Italian Women Referred for a Colposcopy" International Journal of Environmental Research and Public Health 16, no. 24: 5000. https://doi.org/10.3390/ijerph16245000
APA StyleMartinelli, M., Musumeci, R., Sechi, I., Sotgiu, G., Piana, A., Perdoni, F., Sina, F., Fruscio, R., Landoni, F., & Cocuzza, C. E. (2019). Prevalence of Human Papillomavirus (HPV) and Other Sexually Transmitted Infections (STIs) among Italian Women Referred for a Colposcopy. International Journal of Environmental Research and Public Health, 16(24), 5000. https://doi.org/10.3390/ijerph16245000