1. Introduction
The monitoring of air quality in Poland over the past two years indicated the occurrence of two winter smog episodes, with the first occurring during the period between 4 January and 8 January 2016 and the second between 7 January and 11 January 2017 [
1]. Both of these winter smog episodes were an important public health issue which induced a great concern among residents, particularly the inhabitants of Silesian Voivodeship, an urbanized, historical, and coal mining industrial region located in southern Poland with over 3.8 million people [
2]. Therefore, it is justifiable to estimate the actual relationship between the rapidly worsening air quality during winter smog episodes and the exacerbation of respiratory diseases among the exposed population. The obtained results are necessary for the environmental health risk communication and will prove to be a useful indicator for the implementation of the necessary health policy actions in the region. Episodes of winter smog in Poland occur every year, especially during the colder winter season. The level of environmental health perception in the country is understandably categorized as one of the lowest in Europe. However, contemporary media outlets have publicized and sensationalized the problem, leading to widespread panic among inhabitants. The situation is particularly difficult in the Silesia, a region where coal is mined and many people are employed in the mining industry. Our task is to document the relationship between the emerging hazard and the health of the population and communicate the risk based on reliable evidence. We believe that the results of our study will help to improve the inhabitants’ knowledge on the real hazard, and will reinforce the social activity needed to improve the quality of the environment. Among the well-described pulmonary adverse health effects associated with air pollution are short-term effects such as inflammatory reactions of the lungs and bronchi, and respiratory symptoms (coughing, wheezing, and problems with breathing). Additionally, increases in daily hospitalization, respiratory mortality, and increases in the usage of medications were reported [
3]. The available data point to a significant increase in sales of medicaments used to treat exacerbations of respiratory diseases in the cold season, with a maximum in January and February [
4]. This is similar to other countries, where a relationship between the concentration of fine particulate matter (PM
2.5) and daily mortality due to respiratory diseases were observed [
5,
6,
7]. Typically in environmental epidemiology, the moving average or temporal lags are used as a measure of exposure during the estimation of the concentration–response effects [
8,
9].
The aim of this study was to assess the relationship between daily concentrations of fine particulate matter in ambient air and exacerbations of respiratory diseases registered in the period from 1 January 2016 to 31 August 2017 in the central agglomeration area (CAA) of the Silesian Voivodeship, a southern region in Poland.
2. Materials and Methods
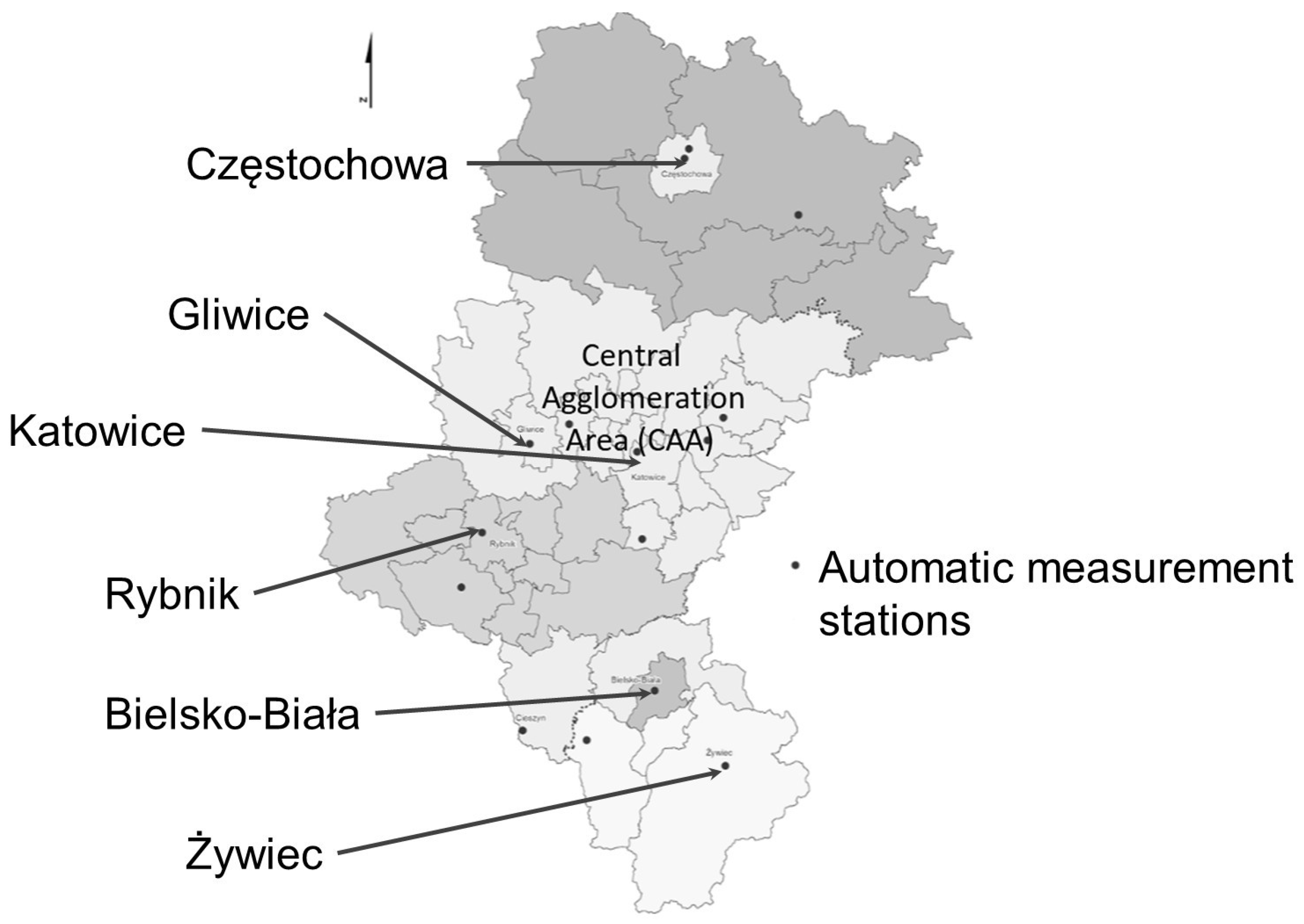
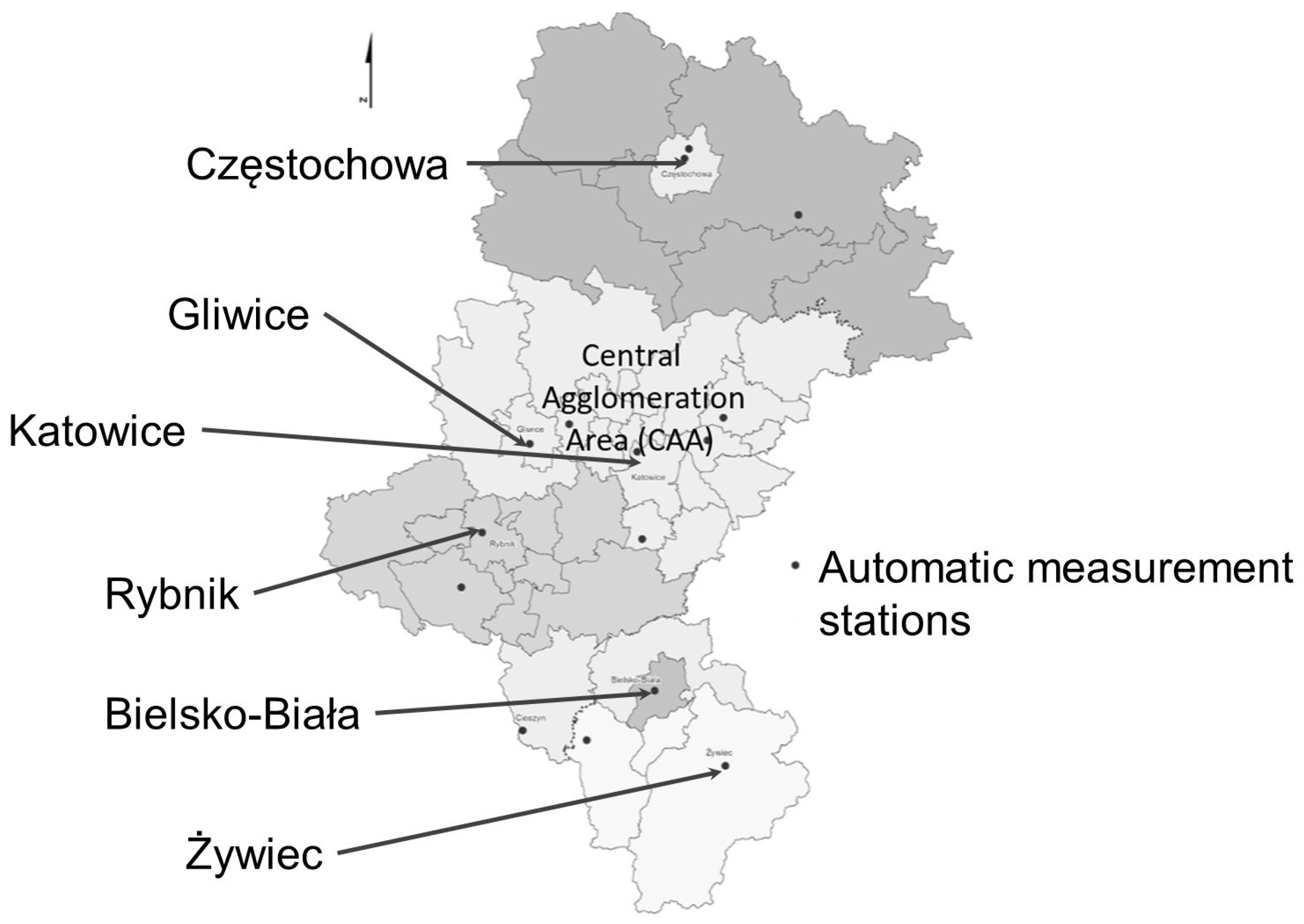
Secondary epidemiological data of daily registered outpatient visits or hospitalizations of Silesian inhabitants due to total respiratory diseases (J00–J99 by ICD-10) in the study period (1 January 2016 to 31 August 2017) were obtained from the National Health Fund database in Katowice. The original data included the entire Silesian Voivodeship, however, the final database was limited to the central agglomeration area (CAA) with a population of 2,429,471 inhabitants (2015 year) and an area of 3337 km
2. The total number of outpatient visits due to respiratory diseases in the study period was 3,550,901 and the total number hospitalizations was 60,346. CAA included the Upper Silesia Agglomeration and the central part of the Silesian zone with the following powiats: Będzin, Zawiercie, Tarnowskie Góry, Gliwice, and Bieruń-Lędziny counties. This decision was a consequence of the need to maintain consistency with the health data on air quality and to relate it with the real existing definition of CAA in the previous system of prognosis of the air quality index. It was defined at a website which existed until 1 January 2019.
Figure 1 presents the location of CAA in the Silesian Voivodeship.
Air pollution and meteorological data in the study period, including daily concentration of SO
2, NO
2, NO
x, ozone, and CO in ambient air, as well as daily temperature, relative humidity, and atmospheric pressure, were gathered from the Provincial Inspectorate of Environmental Protection in Katowice database [
1]. Daily average concentrations of PM
2.5 and PM
10 (particles with an aerodynamic diameter less or equal 2.5 and 10 micrometers, respectively) were available only from two automatic measuring stations (urban background): in Katowice at Kossutha str. and in Gliwice at Gallus str. (out of all 15 stations located in the region). Because of very high correlation coefficients between daily averages recorded at both stations (
r = 0.93,
r = 0.90, and
r = 0.99, for PM
2.5, SO
2, and ambient air daily air temperature or relative air humidity, respectively) values from Katowice station were used in the further analysis of the measurements. Moreover, a similarly high correlation was obtained for the other pollutants measured in Katowice and in other stations located in the study region (CAA) and in characterizing the agglomeration of the urban background [
4].
To assess the relationship between ambient air pollution and the number of outpatient visits or hospitalizations due to respiratory diseases, the multivariable log-linear Poisson regression model was used. The model was linked with Equation (1):
where E(ND) is the observed daily number of outpatient visits or hospitalizations (dependent variable), X is a vector of independent variables (daily concentration of particulate matter, daily meteorological conditions, the season of the year, influenza episodes, and weekend days), and β means the calculated regression coefficient. The variables describing ambient air pollutant were expressed first as 1, 3, 5, 7, 14, and 30-day moving averages of PM
10 and PM
2.5 concentrations. Next, the exposure was expressed as a temporal lag of 1, 3, 5, 7, 14, and 30 days of outpatient visits or hospitalization. The confounding factors like daily average air temperature, relative humidity, atmospheric pressure, season (according to astronomical seasons), and week days (working day vs. holiday), but only for outpatient visits, were included in the model. Moreover, there was no observed influenza epidemic in the study period. Results of the model were presented by the relative risk (RR) of respiratory effect related to the increase in concentration of PM
10 or PM
2.5 by interquartile range (IQR) and were calculated using Equation (2):
where β is the regression coefficient and delta is the IQR. The level of statistical significance used was α = 0.05. Calculations were conducted using SAS version 9.4 (SAS Institute Inc., Cary, North Carolina, USA).
3. Results
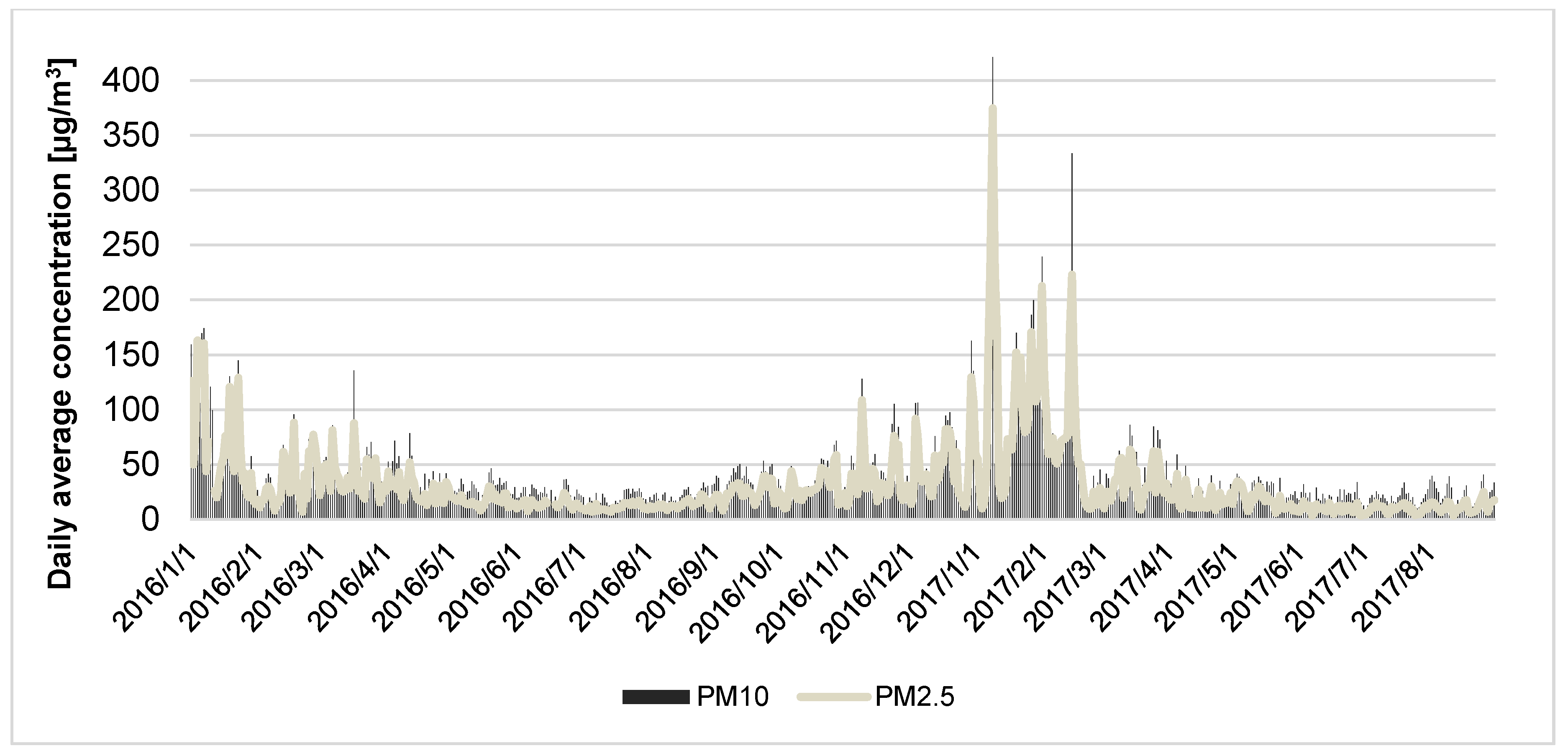
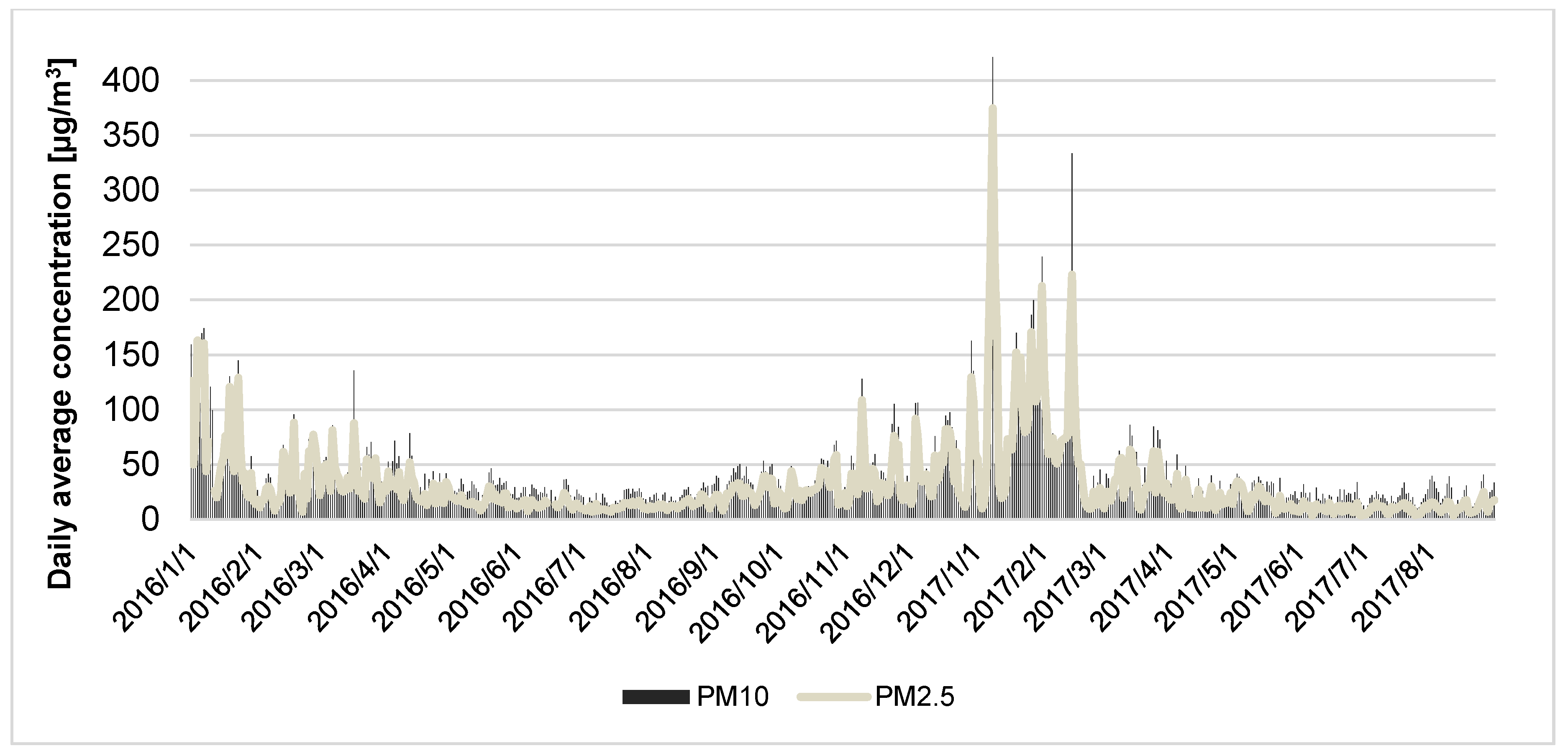
The study results confirmed the significant worsening of the ambient air quality during cold seasons in the study region (central area of Silesian Voivodeship, Poland), with the occurrence of two winter smog episodes in the study period. Both of the smog episodes were in January—the first one occurred from 4 January 2016 to 7 January 2016 and the second one from 7 January 2017 to 11 January 2017. In the second period, the temperature of ambient air was very low and the concentration of particulate matter was the highest. Median and IQR values for PM2.5 and PM10 concentrations in winter time were 44 (49.0) µg/m3 and 52.58 (53.22) µg/m3, respectively.
Figure 2 shows the daily mean concentration of PM
2.5 and PM
10 measured in the study region between 1 January 2016 and 31 August 2017. The highest concentration of fine particulate matter was observed in the winter season of 2016/2017. In the time period from January 2017 until March 2017 the daily mean concentrations of PM
10 were higher than 150 µg/m
3 on 17 days, and daily mean concentrations of PM
2.5 were higher than 100 µg/m
3 on 20 days.
Table 1 shows the seasonal variability of air pollutants as well as the daily mean of the health outcomes occurring (hospitalization, outpatient visits) stratified for different seasons. The highest number of registered outpatient visits and hospitalizations due to respiratory diseases (codes J00–J99 according to ICD-10) was also observed in the cold season of 2016 and 2016/2017, with median values of 9664.5 (10,746.5) and 136 (69.5), respectively.
In
Table 2, the Spearman correlation coefficients between air pollutants and meteorological conditions measured at the two monitoring sites in Katowice and Gliwice are shown. A strong positive and statistically significant correlation between PM
10 and PM
2.5 concentration and other measured pollutants such as NO
2, NO
x, and CO was observed. A negative and also statistically significant correlation was noted for particulate matters and temperature, wind speed, or ozone concentrations. Higher values of relative humidity significantly increased the concentration of fine particles (PM
2.5), whereas the effect in the case of PM
10 was a bit lower. Moreover, the dominant direction of the wind was the west direction (49.5%), followed by the south (20.5%) and east (20.5%) direction.
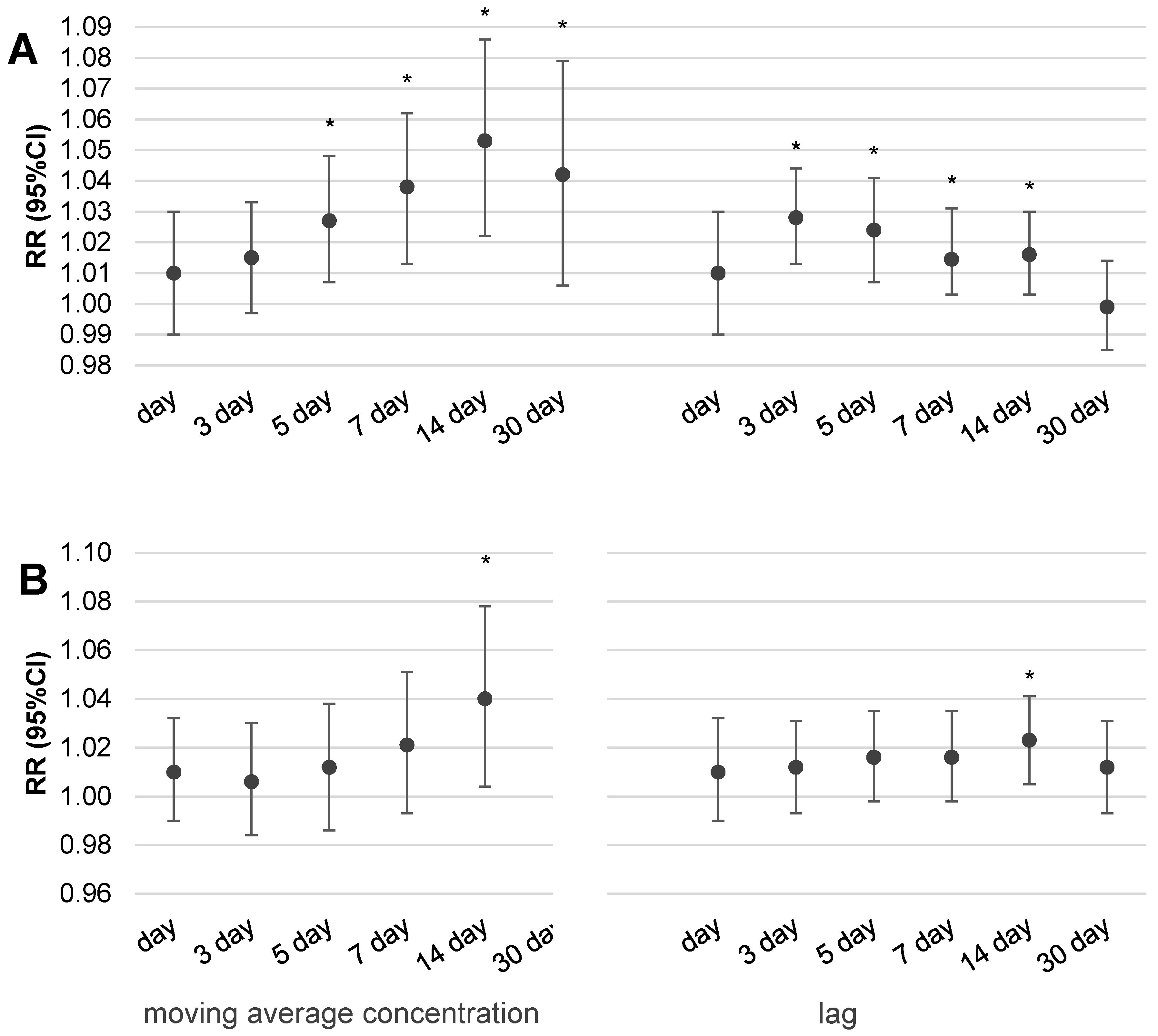
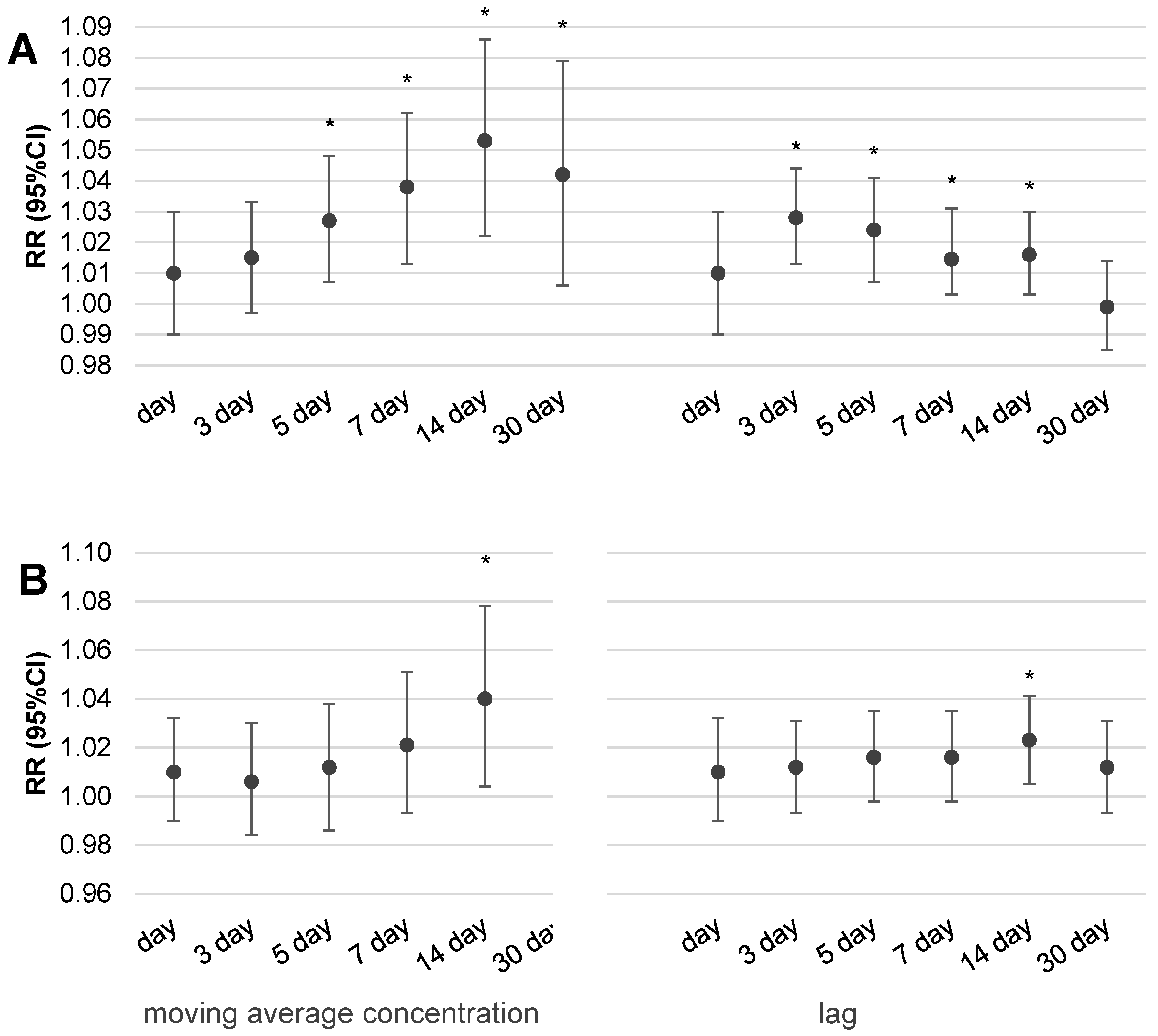
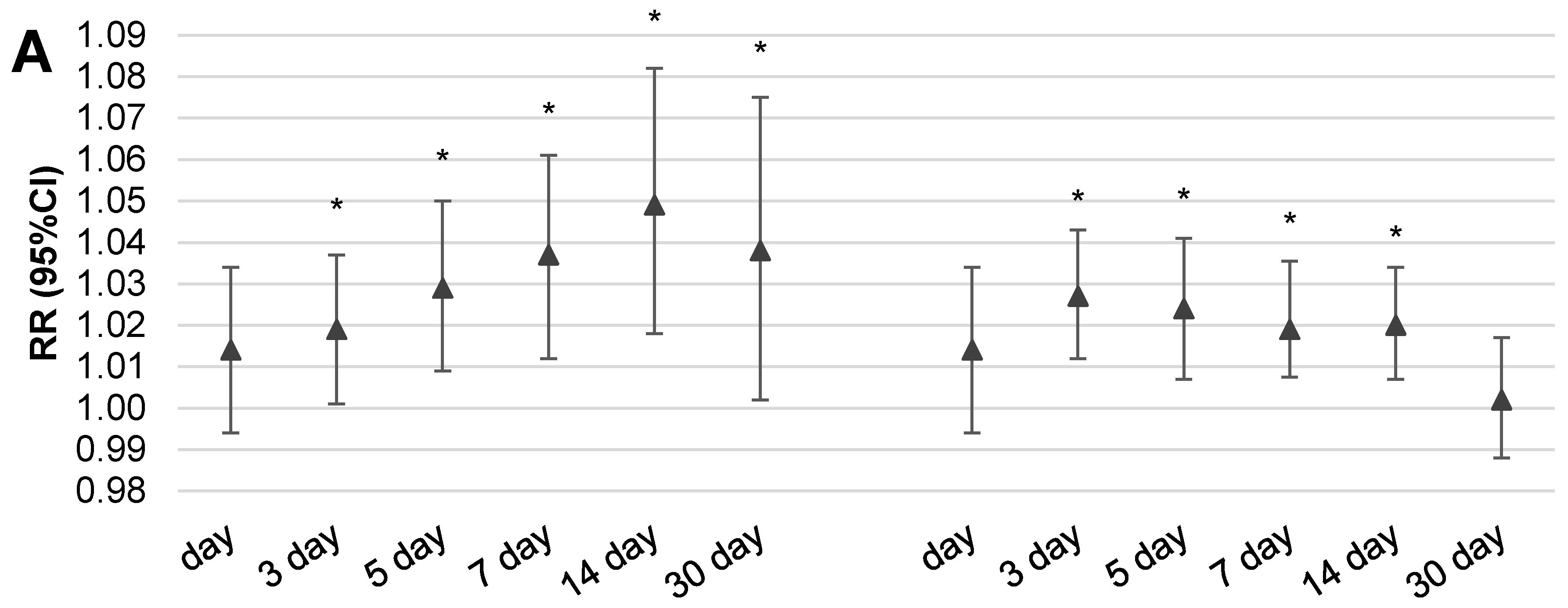
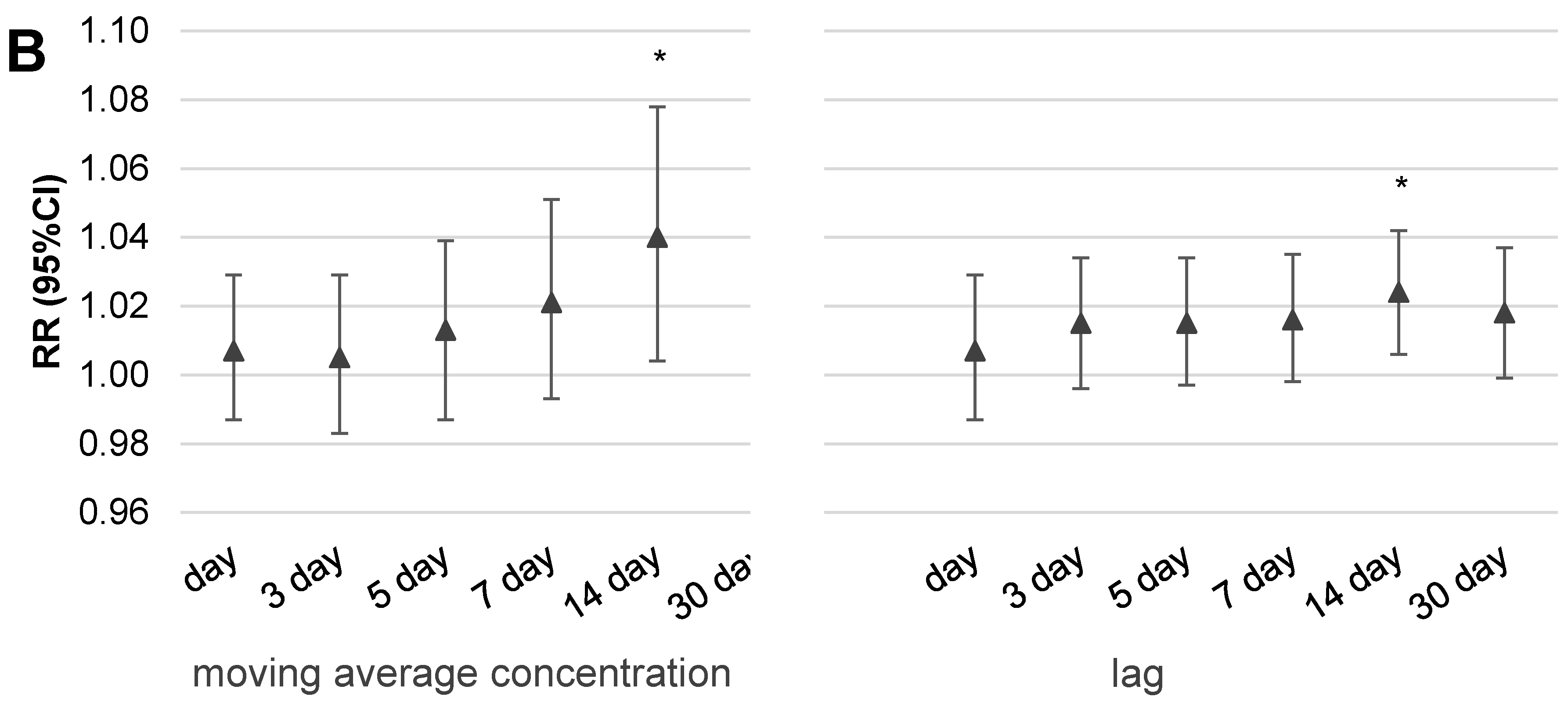
Figure 3 and
Figure 4 illustrate the results of the multivariable analysis assessing the risk ratio of daily outpatient visits (A) or hospitalization (B) due to respiratory disorders related to the increase of fine particulate matter concentrations by IQR value (24.5 µg/m
3 for PM
10 and 22.5 µg/m
3 for PM
2.5) in two scenarios of exposure: expressed by the moving average concentration or related to a temporal lag of health effect.
It is interesting that statistically significant increases of health effects (both outpatient visits and hospitalizations) were observed in the case of dose expressed by two-week moving average concentrations. Despite the fact that we observed an increase in respiratory health effects related to an increase in particulate matter concentration by IQR, the pattern is a bit different for outpatient visits than in the case of hospitalizations. It was noticed that the 14-day moving average concentration of particulate matter was responsible for the highest risk of outpatient visits, RR = 1.049 (95%CI: 1.017–1.084) for PM2.5 and RR = 1.053 (95%CI: 1.022–1.086) for PM10, respectively. Moreover, both values were statistically significant. A similar observation was also seen in hospitalizations and 14-day moving average concentrations of PM10, however, the highest risk was observed for 30-day moving average concentrations of pollution, RR = 1.054 (95%CI: 1.009–1.099) for PM2.5 and RR = 1.053 (95%CI: 1.01–1.097) for PM10. In the case of the moving average concentration of PM10, a more evident respiratory effect was related with longer time of exposure and a statistically significant effect was obtained for 14-day moving average concentrations for both outpatient visits and hospitalizations. A similar relation was observed for PM2.5; the greatest and statistically significant risk was observed for two-week moving average concentrations in the case of outpatient visits as well as hospitalizations. In conclusion, we have to underline that the obtained risk ratios were small, as an increase of PM10 or PM2.5 concentration by IQR value increased the risk of outpatient visits or hospitalizations due to respiratory diseases by, on average, 2–5%.
The pattern of concentration–response effect in the case of exposure expressed by the temporal lag of health effects in relation to measuring day is a bit different. In the case of outpatient visits, the highest and statistically significant risk was observed with three or even five days lag after exposure for both pollutants, PM2.5 and PM10. In the case of hospitalizations, significant health effect was noted only for two-week lags of exposure. The highest risks related with PM2.5 were as follows: RR = 1.024 (95%CI: 1.004–1.044) for 14-day lags in hospitalizations and RR = 1.027 (95%CI: 1.01–1.043) for 3-day lags in the case of outpatient visits.
4. Discussion
The highest levels of air pollutants in the CAA occurred during the winter season (especially in January 2016 and 2017). This observation is similar to those reported from other countries, where the worst quality of ambient air is found in the cold season [
10,
11]. A major source of PM emission in winter in Poland remains outdated individual heating stoves in which people burn poor quality coal, biomass, or even garbage [
4,
12]. Numerous educational campaigns that have been raised for many years in an effort to improve the risk perception of environmental health hazards have failed to bring significant results in Poland—especially in the study region, because the major source of energy used for industrial production and house heating is coal combustion [
3]. The principal reason for such behavior is energy poverty, and a low awareness of the risks persists in the population. A significant contribution to emissions and human exposure also comes from road transport, which has rapidly increased in the last decade in the study region [
13].
Simultaneously, we observed that the highest number of outpatient visits and hospitalizations due to respiratory diseases (codes J00–J99 according to ICD-10) were evident during the coldest season. In the case of hospitalizations, the median number of patients during winter was approximately 2 times higher than in summer (136.0 vs. 79.5), and in the case of outpatient visits, the disparity was even higher (9664.5 vs. 2983). It is worth mentioning that forecasting, risk communication about the necessity of reducing emissions from individual heating stoves and medical services activation were the most effective in eliminating the harmful health consequences of winter smog conditions in the UK [
11]. Available data suggest that improving air quality and reducing haze days in Beijing would benefit health, potentially resulting in reductions in the number of hospital emergency room visits due to respiratory diseases [
14]. Current air quality in the central agglomeration area of Silesian Voivodeship is quite similar to those observed in China, probably because of the similarity of the sources of energy and heat production.
Another important issue in environmental epidemiology studies is the method of exposure estimation [
15]. Usually, researchers assess the short-term health effects relating to increases in air pollutant concentration by the moving average concentration of pollution [
16,
17] or temporal lags (1–30 days) as a measure of exposure [
18,
19,
20]. Commonly used models assess the risk ratio of health effects in response to an increase in pollutant concentration by a unit of a single IQR value. Our intention was, inter alia, to recognize which type of accepted method of the exposure presentation better reflects the concentration–response function in the Silesian province. The results from our study confirmed that the moving average concentration was better suited for the modelling of biological response as a result of PM
2.5 or PM
10 exposure. Evidently, each increase of dose expressed in the form of moving average concentration over a longer time (up to 2 weeks) leads to a slow increase in the daily number of outpatient visits or hospitalizations due to respiratory effects. The picture of the concentration–effect relationship assessed by the lag of health effect was not so clear. In the case of outpatient visits, the highest and statistically significant risk was observed with three or even five days lag after exposure for both pollutants, PM
10 and PM
2.5. In the case of hospitalizations, a significant health effect was noted only for two weeks lag of exposure. We observed an increase in health risk in relation to longer exposure times expressed by two or even four weeks moving average concentrations. The second way of exposure calculation (by temporal lag) also suggests an increase of outpatient visits and hospitalizations related to a longer time of exposure. It seems logical that, initially, people manage themselves in consultation with their doctor and in the absence of improvement they are hospitalized. Such an observation is in line with the well-known ‘air pollution health pyramid’ concept, where the effects have ranged from subtle subclinical effects through pharmaceutic usage and doctor consultancy to premature death [
21]. It should be emphasized that the value of the estimated risk of respiratory hospitalization or outpatient visits related to an increase in particulate matter concentration depends on the method chosen to measure the exposure. However, it should be noted that regardless of the exposure presentation form, the statistically significant short-term effects of particulate matter exposure, manifested in ambulatory visits or hospital admissions due to the respiratory problem, was associated with a two-week exposure.
One limitation of this study is the secondary character of health data, which were obtained from the current system of National Health Found registration. It is impossible to rule out misdiagnosed cases, although in this paper we included only the number of diagnoses due to total respiratory diseases (codes J00–J99 according to ICD-10). Another issue is the applied exposure presentation as daily average values for the central agglomeration area without individual exposure data. However, this method, although imperfect, is often used in ecological epidemiological studies, mostly in regions where no individual PM
2.5 or PM
10 data are available. The use of one or several fixed monitoring stations is a common method of exposure estimation in short-term studies on health effects including mortality or morbidity [
22,
23]. Estimation of personal exposure might be better; however, the high cost of personal measurements makes it difficult to apply this approach for exposure estimation of a large population [
24].

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}