Neurocognitive Mechanism of Human Resilience: A Conceptual Framework and Empirical Review


Abstract
:1. Introduction
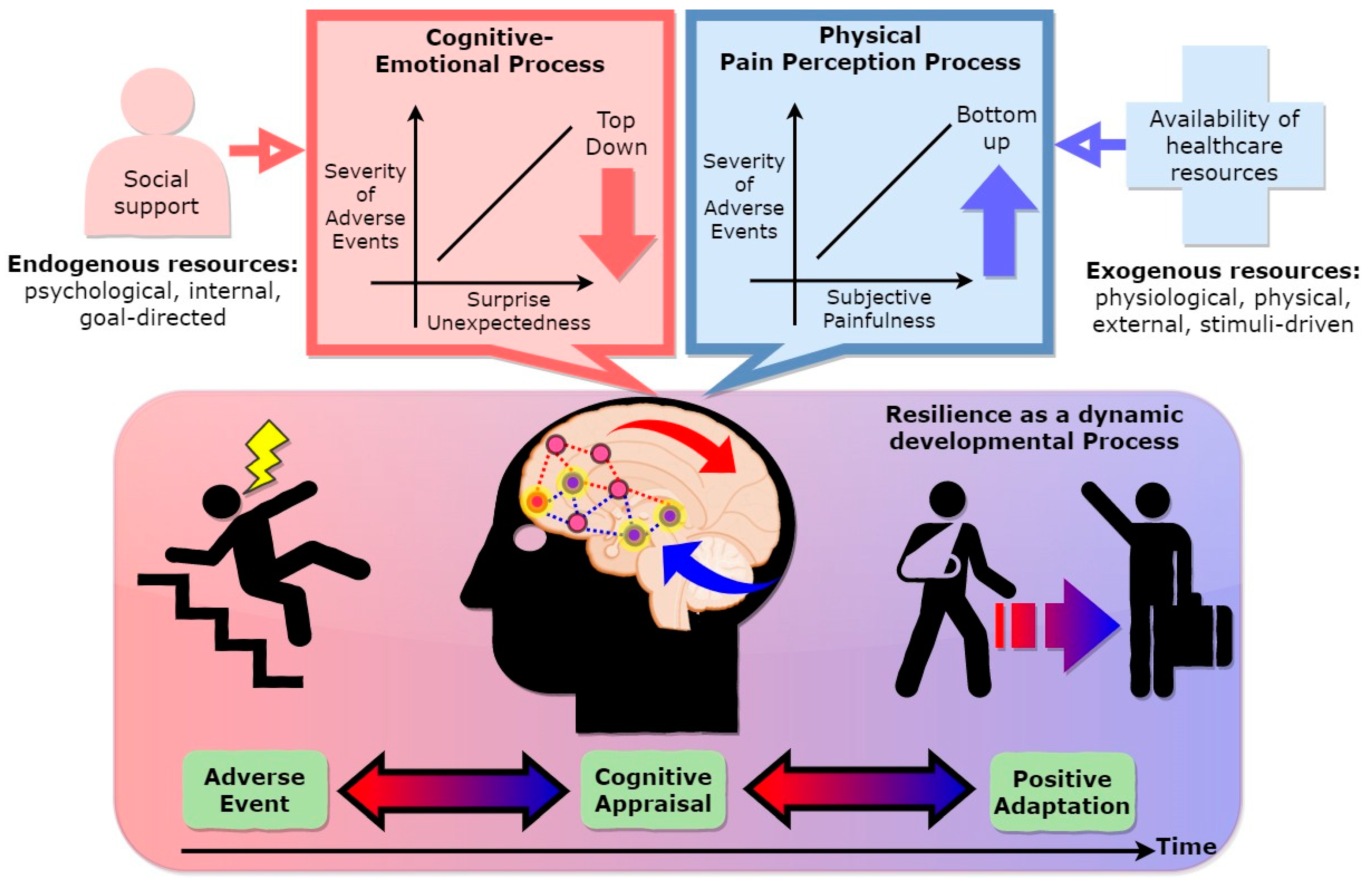
2. Resilience as a Dynamic Developmental Process
3. Cognitive Appraisal of Adversity
3.1. The Perspective of Stressor Perception
3.2. Stressor Severity: The Importance of Cognitive–Emotional Process and Perception of Pain
3.3. The Role of Cognitive Appraisal in Cognitive–Emotional Processes
3.4. Cognition–Emotion–Perception Processes Connect Cognitive Appraisal
4. The Role of the Prefrontal Cortex in Cognitive Control, Emotional Regulation, and Pain Perception
5. Linking the Malleable Brain, Resilient Mind, and Adaptive Behavior: The Role of Cognitive Flexibility in Cognitive Control, Emotional Regulation, and Pain Perception
6. Future Perspectives and Concluding Remarks
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burns, D.L.; Catlin, A.J. Positive Toxicology Screening in Newborns: Ethical Issues in the Decision to Legally Intervene. Pediatric Nurs. 2017, 23, 73–80. [Google Scholar]
- Mureşan, L.; Georgescu, A. The Road to Resilience in 2050: Critical space infrastructure and space security. RUSI J. 2015, 160, 58–66. [Google Scholar] [CrossRef]
- Southwick, S.M.; Charney, D.S. THE science of resilience: Implications for the prevention and treatment of depression. Science 2012, 338, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Kalisch, R.; Baker, D.G.; Basten, U.; Boks, M.P.; Bonanno, G.A.; Brummelman, E.; Chmitorz, A.; Fernàndez, G.; Fiebach, C.J.; Galatzer-Levy, I.; et al. The resilience framework as a strategy to combat stress-related disorders. Nat. Hum. Behav. 2017, 1, 784–790. [Google Scholar] [CrossRef] [Green Version]
- Southwick, S.M.; Bonanno, G.A.; Masten, A.S.; Panter-Brick, C.; Yehuda, R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatol. 2014, 5, 25338. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, D.; Sarkar, M. Psychological resilience: A review and critique of definitions, concepts, and theory. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Windle, G. What is resilience? A review and concept analysis. Rev. Clin. Gerontol. 2011, 21, 152–169. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Leipold, B.; Greve, W. A conceptual bridge between coping and development. Eur. Psychol. 2009, 14, 40–50. [Google Scholar] [CrossRef]
- Cicchetti, D. Resilience under conditions of extreme stress: A multilevel perspective. World Psychiatry 2010, 9, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Masten, A.S. Ordinary magic: Resilience processes in development. Am. Psychol. 2001, 56, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Mancini, A.D.; Bonanno, G.A. Predictors and parameters of resilience to loss: Toward an individual differences model. J. Pers. 2009, 77, 1805–1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lock, S.; Rees, C.S.; Heritage, B. Development and validation of a brief measure of psychological resilience: The state—Trait assessment of resilience scale. Aust. Psychol. 2019. [Google Scholar] [CrossRef]
- Van der Meer, C.A.I.; te Brake, H.; van der Aa, N.; Dashtgard, P.; Bakker, A.; Olff, M. Assessing psychological resilience: Development and psychometric properties of the english and dutch version of the Resilience Evaluation Scale (RES). Front. Psychiatry 2018, 9, 169. [Google Scholar] [CrossRef] [PubMed]
- Windle, G.; Bennett, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doukas, A.M.; D’Andrea, W.M.; Gregory, W.E.; Joachim, B.; Lee, K.A.; Robinson, G.; Freed, S.J.; Khedari-DePierro, V.; Pfeffer, K.A.; Todman, M.; et al. Hurts so good: Pain as an emotion regulation strategy. Emotion 2019. [Google Scholar] [CrossRef]
- Eysenck, M.W.; Derakshan, N.; Santos, R.; Calvo, M.G. Anxiety and cognitive performance: Attentional control theory. Emotion 2007, 7, 336–353. [Google Scholar] [CrossRef] [Green Version]
- Blascovich, J.; Elliot, A.J. Challenge and threat. In Handbook of Approach and Avoidance Motivation; Psychology Press: New York, NY, USA, 2008; pp. 431–445. [Google Scholar]
- Major, B.; Richards, C.; Cozzarelli, C.; Cooper, M.L.; Zubek, J. Personal resilience, cognitive appraisals, and coping: An integrative model of adjustment to abortion. J. Pers. Soc. Psychol. 1998, 74, 735–752. [Google Scholar] [CrossRef]
- Vanderbilt-Adriance, E.; Shaw, D.S. Protective factors and the development of resilience in the context of neighborhood disadvantage. J. Abnorm. Child Psychol. 2008, 36, 887–901. [Google Scholar] [CrossRef] [Green Version]
- Bubic, A.; Von Cramon, D.Y.; Schubotz, R.I. Prediction, cognition and the brain. Front. Hum. Neurosci. 2010, 4, 25. [Google Scholar] [CrossRef] [Green Version]
- Friston, K. The free-energy principle: A unified brain theory? Nat. Rev. Neurosci. 2010, 11, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Koyama, T.; McHaffie, J.G.; Laurienti, P.J.; Coghill, R.C. The subjective experience of pain: Where expectations become reality. Proc. Natl. Acad. Sci. USA 2005, 102, 12950–12955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mellers, B.; Fincher, K.; Drummond, C.; Bigony, M. Surprise. A belief or an emotion? In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2013; Volume 202, pp. 3–19. [Google Scholar]
- Den Ouden, H.E.M.; Kok, P.; de Lange, F.P. How prediction errors shape perception, attention, and motivation. Front. Psychol. 2012, 3, 548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherrer, M.V. The role of cognitive appraisal in adaptation to traumatic stress in adults with serious mental illness: A critical review. Trauma Violence Abus. 2011, 12, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Transactional theory and research on emotions and coping. Eur. J. Pers. 1987, 1, 141–169. [Google Scholar] [CrossRef]
- Lazarus, R.S. Progress on a cognitive-motivational-relational theory of emotion. Am. Psychol. 1991, 46, 819–834. [Google Scholar] [CrossRef]
- Roseman, I.J. Appraisal determinants of emotions: Constructing a more accurate and comprehensive theory. Cogn. Emot. 1996, 10, 241–278. [Google Scholar] [CrossRef]
- Parsons, S.; Kruijt, A.-W.; Fox, E. A Cognitive model of psychological resilience. J. Exp. Psychopathol. 2016, 7, 296–310. [Google Scholar] [CrossRef] [Green Version]
- Kalisch, R.; Müller, M.B.; Tüscher, O. A conceptual framework for the neurobiological study of resilience. Behav. Brain Sci. 2015, 38, e92. [Google Scholar] [CrossRef]
- Clark, A. A nice surprise? Predictive processing and the active pursuit of novelty. Phenomenol. Cogn. Sci. 2018, 17, 521–534. [Google Scholar] [CrossRef] [Green Version]
- Clark, A. Whatever next? Predictive brains, situated agents, and the future of cognitive science. Behav. Brain Sci. 2013, 36, 181–204. [Google Scholar] [CrossRef] [PubMed]
- Ochsner, K.N.; Ray, R.R.; Hughes, B.; Mcrae, K.; Cooper, J.C.; Weber, J.; Gabrieli, J.D.E.; Gross, J.J. Bottom-up and top-down processes in emotion generation: Common and distinct neural mechanisms. Psychol. Sci. 2009, 20, 1322–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schubotz, R.I. Prediction and expectation. In Brain Mapping: An Encyclopedic Reference; Arthur, W., Toga, A.W., Eds.; Elsevier: Amsterdam, The Netherlands, 2015; Volume 3, pp. 295–302. [Google Scholar] [CrossRef]
- Sturgeon, J.A.; Zautra, A.J. Social pain and physical pain: Shared paths to resilience. Pain Manag. 2016, 6, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Meerwijk, E.L.; Ford, J.M.; Weiss, S.J. Brain regions associated with psychological pain: Implications for a neural network and its relationship to physical pain. Brain Imaging Behav. 2013, 7, 1–14. [Google Scholar] [CrossRef]
- Kross, E.; Berman, M.G.; Mischel, W.; Smith, E.E.; Wager, T.D. Social rejection shares somatosensory representations with physical pain. Proc. Natl. Acad. Sci. USA 2011, 108, 6270–6275. [Google Scholar] [CrossRef] [Green Version]
- Eisenberger, N.I.; Lieberman, M.D. Why rejection hurts: A common neural alarm system for physical and social pain. Trends Cogn. Sci. 2004, 8, 294–300. [Google Scholar] [CrossRef]
- Lumley, M.A.; Cohen, J.L.; Borszcz, G.S.; Cano, A.; Radcliffe, A.M.; Porter, L.S.; Schubiner, H.; Keefe, F.J. Pain and emotion: A biopsychosocial review of recent research. J. Clin. Psychol. 2011, 67, 942–968. [Google Scholar] [CrossRef] [Green Version]
- Wiech, K. Deconstructing the sensation of pain: The influence of cognitive processes on pain perception. Science 2016, 354, 584–587. [Google Scholar] [CrossRef]
- Roseman, I.J.; Evdokas, A. Appraisals cause experienced emotions: Experimental evidence. Cogn. Emot. 2004, 18, 1–28. [Google Scholar] [CrossRef]
- Bushnell, M.C.; Čeko, M.; Low, L.A. Cognitive and emotional control of pain and its disruption in chronic pain. Nat. Rev. Neurosci. 2013, 14, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Southwick, S.M.; Litz, B.T.; Charney, D.; Friedman, M.J. Resilience and Mental Health: Challenges across the Lifespan; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar] [CrossRef] [Green Version]
- Feder, A.; Nestler, E.J.; Charney, D.S. Psychobiology and molecular genetics of resilience. Nat. Rev. Neurosci. 2009, 10, 446–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tugade, M.M.; Fredrickson, B.L. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J. Pers. Soc. Psychol. 2004, 86, 320–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denson, T.F.; Spanovic, M.; Miller, N. Cognitive appraisals and emotions predict cortisol and immune responses: A meta-analysis of acute laboratory social stressors and emotion inductions. Psychol. Bull. 2009, 135, 823–853. [Google Scholar] [CrossRef] [PubMed]
- Leterme, P.; Pirard, L.; Théwis, A. A note on the comparison of methods for estimating the ileal digestibility of amino acids in pigs. Anim. Prod. 1991, 52, 404–406. [Google Scholar] [CrossRef]
- Kay, S.A. Emotion regulation and resilience: Overlooked connections. Ind. Organ. Psychol. 2016, 9, 411–415. [Google Scholar] [CrossRef]
- Brummer, L.; Stopa, L.; Bucks, R. The influence of age on emotion regulation strategies and psychological distress. Behav. Cogn. Psychother. 2014, 42, 668–681. [Google Scholar] [CrossRef] [PubMed]
- Brümmer, L. Ageing and Emotion Regulation. Ph.D. Thesis, University of Southhampton, Southampton, UK, 2009. [Google Scholar]
- Verduyn, P.; Van Mechelen, I.; Tuerlinckx, F. The relation between event processing and the duration of emotional experience. Emotion 2011, 11, 20–28. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.A.; Lambert, H.K. Child trauma exposure and psychopathology: Mechanisms of risk and resilience. Curr. Opin. Psychol. 2017, 14, 29–34. [Google Scholar] [CrossRef]
- Infurna, F.J.; Luthar, S.S. Resilience to major life stressors is not as common as thought. Perspect. Psychol. Sci. 2016, 11, 175–194. [Google Scholar] [CrossRef]
- Richardson, G.E.; Neiger, B.L.; Jensen, S.; Kumpfer, K.L. The resiliency model. Health Educ. 1990, 21, 33–39. [Google Scholar] [CrossRef]
- Sandal, G.M.; Manzey, D.; Smith, N.; Landon, L.B.; Barrett, J.D. Psychological resilience. Space Saf. Hum. Perform. 2017, 18, 183–237. [Google Scholar] [CrossRef]
- Agaibi, C.E.; Wilson, J.P. Trauma, PTSD and resilience: A review of the literature. Trauma Violence Abus. 2005, 6, 195–216. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Sills, L.; Cohan, S.L.; Stein, M.B. Relationship of resilience to personality, coping, and psychiatric symptoms in young adults. Behav. Res. Ther. 2006, 44, 585–599. [Google Scholar] [CrossRef] [PubMed]
- Abrahams, N.; Mathews, S.; Martin, L.J.; Lombard, C.; Jewkes, R. Intimate partner femicide in South Africa in 1999 and 2009. PLoS Med. 2013, 10, e1001412. [Google Scholar] [CrossRef] [PubMed]
- Galli, N.; Vealey, R.S. “Bouncing Back” from adversity: Athletes’ experiences of resilience. Sport Psychol. 2016, 22, 316–335. [Google Scholar] [CrossRef]
- Richardson, G.E. The metatheory of resilience and resiliency. J. Clin. Psychol. 2002, 58, 307–321. [Google Scholar] [CrossRef]
- Rutter, M. Implications of resilience concepts for scientific understanding. Ann. N. Y. Acad. Sci. 2006, 1094, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Montpetit, M.A.; Bergeman, C.S.; Deboeck, P.R.; Tiberio, S.S.; Boker, S.M. Resilience-as-process: Negative affect, stress, and coupled dynamical systems. Psychol. Aging 2010, 25, 631–640. [Google Scholar] [CrossRef]
- Kong, F.; Wang, X.; Hu, S.; Liu, J. Neural correlates of psychological resilience and their relation to life satisfaction in a sample of healthy young adults. Neuroimage 2015, 123, 165–172. [Google Scholar] [CrossRef]
- Walker, F.R.; Pfingst, K.; Carnevali, L.; Sgoifo, A.; Nalivaiko, E. In the search for integrative biomarker of resilience to psychological stress. Neurosci. Biobehav. Rev. 2017, 74, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, A.; Kotozaki, Y.; Sugiura, M.; Nouchi, R.; Takeuchi, H.; Hanawa, S.; Nakagawa, S.; Miyauchi, C.M.; Araki, T.; Sakuma, A.; et al. Resilience after 3/11: Structural brain changes 1 year after the Japanese earthquake. Mol. Psychiatry 2015, 20, 552–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feder, A.; Charney, D.; Collins, K. Neurobiology of resilience. Resil. Ment. Health Chall. Across Lifesp. 2011, 15, 1–29. [Google Scholar] [CrossRef]
- Bressler, S.L.; Menon, V. Large-scale brain networks in cognition: Emerging methods and principles. Trends Cogn. Sci. 2010, 14, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Friston, K. Structural and functional brain networks: From connections to cognition. Science 2013, 342, 1238411. [Google Scholar] [CrossRef] [Green Version]
- Siettos, C.; Starke, J. Multiscale modeling of brain dynamics: From single neurons and networks to mathematical tools. Wiley Interdiscip. Rev. Syst. Biol. Med. 2016, 8, 438–458. [Google Scholar] [CrossRef]
- Sandler, I.N.; Wolchik, S.A.; Ayers, T.S. Resilience rather than recovery: A contextual framework on adaptation following bereavement. Death Stud. 2008, 32, 59–73. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Emory, E. Executive function and the frontal lobes: A meta-analytic review. Neuropsychol. Rev. 2006, 16, 17–42. [Google Scholar] [CrossRef]
- Brower, M.C.; Price, B.H. Neuropsychiatry of frontal lobe dysfunction in violent and criminal behaviour: A critical review. J. Neurol. Neurosurg. Psychiatry 2001, 71, 720–726. [Google Scholar] [CrossRef]
- Maier, S.F.; Amat, J.; Baratta, M.V.; Paul, E.; Watkins, L.R. Behavioral control, the medial prefrontal cortex, and resilience. Dialogues Clin. Neurosci. 2006, 8, 397–406. [Google Scholar]
- Shackman, A.J.; Salomons, T.V.; Slagter, H.A.; Fox, A.S.; Winter, J.J.; Davidson, R.J. The integration of negative affect, pain and cognitive control in the cingulate cortex. Nature Reviews Neuroscience. 2011, 12, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Etkin, A.; Egner, T.; Kalisch, R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cogn. Sci. 2011, 15, 85–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnevali, L.; Koenig, J.; Sgoifo, A.; Ottaviani, C. Autonomic and brain morphological predictors of stress resilience. Front. Neurosci. 2018, 12, 228. [Google Scholar] [CrossRef] [PubMed]
- Maren, S.; Phan, K.L.; Liberzon, I. The contextual brain: Implications for fear conditioning, extinction and psychopathology. Nat. Rev. Neurosci. 2013, 14, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Mcewen, B.S.; Gianaros, P.J. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Ann. N. Y. Acad. Sci. 2010, 1186, 190–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, Y.; Li, L.; Jin, C.; Hu, X.; Duan, L.; Eyler, L.T.; Gong, Q.; Song, M.; Jiang, T.; Liao, M.; et al. Abnormal baseline brain activity in posttraumatic stress disorder: A resting-state functional magnetic resonance imaging study. Neurosci. Lett. 2011, 498, 185–189. [Google Scholar] [CrossRef]
- Hull, A.M. Neuroimaging findings in post-traumatic stress disorder: Systematic review. Br. J. Psychiatry 2002, 181, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Shin, L.M.; Orr, S.P.; Carson, M.A.; Rauch, S.L.; Macklin, M.L.; Lasko, N.B.; Peters, P.M.; Metzger, L.J.; Dougherty, D.D.; Cannistraro, P.A.; et al. Regional cerebral blood flow in the amygdala and medial prefrontal cortex during traumatic imagery in male and female vietnam veterans with PTSD. Arch. Gen. Psychiatry 2004, 61, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Lanius, R.; Daniels, J.K.; Williamson, P.C.; Mcfarlane, A.; Moores, K.; Clark, C.R.; Shaw, M.E. Intrinsic network abnormalities in PTSD. Int. J. Neuropsychopharmacol. 2012, 15 (Suppl. 1), 1–271. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Wang, Z.; Qin, L.D.; Wan, J.Q.; Sun, Y.W.; Su, S.S.; Ding, W.N.; Xu, J.R. Early Altered Resting-State Functional Connectivity Predicts the Severity of Post-Traumatic Stress. PLoS ONE 2012, 7, e46833. [Google Scholar] [CrossRef]
- Shim, M.; Im, C.H.; Lee, S.H. Disrupted cortical brain network in post-traumatic stress disorder patients: A resting-state electroencephalographic study. Transl. Psychiatry 2017, 7, e1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, T.W.; Driscoll, D.; Mowrer, S.M.; Sollers, J.J.; Thayer, J.F.; Kirschbaum, C.; Tranel, D. Medial prefrontal cortex damage affects physiological and psychological stress responses differently in men and women. Psychoneuroendocrinology 2010, 35, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulrich-Lai, Y.M.; Herman, J.P. Neural regulation of endocrine and autonomic stress responses. Nat. Rev. Neurosci. 2009, 10, 397–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milad, M.R.; Quirk, G.J. Neurons in medial prefrontal cortex signal memory for fear extinction. Nature 2002, 420, 70–74. [Google Scholar] [CrossRef]
- Campbell, K.L.; Madore, K.P.; Benoit, R.G.; Thakral, P.P.; Schacter, D.L. Increased hippocampus to ventromedial prefrontal connectivity during the construction of episodic future events. Hippocampus 2018, 28, 76–80. [Google Scholar] [CrossRef]
- Yang, Y.; Raine, A.; Colletti, P.; Toga, A.W.; Narr, K.L. Morphological alterations in the prefrontal cortex and the amygdala in unsuccessful psychopaths. J. Abnorm. Psychol. 2010, 119, 546–554. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J.; Stevenson, R.F.; Mander, B.A.; Mnatsakanyan, L.; Hsu, F.P.K.; Vadera, S.; Knight, R.T.; Yassa, M.A.; Lin, J.J. Multiplexing of theta and alpha rhythms in the amygdala-hippocampal circuit supports pattern separation of emotional information. Neuron 2019, 102, 887–898.e5. [Google Scholar] [CrossRef]
- New, A.S.; Fan, J.; Murrough, J.W.; Liu, X.; Liebman, R.E.; Guise, K.G.; Tang, C.Y.; Charney, D.S. A functional magnetic resonance imaging study of deliberate emotion regulation in resilience and posttraumatic stress disorder. Biol. Psychiatry 2009, 66, 656–664. [Google Scholar] [CrossRef]
- Shin, L.M.; Rauch, S.L.; Pitman, R.K. Amygdala, medial prefrontal cortex, and hippocampal function in PTSD. Ann. N. Y. Acad. Sci. 2006, 1071, 67–79. [Google Scholar] [CrossRef] [Green Version]
- Gross, J.J. Emotion regulation: Affective, cognitive, and social consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Ochsner, K.N.; Gross, J.J. The cognitive control of emotion. Trends Cogn. Sci. 2005, 9, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Wager, T.D.; Davidson, M.L.; Hughes, B.L.; Lindquist, M.A.; Ochsner, K.N. Prefrontal-subcortical pathways mediating successful emotion regulation. Neuron 2008, 59, 1037–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inzlicht, M.; Bartholow, B.D.; Hirsh, J.B. Emotional foundations of cognitive control. Trends Cogn. Sci. 2015, 19, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharot, T.; Riccardi, A.M.; Raio, C.M.; Phelps, E.A. Neural mechanisms mediating optimism bias. Nature 2007, 450, 102–105. [Google Scholar] [CrossRef]
- Schacter, D.L.; Addis, D.R. The optimistic brain. Nat. Neurosci. 2007, 10, 1345–1347. [Google Scholar] [CrossRef]
- Kragel, P.A.; Kano, M.; Van Oudenhove, L.; Ly, H.G.; Dupont, P.; Rubio, A.; Delon-Martin, C.; Bonaz, B.L.; Manuck, S.B.; Gianaros, P.J.; et al. Generalizable representations of pain, cognitive control, and negative emotion in medial frontal cortex. Nat. Neurosci. 2018, 21, 283–289. [Google Scholar] [CrossRef]
- Tracey, I.; Mantyh, P.W. The cerebral signature for pain perception and its modulation. Neuron 2007, 55, 377–391. [Google Scholar] [CrossRef] [Green Version]
- Jahn, A.; Nee, D.E.; Alexander, W.H.; Brown, J.W. Distinct regions within medial prefrontal cortex process pain and cognition. J. Neurosci. 2016, 36, 12385–12392. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Nakae, K.; Ishii, S.; Naoki, H. Uncertainty-dependent extinction of fear memory in an amygdala-MPFC neural circuit model. PLoS Comput. Biol. 2016, 12, e1005099. [Google Scholar] [CrossRef]
- Winston, J.S.; Strange, B.A.; O’doherty, J.; Dolan, R.J. Automatic and intentional brain responses during evaluation of trustworthiness of faces. Nat. Neurosci. 2002, 5, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Wiech, K.; Ploner, M.; Tracey, I. Neurocognitive aspects of pain perception. Trends Cogn. Sci. 2008, 12, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Morey, R.A.; Haswell, C.C.; Hooper, S.R.; De Bellis, M.D. Amygdala, hippocampus, and ventral medial prefrontal cortex volumes differ in maltreated youth with and without chronic posttraumatic stress disorder. Neuropsychopharmacology 2016, 41, 791–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonanno, G.A.; Burton, C.L. Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspect. Psychol. Sci. 2013, 8, 591–612. [Google Scholar] [CrossRef] [PubMed]
- Gabrys, R.L.; Howell, J.W.; Cebulski, S.F.; Anismana, H.; Matheson, K. Acute stressor effects on cognitive flexibility: Mediating role of stressor appraisals and cortisol. Stress 2019, 22, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Liston, C.; McEwen, B.S.; Casey, B.J. Psychosocial stress reversibly disrupts prefrontal processing and attentional control. Proc. Natl. Acad. Sci. USA 2009, 106, 912–917. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.; Johnson, N.F.; Cilles, S.E.; Gold, B.T. Common and distinct mechanisms of cognitive flexibility in prefrontal cortex. J. Neurosci. 2011, 31, 4771–4779. [Google Scholar] [CrossRef] [Green Version]
- Dajani, D.R.; Uddin, L.Q. Demystifying cognitive flexibility: Implications for clinical and developmental neuroscience. Trends Neurosci. 2015, 38, 571–578. [Google Scholar] [CrossRef] [Green Version]
- Hyafil, A.; Summerfield, C.; Koechlin, E. Two mechanisms for task switching in the prefrontal cortex. J. Neurosci. 2009, 29, 5135–5142. [Google Scholar] [CrossRef]
- Braver, T.S.; Paxton, J.L.; Locke, H.S.; Barch, D.M. Flexible neural mechanisms of cognitive control within human prefrontal cortex. Proc. Natl. Acad. Sci. USA 2009, 106, 7351–7356. [Google Scholar] [CrossRef] [Green Version]
- Gabrys, R.L.; Dixon, K.; Anisman, H. Traumatic life events in relation to cognitive flexibility: Moderating role of the BDNF Val66Met gene polymorphism. Front. Behav. Neurosci. 2017, 11, 241. [Google Scholar] [CrossRef] [Green Version]
- Iacoviello, B.M.; Charney, D.S. Cognitive and behavioral components of resilience to stress. In Stress Resilience; Academic Press: Cambridge, MA, USA, 2020; pp. 23–31. [Google Scholar] [CrossRef]
- Fenster, R.J.; Lebois, L.A.M.; Ressler, K.J.; Suh, J. Brain circuit dysfunction in post-traumatic stress disorder: From mouse to man. Nat. Rev. Neurosci. 2018, 19, 535–551. [Google Scholar] [CrossRef] [PubMed]
- McDaniel, R.R.; Jordan, M.E.; Fleeman, B.F. Surprise, surprise, surprise! A complexity science view of the unexpected. Health Care Manag. Rev. 2003, 28, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.W.; Anda, R.F.; Edwards, V.J.; Felitti, V.J.; Dube, S.R.; Giles, W.H. Adverse childhood experiences and childhood autobiographical memory disturbance. Child Abus. Negl. 2007, 31, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Pechtel, P.; Pizzagalli, D.A. Effects of early life stress on cognitive and affective function: An integrated review of human literature. Psychopharmacology (Berl) 2011, 214, 55–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Z.; Bayley, M.T.; Perrier, L.; Dhir, P.; Dépatie, L.; Comper, P.; Ruttan, L.; Lay, C.; Munce, S.E.P. The association between adverse childhood experiences and adult traumatic brain injury/concussion: A scoping review. Disabil. Rehabil. 2019, 41, 1360–1366. [Google Scholar] [CrossRef]
- McEwen, B.S. In pursuit of resilience: Stress, epigenetics, and brain plasticity. Ann. N. Y. Acad. Sci. 2016, 1373, 56–64. [Google Scholar] [CrossRef]
- McEwen, B.S.; Morrison, J.H. The brain on stress: Vulnerability and plasticity of the prefrontal cortex over the life course. Neuron 2013, 79, 16–29. [Google Scholar] [CrossRef] [Green Version]
- Radley, J.; Morilak, D.; Viau, V.; Campeau, S. Chronic stress and brain plasticity: Mechanisms underlying adaptive and maladaptive changes and implications for stress-related CNS disorders. Neurosci. Biobehav. Rev. 2015, 58, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Nava, E.; Röder, B. Adaptation and maladaptation. Prog. Brain Res. 2011, 191, 177–194. [Google Scholar] [CrossRef]
- Vitaliano, P.P.; Russo, J.; Carr, J.E.; Maiuro, R.D.; Becker, J. The ways of coping checklist: Revision and psychometric properties. Multivar. Behav. Res. 1985, 20, 3–26. [Google Scholar] [CrossRef]
- Elklit, A. Coping styles questionnaire: A contribution to the validation of a scale for measuring coping strategies. Personal. Individ. Differ. 1996, 21, 809–812. [Google Scholar] [CrossRef]
- Carver, C.; Scheier, M.; Weintraub, J. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Meins, E.; McCarthy-Jones, S.; Fernyhough, C.; Lewis, G.; Bentall, R.P.; Alloy, L.B. Assessing negative cognitive style: Development and validation of a short-form version of the cognitive style questionnaire. Pers. Individ. Differ. 2012, 52, 581–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabrys, R.L.; Tabri, N.; Anisman, H.; Matheson, K. Cognitive control and flexibility in the context of stress and depressive symptoms: The cognitive control and flexibility questionnaire. Front. Psychol. 2018, 9, 2219. [Google Scholar] [CrossRef] [PubMed]
- Garnefski, N.; Kraaij, V. The cognitive emotion regulation questionnaire: Psychometric features and prospective relationships with depression and anxiety in adults. Eur. J. Psychol. Assess. 2007, 23, 141–149. [Google Scholar] [CrossRef]
- Allport, A.; Styles, E.A.; Hsieh, S. Shifting intentional set: Exploring the dynamic control of tasks. In Attention and performance XV: Conscious and nonconscious information processing; Umiltá, C., Moskovitch, M., Eds.; The MIT Press: Cambridge, MA, USA, 1994; Volume XV, pp. 421–452. [Google Scholar]
- Richards, J.M.; Gross, J.J. Emotion Regulation and Memory: The Cognitive Costs of Keeping One’s Cool. J. Pers. Soc. Psychol. 2000, 79, 410–424. [Google Scholar] [CrossRef]
- Kutas, M.; Federmeier, K.D. Thirty years and counting: Finding meaning in the N400 component of the Event-Related Brain Potential (ERP). Annu. Rev. Psychol. 2011, 62, 621–647. [Google Scholar] [CrossRef] [Green Version]
- Trempler, I.; Schiffer, A.M.; El-Sourani, N.; Ahlheim, C.; Fink, G.R.; Schubotz, R.I. Frontostriatal contribution to the interplay of flexibility and stability in serial prediction. J. Cogn. Neurosci. 2017, 29, 298–309. [Google Scholar] [CrossRef] [Green Version]
- Chumbley, J.R.; Burke, C.J.; Stephan, K.E.; Friston, K.J.; Tobler, P.N.; Fehr, E. Surprise beyond prediction error. Hum. Brain Mapp. 2014, 35, 4805–4814. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Section Highlights | Authors (Year) | Article (Title) | Source (Journal) | Relevant Findings and Their Implications to the Highlights | |
|---|---|---|---|---|---|
| Section 1 | Human resilience may protect us from developing mental health issues. | Southwick and Charney (2012) | The Science of Resilience: Implications for the Prevention and Treatment of Depression | Science | This paper shows the importance of resilience in protecting humans from developing mental issues. Authors review interdisciplinary factors that influences resilience and call for integrating salient concepts of resilience into relevant fields of medicine, mental health, and science. |
| Southwick et al. (2014) | Resilience Definitions, Theory, and Challenges: Interdisci-plinary Perspectives | European Journal of Psychotrau-matology | This paper summarizes the discussion from multidisciplinary experts in the study of psychological resilience for the most pressing current questions in the field of resilience research. The consensus among these experts was resilience is a complex construct and multiple levels of analysis from interdisciplinary perspectives are urgent and needed. | ||
| Section 2 | Resilience refers to a dynamic process encompassing positive adaptation within the context of significant adversity. | Fletcher and Sarkar (2013) | Psychological Resilience: A Review and Critique of Definitions, Concepts, and Theory | European Psychologist. | In this paper, the authors review the literature and operationalized definitions of resilience, suggesting positive adaptation must be conceptually appropriate to the adversity examined. They argue more conceptual study is needed that should take into account the multiple demands individuals encounter, the meta-cognitive and -emotive processes that affect the resilience–stress relationship, and the conceptual distinction between resilience and coping. |
| Mancini and Bonanno (2009) | Predictors and Parameters of Resilience to Loss: Toward an Individual Differences Model | Journal of Personality | In this paper, Bonanno, et al. discussed what is the resilient capacity by reviewing prior work (G.A. Bonanno, 2004). They provide an operational definition of resilience as a specific trajectory of psychological outcome and describe how the resilient trajectory differs from other trajectories of response to loss. They integrate these individual differences in a hypothesized model of resilience, focusing on their role in appraisal processes and the use of social resources. In line with this paper, we suggest the period between experience difficulties completing their normal tasks at daily functioning until begin to return to their pre-loss level of functioning that able to complete tasks in daily life may see as indexes of positive adaptation. | ||
| Section 3 | Cognitive appraisal mediates cognition–emotion–perception processes from adverse experience to positive adaptation. | Major et al. (1998) | Personal Resilience, Cognitive Appraisals, and Coping: An Integrative Model of Adjustment to Abortion | Journal of Personality and Social Psychology | In this paper, the authors found that women who had more resilient personality resources to draw on (i.e., self-esteem, perceived control, and optimism) were less likely to appraise their upcoming abortions as stressful. The results implied the role of cognitive appraisals in personal resilience and coping are discussed as possible mediators of this relationship. |
| Verduyn et al. (2011) | The Relation Between Event Processing and the Duration of Emotional Experience | Emotion | In this paper, the authors explored the factors that affect the duration of emotional experience. Specifically, they focus on the difference between rumination versus reappraisal of an emotional event. They explored how this difference affects the “duration” of an emotional experience, and in which direction it proceeds (shortening or lengthening). The authors argue that cognition is the primary factor impacting duration and the experience of emotion, by claiming that “thoughts appear to act as the fuel that stirs up the emotional fire and leads to a prolongation of the episode”. This study demonstrates the significance of cognitive appraisal by indicating its role in the duration of an emotional experience. | ||
| Doukas et al. (2019) | Hurts So Good: Pain as an Emotion Regulation Strategy. | Emotion | In this paper, the authors tested two primary hypotheses: some people will choose to inflict pain to regulate negative emotional states, and (b) pain provides effective short-term relief from negative emotion. Their results suggest physical pain as a response to an emotion regulation strategy, linking physical pain, emotional response, and cognitive appraisal. | ||
| Eysenck et al. (2007) | Anxiety and Cognitive Performance: Attentional Control Theory. | Emotion | In this paper, Eysenck et al. discussed top-down and bottom-up processing in regulating two central executive functions related to attentional control: inhibition and shifting. Mental health impaired (e.g., anxiety) disrupts these two functions by weakens the degree to which inhibitory mechanisms can regulate automatic responses, that is, anxiety weakens top-down cognitive control. They illuminate the functional role of attention in modulating these processes and neatly capture the special contribution of cortical processing to adaptive success. This theory has a profound impact on mental health research. We speculate this regulatory mechanism also exists in the process of positive adaption in the face of adversity. | ||
| Section 4 | Frontal brain network connects cognitive control, emotion regulation, and pain perception | Shin et al. (2004) | Regional Cerebral Blood Flow in the Amygdala and Medial Prefrontal Cortex during Traumatic Imagery in Male and Female Vietnam Veterans with PTSD | Archives of General Psychiatry | Shin et al. have reported that PTSD patients showed amygdala hyperactivation and frontal hypoactivation and found that these regional activities were significantly correlated with the Clinician-Administered PTSD Scale score. Indeed, some functional magnetic resonance imaging (fMRI) studies have shown an altered resting-state FC in some brain regions, including the amygdala, anterior cingulate cortex (ACC), and medial prefrontal cortex in patients with PTSD, as compared to healthy controls. These findings suggested that disrupted frontal network connectivity may be related to those who struggled to recover from adverse experiences. |
| Milad and Quirk (2002) | Neurons in Medial Prefrontal Cortex Signal Memory for Fear Extinction | Nature | Aversive experience events are often turned into unwanted memories. Simple reminders can then trigger the involuntary retrieval of these memories. Milad and Quirk (2002) used animal models to show the role of mPFC in storing long-term memories for fear of extinction [89]. The mPFC is also part of a core network that not only supports the recollection of past episodes but also imagines prospective events (e.g., when and where to meet a person). | ||
| Section 5 | Cognitive flexibility moderate resilience by regulating frontal brain circuitry. | Gabrys et al. (2017) | Traumatic Life Events in Relation to Cognitive Flexibility: Moderating Role of the BDNF Val66Met Gene Polymorphism | Frontiers in Behavioral Neuroscience | In this paper, the authors showed that children who experience a longer duration of trauma experience greater difficulties in attention-shifting, highlighting the link between cognitive flexibility and early-life adverse experiences. |
| Gabrys et al. (2019) | Acute Stressor Effects on Cognitive Flexibility: Mediating Role of Stressor Appraisals and Cortisol. | Stress | In this paper, the authors examined the effects of an acute psychosocial stressor (the Trier Social Stress Test) on a specific form of cognitive flexibility, namely that of set-shifting, which was assessed by the Berg’s Card Sorting Task (BCST). Their results showed that exposure to an acute social stressor promoted better performance on the BSCT, but this enhancing effect was minimized among individuals who appraised the stressor as being uncontrollable. | ||
| Bonanno and Burton (2013) | Regulatory Flexibility: An Individual Differences Perspective on Coping and Emotion Regulation | Perspectives on Psychological Science | In this paper, the author describes emotion-regulation flexibility, defined as the matching of emotion-regulation strategy to environmental circumstance. They segmented emotion-regulation flexibility into three separable valuation systems: (1) how we read the situation or context-sensitivity; (2) a repertoire of behaviors; and (3) the ability to regroup by using corrective feedback. This paper echoes our concept of flexibility in regulating resilience: We focus on neurocognitive aspects of flexibility and suggest its mechanism underlies human resilience. | ||
| Section 6 | Examples, questions remain and future direction. | Parsons et al. (2016) | A Cognitive Model of Psychological Resilience | Journal of Experimental Psychopathology | The authors proposed a cognitive model to describe the role of selective information processing in positive adaption in the face of adversity. In their theoretical framework, they provide some possible psychological task manipulations (e.g., threat cues to induce anxiety) that may enable the study of the development of cognitive functions that are important in the resilience process. This paper resonates with our paper and shows the potential to examine whether the cognitive aspect plays a role in resilience. |
| 1. Brain structures and functions investigation |
|
| 2. Brain plasticity and cognitive training intervention |
|
| 3. Developmental consequences in resilience |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, Z.-F.; Hsieh, S. Neurocognitive Mechanism of Human Resilience: A Conceptual Framework and Empirical Review. Int. J. Environ. Res. Public Health 2019, 16, 5123. https://doi.org/10.3390/ijerph16245123
Yao Z-F, Hsieh S. Neurocognitive Mechanism of Human Resilience: A Conceptual Framework and Empirical Review. International Journal of Environmental Research and Public Health. 2019; 16(24):5123. https://doi.org/10.3390/ijerph16245123
Chicago/Turabian StyleYao, Zai-Fu, and Shulan Hsieh. 2019. "Neurocognitive Mechanism of Human Resilience: A Conceptual Framework and Empirical Review" International Journal of Environmental Research and Public Health 16, no. 24: 5123. https://doi.org/10.3390/ijerph16245123