Do Sociodemographic Factors and Urban Green Space Affect Mental Health Outcomes Among the Urban Elderly Population?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data
2.2.1. Control Variables
2.2.2. Response Variables
2.2.3. Explanatory Variables
2.3. Statistical Analysis
3. Results
3.1. Study Sample Characteristics
3.2. Association of Sociodemographic Characteristics with Stress Levels and Symptoms of Depression
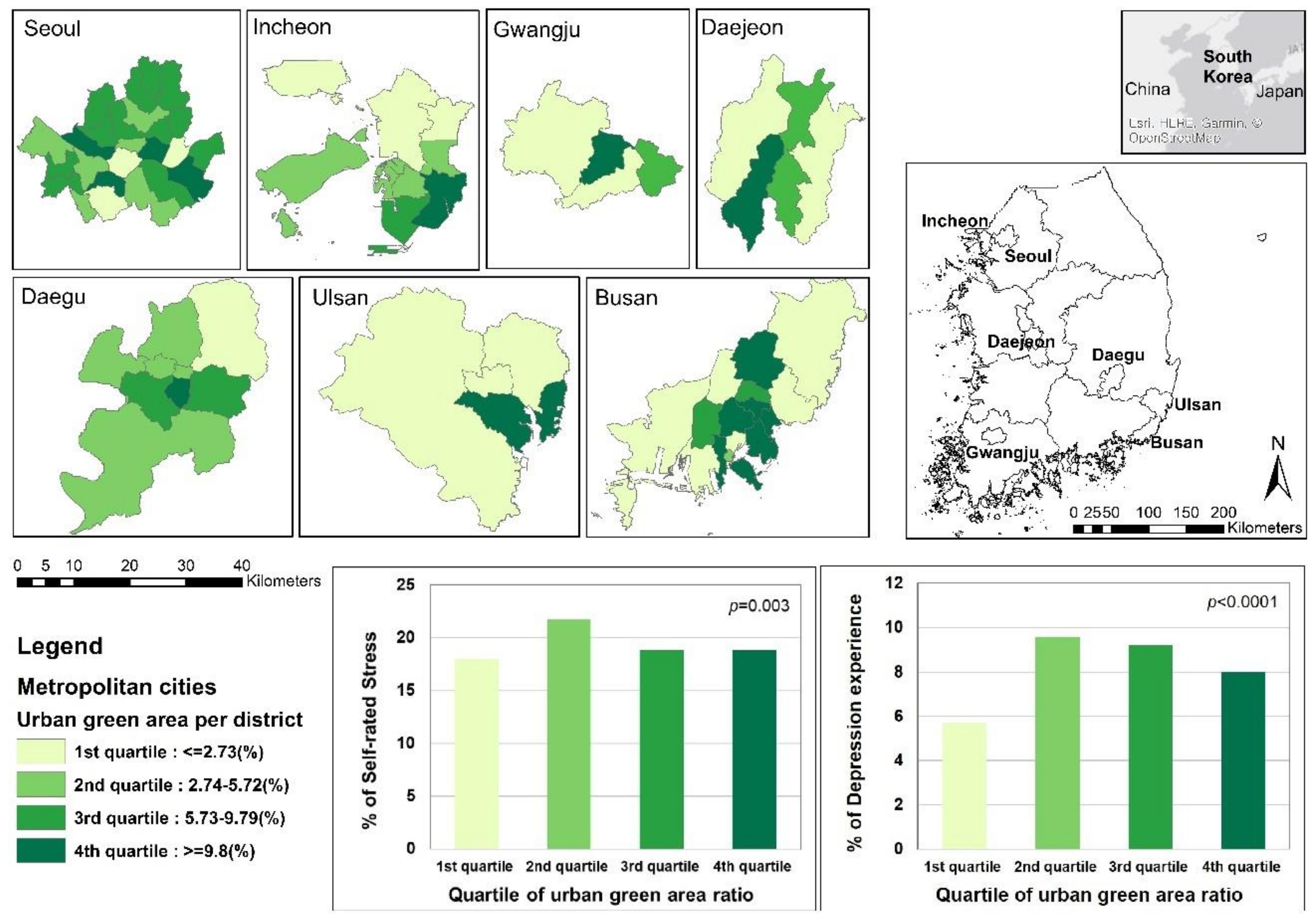
3.3. Association of the Urban Green Area Ratio with Stress Levels and Symptoms of Depression
4. Discussion
4.1. Policy Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Health and Aging; WHO: New York, NY, USA, 2011; pp. 2–23. [Google Scholar]
- Korea Institute for Health and Social Affairs. 2017 Survey of the Elderly; KIHASA: Sejong, Republic of Korea, 2017; pp. 29–62. [Google Scholar]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.; Peeters Geeske, G.M.E.E.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Urban Population Status (2017). Available online: http://kosis.kr (accessed on 7 August 2018).
- Kim, J.-H.; Gu, D.; Sohn, W.; Kil, S.H.; Kim, H.; Lee, D.K. Neighborhood landscape spatial patterns and land surface temperature: An empirical study on single-family residential areas in Austin, Texas. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Okkels, N.; Kristiansen, C.B.; Munk-Jørgensen, P.; Sartorius, N. Urban mental health: challenges and perspectives. Curr. Opin. Psychiatry 2018, 31, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Deckers, K.; van Boxtel, M.P.J.; Schiepers, O.J.G.; de Vugt, M.; Muñoz Sánchez, J.L.; Anstey, K.J.; Brayne, C.; Dartigues, J.-F.; Engedal, K.; Kivipelto, M.; et al. Target risk factors for dementia prevention: a systematic review and Delphi consensus study on the evidence from observational studies. Int. J. Geriatr. Psychiatry 2015, 30, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Langa, K.M. Is the risk of Alzheimer’s disease and dementia declining? Alzheimers. Res. Ther. 2015, 7, 34. [Google Scholar] [CrossRef] [PubMed]
- Min, K.B.; Kim, H.J.; Kim, H.J.; Min, J.Y. Parks and green areas and the risk for depression and suicidal indicators. Int. J. Public Health 2017, 62, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, A.M.; Winblad, B.; Jönsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimer’s Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ward Thompson, C.; Aspinall, P.; Roe, J.; Robertson, L.; Miller, D. Mitigating stress and supporting health in deprived urban communities: The importance of green space and the social environment. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Lee, C.; Olvera, N.E.; Ellis, C.D. The Role of Landscape Spatial Patterns on Obesity in Hispanic Children Residing in Inner-City Neighborhoods. J. Phys. Act. Heal. 2014, 11, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- McEachan, R.R.C.; Prady, S.L.; Smith, G.; Fairley, L.; Cabieses, B.; Gidlow, C.; Wright, J.; Dadvand, P.; van Gent, D.; Nieuwenhuijsen, M.J. The association between green space and depressive symptoms in pregnant women: Moderating roles of socioeconomic status and physical activity. J. Epidemiol. Community Health 2016, 70, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Orstad, S.L.; McDonough, M.H.; James, P.; Klenosky, D.B.; Laden, F.; Mattson, M.; Troped, P.J. Neighborhood walkability and physical activity among older women: Tests of mediation by environmental perceptions and moderation by depressive symptoms. Prev. Med. (Baltim). 2018, 116, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.T.C.; Shanahan, D.F.; Hudson, H.L.; Plummer, K.E.; Siriwardena, G.M.; Fuller, R.A.; Anderson, K.; Hancock, S.; Gaston, K.J. Doses of neighborhood nature: The benefits for mental health of living with nature. Bioscience 2017, 67, 147–155. [Google Scholar] [CrossRef]
- Guffanti, G.; Gameroff, M.J.; Warner, V.; Talati, A.; Glatt, C.E.; Wickramaratne, P.; Weissman, M.M. Heritability of major depressive and comorbid anxiety disorders in multi-generational families at high risk for depression. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2016, 171, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.; Jané-Llopis, E. Mental health and global well-being. Health Promot. Int. 2011, 26, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Compton, M.T.; Shim, R.S. The Social Determinants of Mental Health. Focus (Madison). 2015, 13, 419–425. [Google Scholar] [CrossRef]
- Ord, K.; Mitchell, R.; Pearce, J. Is level of neighbourhood green space associated with physical activity in green space? Int. J. Behav. Nutr. Phys. Act. 2013, 10, 127. [Google Scholar] [CrossRef] [PubMed]
- Mota-Pereira, J.; Carvalho, S.; Silverio, J.; Fonte, D.; Pizarro, A.; Teixeira, J.; Ribeiro, J.C.; Ramos, J. Moderate physical exercise and quality of life in patients with treatment-resistant major depressive disorder. J. Psychiatr. Res. 2011, 45, 1657–1659. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Johansson, G.; Kylin, C. Residence in the social ecology of stress and restoration. J. Soc. Issues 2003, 59, 611–636. [Google Scholar] [CrossRef]
- Douglas, O.; Lennon, M.; Scott, M. Green space benefits for health and well-being: A life-course approach for urban planning, design and management. Cities 2017, 66, 53–62. [Google Scholar] [CrossRef]
- Mamplekou, E.; Bountziouka, V.; Psaltopoulou, T.; Zeimbekis, A.; Tsakoundakis, N.; Papaerakleous, N.; Gotsis, E.; Metallinos, G.; Pounis, G.; Polychronopoulos, E.; et al. Urban environment, physical inactivity and unhealthy dietary habits correlate to depression among elderly living in eastern Mediterranean islands: The MEDIS (MEDiterranean ISlands elderly) study. J. Nutr. Health Aging 2010, 14, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Mas, M.T.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control and Prevention. Community Health Survey, 2015. Available online: https://chs.cdc.go.kr (accessed on 17 January 2016).
- Kim, J.; Kim, H. Demographic and environmental factors associated with mental health: A cross-sectional study. Int. J. Environ. Res. Public Health 2017, 14, 431. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-Y.; Yu, C.-P.; Wu, C.-D.; Pan, W.-C.; Lee, H.-Y.; Yu, C.-P.; Wu, C.-D.; Pan, W.-C. The Effect of Leisure Activity Diversity and Exercise Time on the Prevention of Depression in the Middle-Aged and Elderly Residents of Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 654. [Google Scholar] [CrossRef] [PubMed]
- Borge, L.-E.; Rattsø, J. Young and Old Competing for Public Welfare Services; CESifo Working Paper Series No. 2223; CESifo: Munich, Germany, 2008; pp. 1–4. [Google Scholar]
- Walker, A.; Martimo, K. Ageing and intergenerational relations in Britain. In Comparing Social Policies: Exploring New Perspectives in Britain and Japan; The Policy Press: Bristol, UK, 2003; p. 49. [Google Scholar]
- Zale, E.L.; Maisto, S.A.; Ditre, J.W. Anxiety and Depression in Bidirectional Relations Between Pain and Smoking. Behav. Modif. 2016, 40, 7–28. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, A.H.; Kashan, R.S.; Shpigel, D.M.; Esan, H.; Taha, F.; Lee, C.J.; Funk, A.P.; Goodwin, R.D. Depression and cigarette smoking behavior: A critical review of population-based studies. Am. J. Drug Alcohol Abuse 2017, 43, 416–431. [Google Scholar] [CrossRef] [PubMed]
- Saunders, P.A.; Copeland, J.R.M.; Dewey, M.E.; Davidson, I.A.; Mcwilliam, C.; Sharma, V.; Sullivan, C. Heavy Drinking as a Risk Factor for Depression and Dementia in Elderly Men. Br. J. Psychiatry 1991, 159, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Driessen, M.; Meier, S.; Hill, A.; Wetterling, T.; Lange, W.; Junghanns, K. The course of anxiety, depression and drinking behaviours after completed detoxification in alcoholics with and without comorbid anxiety and depressive disorders. Alcohol Alcohol. 2001, 36, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.P.; Hughes, T.L.; Cho, Y.I.; Wilsnack, S.C.; Aranda, F.; Szalacha, L.A. Hazardous drinking, depression, and anxiety among sexual-minority women: Self-medication or impaired functioning? J. Stud. Alcohol Drugs 2013, 74, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Kim, W. Drinking Culture of Elderly Korean Immigrants in Canada: A Focus Group Study. J. Cross. Cult. Gerontol. 2009, 24, 339–353. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Park, H.S.; Lee, T.S.; Kim, M.K.; Kim, Y.H. Korean working adults’ and undergraduates’ attitudes towards, and self-efficacy in joining drinking parties. Soc. Behav. Personal. an Int. J. 2006, 34, 487–498. [Google Scholar] [CrossRef]
- Teo, A.R.; Choi, H.; Valenstein, M. Social Relationships and Depression: Ten-Year Follow-Up from a Nationally Representative Study. PLoS ONE 2013, 8, e62396. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Hawkley, L.C.; Thisted, R.A. Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychol. Aging 2010, 25, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Xue, D.; Liu, Y. The Relationship between Air Pollution and Depression in China: Is Neighbourhood Social Capital Protective? Int. J. Environ. Res. Public Heal. 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Xue, D.; Liu, Y.; Chen, H.; Qiu, Y. The relationship between urbanization and depression in China: The mediating role of neighborhood social capital. Int. J. Equity Health 2018, 17, 105. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.; Albert, C.; Von Haaren, C. The elderly in green spaces: Exploring requirements and preferences concerning nature-based recreation. Sustain. Cities Soc. 2018, 38, 582–593. [Google Scholar] [CrossRef]
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007; ISBN 9789241547307. Available online: http://www.who.int/ageing/age_friendly_cities_guide/en/ (accessed on 22 February 2017).
- Norman, G.J.; Nutter, S.K.; Ryan, S.; Sallis, J.F.; Calfas, K.J.; Patrick, K. Community design and access to recreational facilities as correlates of adolescent physical activity and body-mass index. J. Phys. Act. Heal. 2006, 3, S118–S128. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.J.; Tester, J. Environment shapes health, including children’s mental health. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shepley, M.M.; Rodiek, S.D. Aging in place at home through environmental support of physical activity: An Interdisciplinary conceptual framework and analysis. J. Hous. Elderly 2012, 26, 338–354. [Google Scholar] [CrossRef]
- Pleson, E.; Nieuwendyk, L.M.; Lee, K.K.; Chaddah, A.; Nykiforuk, C.I.J.; Schopflocher, D. Understanding older adults’ usage of community green spaces in Taipei, Taiwan. Int. J. Environ. Res. Public Health 2014, 11, 1444–1464. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, C.; Gallacher, J.; Webster, C. Urban built environment configuration and psychological distress in older men: Results from the Caerphilly study. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Orban, E.; Sutcliffe, R.; Roggenbuck, U.; Dragano, N.; Wahl, S.; Weyers, S.; Jöckel, K.; Moebus, S. Residential surrounding greenness, self-rated health and associations with neighborhood satisfaction and social capital. Das Gesundheitswes. 2016, 78, A118. [Google Scholar] [CrossRef]
- Gascon, M.; Sánchez-Benavides, G.; Dadvand, P.; Martínez, D.; Gramunt, N.; Gotsens, X.; Cirach, M.; Vert, C.; Molinuevo, J.L.; Crous-Bou, M.; et al. Long-term exposure to residential green and blue spaces and anxiety and depression in adults: A cross-sectional study. Environ. Res. 2018, 162. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Cline, H.; Turkheimer, E.; Duncan, G.E. Access to green space, physical activity and mental health: A twin study. J. Epidemiol. Community Health 2015, 69, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-T.; Prina, A.M.; Jones, A.; Matthews, F.E.; Brayne, C.; Mrc Cfas, M. Older people, the natural environment and common mental disorders: Cross-sectional results from the cognitive function and ageing study. BMJ Open 2015, 5, e007936. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Mental health benefits of neighbourhood green space are stronger among physically active adults in middle-to-older age: Evidence from 260,061 Australians. Prev. Med. (Baltim). 2013, 57, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Lin, C.; Tsai, M.; Tsai, Y.; Chen, C. Effects of Short Forest Bathing Program on Autonomic Nervous System Activity and Mood States in Middle-Aged and Elderly Individuals. Int. J. Environ. Res. Public Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Son, S.A. Qualitative Assessment of Experience on Urban Forest Therapy Program for Preventing Dementia of the Elderly Living Alone in Low-Income Class. J People Plants Env. 2018, 21, 565–574. [Google Scholar] [CrossRef]
- Dolling, A.; Nilsson, H.; Lundell, Y. Stress recovery in forest or handicraft environments—An intervention study. Urban For. Urban Green. 2017, 27, 162–172. [Google Scholar] [CrossRef]
- Lewis, C.A. Effects of plants and gardening in creating interpersonal and community well-being. In Role of Horticulture in Human Well-being and Social Development: A National Symposium; Timber Press: Arlington, VA, USA, 1992; pp. 55–65. [Google Scholar]
- Maller, C.; Townsend, M.; Pryor, A.; Brown, P.; St Leger, L. Healthy nature healthy people: ‘Contact with nature’ as an upstream health promotion intervention for populations. Health Promot. Int. 2006, 21, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Yalom, I.D.; Crouch, E.C. The theory and practice of group psychotherapy. Br. J. Psychiatry 1990, 157, 304–306. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Category | All | Sex | x2 (p) | ||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||
| n | % | n | % | n | % | |||
| Total | 11,408 | 100 | 4922 | 43.1 | 6486 | 56.9 | ||
| Age group (years) | 65–69 | 3865 | 33.9 | 1758 | 35.7 | 2107 | 32.5 | 50.857 (0.000) |
| 70–79 | 5789 | 50.7 | 2540 | 51.6 | 3249 | 50.1 | ||
| 80+ | 1754 | 15.4 | 624 | 12.7 | 1130 | 17.4 | ||
| Household type | Solitary | 2155 | 18.9 | 423 | 8.6 | 1732 | 26.7 | 930.290 (0.000) |
| 1 generation | 5058 | 44.3 | 2891 | 58.7 | 2167 | 33.4 | ||
| 2, 3 generations | 4195 | 36.8 | 1608 | 32.7 | 2587 | 39.9 | ||
| Education level | Primary school or less | 5635 | 49.4 | 1377 | 28.0 | 4258 | 65.6 | 1736.141 (0.000) |
| Middle school or high school | 4467 | 39.2 | 2565 | 52.1 | 1902 | 29.3 | ||
| College or university | 1088 | 9.5 | 787 | 16.0 | 301 | 4.6 | ||
| Master’s degree or higher | 218 | 1.9 | 193 | 3.9 | 25 | 0.4 | ||
| Financial aid | No | 10,638 | 93.3 | 4670 | 94.9 | 5968 | 92.0 | 36.534 (0.000) |
| Yes | 770 | 6.7 | 252 | 5.1 | 518 | 8.0 | ||
| Monthly household income in thousands of Korean Won (KRW) | <1000 (<887 USD) | 4758 | 41.7 | 1746 | 35.5 | 3012 | 46.4 | 146.626 (0.000) |
| 1000–3000 (887–2663 USD) | 4266 | 37.4 | 2093 | 42.5 | 2173 | 33.5 | ||
| 3000+ (2663 USD+) | 2384 | 20.9 | 1083 | 22.0 | 1301 | 20.1 | ||
| Labor market participation | No | 8536 | 74.8 | 3179 | 64.6 | 5357 | 82.6 | 481.626 (0.000) |
| Yes | 2872 | 25.2 | 1743 | 35.4 | 1129 | 17.4 | ||
| Comorbidity prevalence | Hypertension | 5758 | 50.5 | 2334 | 47.4 | 3424 | 52.8 | 32.292 (0.000) |
| Diabetes | 2398 | 21 | 1060 | 21.5 | 1338 | 20.6 | 1.386 (0.239) | |
| Dyslipidemia | 2195 | 19.2 | 694 | 14.1 | 1501 | 23.1 | 147.245 (0.000) | |
| Arthritis | 1999 | 17.5 | 338 | 6.9 | 1661 | 25.6 | 680.139 (0.000) | |
| Cigarette Smoker | Current | 1089 | 9.5 | 947 | 19.2 | 142 | 2.2 | 6142.901 (0.000) |
| Former | 2985 | 26.2 | 2795 | 56.8 | 190 | 2.9 | ||
| Never smoked | 7334 | 64.3 | 1180 | 24.0 | 6154 | 94.9 | ||
| Alcohol consumer | No | 5947 | 52.1 | 1677 | 34.1 | 4270 | 65.8 | 1131.331 (0.000) |
| Yes | 5461 | 47.9 | 3245 | 65.9 | 2216 | 34.2 | ||
| Moderate physical activity (day/week) | 0 | 8335 | 73.1 | 3410 | 69.3 | 4925 | 75.9 | 85.0 (0.000) |
| 1–3 | 1407 | 12.3 | 628 | 12.8 | 779 | 12.0 | ||
| 4+ | 1666 | 14.6 | 884 | 18.0 | 782 | 12.1 | ||
| Regular social activity (monthly) | No | 5130 | 45 | 1986 | 40.3 | 3144 | 48.5 | 74.636 (0.000) |
| Yes | 6278 | 55 | 2936 | 59.7 | 3342 | 51.5 | ||
| Self-rated stress level | Slightly or rarely | 9205 | 80.7 | 4186 | 85.0 | 5019 | 77.4 | 105.506 (0.000) |
| Very much or a lot | 2203 | 19.3 | 736 | 15.0 | 1467 | 22.6 | ||
| Symptoms of depression | 916 | 8.0 | 271 | 5.5 | 645 | 9.9 | 74.656 (0.000) | |
| Variable | Category | Odds Ratio (95% CI) | |
|---|---|---|---|
| Self-Rated Stress Level | Symptoms of Depression | ||
| Sex | Female | 1.564 (1.330–1.839) ** | 1.577 (1.242–2.003) ** |
| Male | Reference | Reference | |
| Age group (years) | 65–69 | 1.556 (1.323–1.832) ** | 1.232 (0.989–1.534) |
| 70–79 | 1.419 (1.225–1.642) ** | 1.068 (0.880–1.296) | |
| 80+ | Reference | Reference | |
| Household type | Solitary | 0.632 (0.543–0.736) ** | 1.075 (0.878–1.316) |
| 1 generation | 0.778 (0.690–0.876) ** | 0.722 (0.603–0.865) ** | |
| 2, 3 generations | Reference | Reference | |
| Education level | Primary school or less | 1.089 (0.706–1.681) | 0.766 (0.404–1.454) |
| Middle school or high school | 0.944 (0.614–1.451) | 0.790 (0.419–1.492) | |
| College or university | 1.022 (0.650-1.607) | 0.819 (0.418–1.605) | |
| Master’s degree or higher | Reference | Reference | |
| Financial aid | No | 0.529 (0.446–0.626) ** | 0.534 (0.433–0.659) ** |
| Yes | Reference | Reference | |
| Monthly household income in thousands of Korean Won (KRW) | <1000 (<887 USD) | 1.707 (1.451–2.008) ** | 2.086 (1.617–2.690) ** |
| 1000–3000 (887–2663 USD) | 1.337 (1.155–1.548) ** | 1.552 (1.225–1.965) ** | |
| 3000+ (2663 USD+) | Reference | Reference | |
| Comorbidity prevalence | No | 0.743 (0.672–0.822) ** | 0.835 (0.723–0.965) ** |
| Yes | Reference | Reference | |
| Labor market participation | No | 0.874 (0.777–0.982) * | 1.384 (1.144–1.675) ** |
| Yes | Reference | Reference | |
| Cigarette Smoker | Current | 1.578 (1.304–1.910) ** | 1.520 (1.153–2.003) * |
| Former | 0.951 (0.804–1.125) | 1.064(1.064–0.831) | |
| Never smoked | Reference | Reference | |
| Alcohol consumer | No | 1.092 (0.984–1.211) | 1.226 (1.052–1.429) * |
| Yes | Reference | Reference | |
| Moderate physical activity (day/week) | 0 | 1.058 (0.915–1.223) | 1.237 (0.983–1.557) |
| 1–3 | 1.055 (0.872–1.278) | 1.309 (0.976–1.755) | |
| 4+ | Reference | Reference | |
| Regular social activity (monthly) | No | 1.551 (1.401–1.717) ** | 1.455 (1.255–1.688) ** |
| Yes | Reference | Reference | |
| Unadjusted Model | Adjusted | |||
|---|---|---|---|---|
| Model 1 | Model 2 (a) | Model 2 (b) | ||
| Self-Rated Stress Levels (n = 11,408) | ||||
| 1st quartile (≤2.73%) | 0.944 ** (0.825–1.081) | 0.945 * (0.823–1.085) | 0.931 ** (0.811–1.070) | 1.163 (0.750–1.804) |
| 2nd quartile (2.74–5.72%) | 1.192 ** (1.046–1.359) | 1.188 * (1.039–1.358) | 1.183 ** (1.034–1.353) | 1.451 (0.946–2.227) |
| 3rd quartile (5.73–9.79%) | 0.998 ** (0.874–1.140) | 1.026 * (0.896–1.175) | 1.022 ** (0.892–1.171) | 1.492 (0.987–2.256) |
| 4th quartile (≥9.8%) | Reference | Reference | Reference | Reference |
| p-value for trend | <0.005 | <0.01 | <0.005 | 0.191 |
| 1st quartile (≤2.73%) | 0.730 ** (0.590–0.902) | 0.740 *** (0.597–0.918) | 0.727 *** (0.586–0.902) | 0.742 (0.369–1.491) |
| 2nd quartile (2.74–5.72%) | 1.276 ** (1.057–1.542) | 1.279 *** (1.055–1.550) | 1.280 *** (1.047–1.540) | 0.820 (0.425–1.583) |
| 3rd quartile (5.73–9.79%) | 1.218 ** (1.009–1.471) | 1.274 *** (1.052–1.543) | 1.269 *** (1.056–1.541) | 1.131 (0.615–2.081) |
| 4th quartile (≥9.8%) | Reference | Reference | Reference | Reference |
| p-value for trend | <0.005 | <0.0001 | <0.0001 | 0.561 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.J.; Lee, D.K. Do Sociodemographic Factors and Urban Green Space Affect Mental Health Outcomes Among the Urban Elderly Population? Int. J. Environ. Res. Public Health 2019, 16, 789. https://doi.org/10.3390/ijerph16050789
Lee HJ, Lee DK. Do Sociodemographic Factors and Urban Green Space Affect Mental Health Outcomes Among the Urban Elderly Population? International Journal of Environmental Research and Public Health. 2019; 16(5):789. https://doi.org/10.3390/ijerph16050789
Chicago/Turabian StyleLee, Hyun Jin, and Dong Kun Lee. 2019. "Do Sociodemographic Factors and Urban Green Space Affect Mental Health Outcomes Among the Urban Elderly Population?" International Journal of Environmental Research and Public Health 16, no. 5: 789. https://doi.org/10.3390/ijerph16050789
APA StyleLee, H. J., & Lee, D. K. (2019). Do Sociodemographic Factors and Urban Green Space Affect Mental Health Outcomes Among the Urban Elderly Population? International Journal of Environmental Research and Public Health, 16(5), 789. https://doi.org/10.3390/ijerph16050789