An Evaluation of a Low-Intensity Cognitive Behavioral Therapy mHealth-Supported Intervention to Reduce Loneliness in Older People



Abstract
1. Introduction and Background
2. mLINCC—A LI-CBT Intervention Supported by WhatsApp
3. Methodology
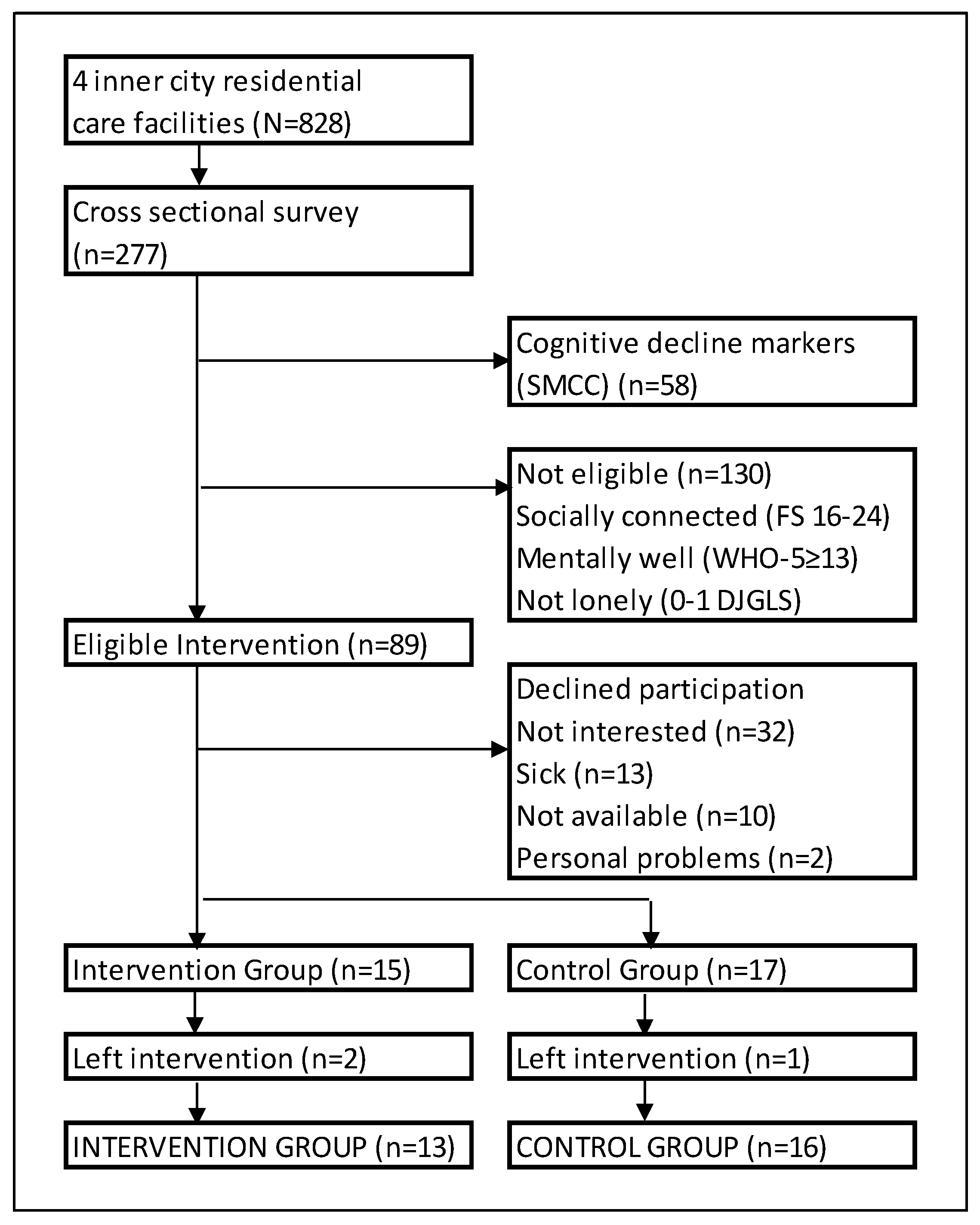
4. Results
Demographics
5. Discussion
6. Conclusions
7. Recommendations
8. Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Du Toit, S.H.J.; Böning, W.; Van Der Merwe, T.R. Dignity and Respect: Facilitating Meaningful Occupation for SeSotho Elders. Scand. J. Occup. Ther. 2014, 21, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Grenade, L.; Boldy, D. Social Isolation and Loneliness among Older People: Issues and Future Challenges in Community and Residential Settings. Aust. Heal. Rev. 2008, 32, 468–478. [Google Scholar] [CrossRef]
- Shklovski, I.; Kraut, R.; Cummings, J. Keeping in Touch by Technology. In Proceedings of the Twenty-Sixth Annual CHI Conference on Human Factors in Computing Systems—CHI ’08, Florence, Italy, 5–10 April 2008; ACM Press: New York, NY, USA, 2008; pp. 807–816. [Google Scholar] [CrossRef]
- Chipps, J.; Jarvis, M.A. Social Capital and Mental Well-Being of Older People Residing in a Residential Care Facility in Durban, South Africa. Aging Ment. Health 2016, 20, 1264–1270. [Google Scholar] [CrossRef]
- Franck, L.; Molyneux, N.; Parkinson, L. Systematic Review of Interventions Addressing Social Isolation and Depression in Aged Care Clients. Qual. Life Res. 2016, 25, 1395–1407. [Google Scholar] [CrossRef]
- Drageset, J.; Kirkevold, M.; Espehaug, B. Loneliness and Social Support among Nursing Home Residents without Cognitive Impairment: A Questionnaire Survey. Int. J. Nurs. Stud. 2011, 48, 611–619. [Google Scholar] [CrossRef] [PubMed]
- de Jong Gierveld, J. Developing and Testing a Model of Loneliness. J. Pers. Soc. Psychol. 1987, 53, 119–128. [Google Scholar] [CrossRef]
- Mann, F.; Bone, J.K.; Lloyd-Evans, B.; Frerichs, J.; Pinfold, V.; Ma, R.; Wang, J.; Johnson, S. A Life Less Lonely: The State of the Art in Interventions to Reduce Loneliness in People with Mental Health Problems. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 627–638. [Google Scholar] [CrossRef]
- Masi, C.M.; Chen, H.-Y.; Hawkley, L.C.; Cacioppo, J.T. A Meta-Analysis of Interventions to Reduce Loneliness. Personal. Soc. Psychol. Rev. 2011, 15, 219–266. [Google Scholar] [CrossRef] [PubMed]
- Kennerley, H.; Kirk, J.; Westbrook, D. An Introduction to Cognitive Behaviour Therapy: Skills and Applications, 3rd ed.; SAGE Publications: London, UK, 2016. [Google Scholar]
- Friedler, B.; Crapser, J.; McCullough, L. One Is the Deadliest Number: The Detrimental Effects of Social Isolation on Cerebrovascular Diseases and Cognition. Acta Neuropathol. 2015, 129, 493–509. [Google Scholar] [CrossRef]
- Chen, Y.-R.R.; Schulz, P.J. The Effect of Information Communication Technology Interventions on Reducing Social Isolation in the Elderly: A Systematic Review. J. Med. Internet Res. 2016, 18, e18. [Google Scholar] [CrossRef]
- Choi, M.; Kong, S.; Jung, D. Computer and Internet Interventions for Loneliness and Depression in Older Adults: A Meta-Analysis. Healthc. Inform. Res. 2012, 18, 191–198. [Google Scholar] [CrossRef]
- Chipps, J.; Jarvis, M.A.; Ramlall, S. The Effectiveness of E-Interventions on Reducing Social Isolation in Older Persons: A Systematic Review of Systematic Reviews. J. Telemed. Telecare 2017, 23, 817–827. [Google Scholar] [CrossRef]
- Chiang, K.; Chu, H.; Chang, H.; Chung, M.; Chen, C.; Chiou, H.; Chou, K. The Effects of Reminiscence Therapy on Psychological Well-Being, Depression, and Loneliness among the Institutionalized Aged. Int. J. Geriatr. Psychiatry 2010, 25, 380–388. [Google Scholar] [CrossRef]
- Poscia, A.; Stojanovic, J.; La Milia, D.I.; Duplaga, M.; Grysztar, M.; Moscato, U.; Onder, G.; Collamati, A.; Ricciardi, W.; Magnavita, N. Interventions Targeting Loneliness and Social Isolation among the Older People: An Update Systematic Review. Exp. Gerontol. 2018, 102, 133–144. [Google Scholar] [CrossRef]
- Bourassa, K.J.; Memel, M.; Woolverton, C.; Sbarra, D.A. Social Participation Predicts Cognitive Functioning in Aging Adults over Time: Comparisons with Physical Health, Depression, and Physical Activity. Aging Ment. Health 2017, 21, 133–146. [Google Scholar] [CrossRef]
- Kuiper, J.S.; Zuidersma, M.; Oude Voshaar, R.C.; Zuidema, S.U.; van den Heuvel, E.R.; Stolk, R.P.; Smidt, N. Social Relationships and Risk of Dementia: A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. Ageing Res. Rev. 2015, 22, 39–57. [Google Scholar] [CrossRef]
- van Bel, D.T.; Smolders, K.C.H.J.; Ijsselsteijn, W.A.; de Kort, Y. Social Connectedness: Concept and Measurement. Intell. Environ. 2009, 2, 67–74. [Google Scholar] [CrossRef]
- Cornwell, E.Y.; Waite, L.J. Social Disconnectedness, Perceived Isolation, and Health among Older Adults. J. Health Soc. Behav. 2009, 50, 31–48. [Google Scholar] [CrossRef]
- Ongun, E.; Guder, F.Z.; Demirag, A. Elderly People’s Choice of Media and Their Perceived State of Loneliness. Online J. Commun. Media Technol. 2016, 6, 35–47. [Google Scholar]
- Pew Research Center. Older Adults and Technology Use; Pew Research Center: Washington, DC, USA, 2014. [Google Scholar]
- World Health Organization (WHO). BE HE@LTHY BE MOBILE A Handbook on How to Implement MAgeing; World Health Organisation: Geneva, Switzerland, 2018. [Google Scholar]
- Goswami, S.; Kobler, F.; Leimeister, J.M.; Krcmar, H. Using Online Social Networking to Enhance Social Connectedness and Social Support for the Elderly. In Proceedings of the International Conference on Information Systems, ICIS 2010, Saint Louis, MO, USA, 12–15 December 2010. [Google Scholar]
- Broady, T.; Chan, A.; Caputi, P. Comparison of Older and Younger Adults’ Attitudes towards and Abilities with Computers: Implications for Training and Learning. Br. J. Educ. Technol. 2010, 41, 473–485. [Google Scholar] [CrossRef]
- Officer, A.; Schneiders, M.L.; Wu, D.; Nash, P.; Thiyagarajan, J.A.; Beard, J.R. Valuing Older People: Time for a Global Campaign to Combat Ageism. Bull. World Health Organ. 2016, 94, 710–710A. [Google Scholar] [CrossRef]
- Chen, K.; Chan, A.H.S. Gerontechnology Acceptance by Elderly Hong Kong Chinese: A Senior Technology Acceptance Model (STAM). Ergonomics 2014, 57, 635–652. [Google Scholar] [CrossRef]
- van Biljon, J.; Renaud, K. A Qualitative Study of the Applicability of Technology Acceptance Models to Senior Mobile Phone Users. In International Conference on Conceptual Modeling; Springer: Barcelona, Spain, 2008; pp. 228–237. [Google Scholar]
- Kuerbis, A.; Mulliken, A.; Muench, F.; Moore, A.; Gardner, D. Older Adults and Mobile Technology: Factors That Enhance and Inhibit Utilization in the Context of Behavioral Health. Ment. Heal. Addict. Res. 2017, 2, 1–11. [Google Scholar] [CrossRef]
- Lee, C.; Coughlin, J.F. PERSPECTIVE: Older Adults’ Adoption of Technology: An Integrated Approach to Identifying Determinants and Barriers. J. Prod. Innov. Manag. 2015, 32, 747–759. [Google Scholar] [CrossRef]
- Aarts, S.; Peek, S.T.M.; Wouters, E.J.M. The Relation between Social Network Site Usage and Loneliness and Mental Health in Community-Dwelling Older Adults. Int. J. Geriatr. Psychiatry 2015, 30, 942–949. [Google Scholar] [CrossRef]
- Dickens, A.P.; Richards, S.H.; Greaves, C.J.; Campbell, J.L. Interventions Targeting Social Isolation in Older People: A Systematic Review. BMC Public Health 2011, 11, 647. [Google Scholar] [CrossRef]
- O’Rourke, H.M.; Collins, L.; Sidani, S. Interventions to Address Social Connectedness and Loneliness for Older Adults: A Scoping Review. BMC Geriatr. 2018, 18, 214. [Google Scholar] [CrossRef]
- Jarvis, M.A.; Padmanabhanunni, A.; Balakrishna, Y.; Chipps, J. The Effectiveness of Interventions Addressing Loneliness in Older Persons: An Umbrella Review of Systematic Reviews and Meta-Analysis. In Submit.
- Cattan, M.; White, M.; Bond, J.; Learmouth, A. Preventing Social Isolation and Loneliness among Older People: A Systematic Review of Health Promotion Interventions. Ageing Soc. 2005, 25, 41–67. [Google Scholar] [CrossRef]
- Kazantzis, N.; Pachana, N.A.; Secker, D.L. Cognitive Behavioral Therapy for Older Adults: Practical Guidelines for the Use of Homework Assignments. Cogn. Behav. Pract. 2003, 10, 324–332. [Google Scholar] [CrossRef]
- Slegers, K.; van Boxtel, M.P.J.; Jolles, J. Effects of Computer Training and Internet Usage on the Well-Being and Quality of Life of Older Adults: A Randomized, Controlled Study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2008, 63, P176–P184. [Google Scholar] [CrossRef]
- Ramlall, S.; Chipps, J.; Bhigjee, A.I.; Pillay, B.J. The Sensitivity and Specificity of Subjective Memory Complaints and the Subjective Memory Rating Scale, Deterioration Cognitive Observee, Mini-Mental State Examination, Six-Item Screener and Clock Drawing Test in Dementia Screening. Dement. Geriatr. Cogn. Disord. 2013, 36, 119–135. [Google Scholar] [CrossRef]
- Hawthorne, G. Measuring Social Isolation in Older Adults: Development and Initial Validation of the Friendship Scale. Soc. Indic. Res. 2006, 77, 521–548. [Google Scholar] [CrossRef]
- de Jong Gierveld, J.; van Tilburg, T.G. The De Jong Gierveld Short Scales for Emotional and Social Loneliness: Tested on Data from 7 Countries in the UN Generations and Gender Surveys. Eur. J. Ageing 2010, 7, 121–130. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Rijkeboer, M.M.; van den Bergh, H.; van den Bout, J. Stability and Discriminative Power of the Young Schema-Questionnaire in a Dutch Clinical versus Non-Clinical Population. J. Behav. Ther. Exp. Psychiatry 2005, 36, 129–144. [Google Scholar] [CrossRef]
- Lyrakos, D.G. The Validity of Young Schema Questionnaire 3rd Version and the Schema Mode Inventory 2nd Version on the Greek Population. Psychology 2014, 05, 461–477. [Google Scholar] [CrossRef]
- Baranoff, J.; Oei, T.P.S.; Cho, S.H.; Kwon, S.-M. Factor Structure and Internal Consistency of the Young Schema Questionnaire (Short Form) in Korean and Australian Samples. J. Affect. Disord. 2006, 93, 133–140. [Google Scholar] [CrossRef]
- Phillips, K.; Brockman, R.; Bailey, P.E.; Kneebone, I.I. Young Schema Questionnaire—Short Form Version 3 (YSQ-S3): Preliminary Validation in Older Adults. Aging Ment. Health 2017, 1–8. [Google Scholar] [CrossRef]
- Penning, M.J.; Liu, G.; Chou, P.H.B. Measuring Loneliness among Middle-Aged and Older Adults: The UCLA and de Jong Gierveld Loneliness Scales. Soc. Indic. Res. 2014, 118, 1147–1166. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO-Five Well-being Index (WHO-5). Available online: https://www.psykiatri-regionh.dk/who-5/Documents/WHO5_English.pdf (accessed on 16 July 2015).
- Gao, Q.; Ebert, D.; Chen, X.; Ding, Y. Design of a Mobile Social Community Platform for Older Chinese People in Urban Areas. Hum. Factors Ergon. Manuf. 2015, 25, 66–89. [Google Scholar] [CrossRef]
- Leung, R.; Tang, C.; Haddad, S.; Mcgrenere, J.; Graf, P.; Ingriany, V. How Older Adults Learn to Use Mobile Devices: Survey and Field Investigatons. ACM Trans. Access. Comput. 2012, 4, 1–33. [Google Scholar] [CrossRef]
- van Dyk, T.; Renaud, K.; van Biljon, J. Moses—Method for Selecting Senior Mobile Phones: Supporting Design & Choice for the Elderly. In Proceedings of the South African Institute for Computer Scientists and Information Technologists Conference SAICSIT ’12, Pretoria, South Africa, 1–3 October 2012; ACM Press: New York, NY, USA, 2012; pp. 277–285. [Google Scholar] [CrossRef]
- Tsai, H.-H.; Tsai, Y.-F.; Wang, H.-H.; Chang, Y.-C.; Chu, H.H. Videoconference Program Enhances Social Support, Loneliness, and Depressive Status of Elderly Nursing Home Residents. Aging Ment. Health 2010, 14, 947–954. [Google Scholar] [CrossRef]
- Oei, T.P.S.; Baranoff, J. Young Schema Questionnaire: Review of Psychometric and Measurement Issues. Aust. J. Psychol. 2007, 59, 78–86. [Google Scholar] [CrossRef]
- de Jong Gierveld, J.; van Tilburg, T.G. A 6-Item Scale for Overall, Emotional, and Social Loneliness. Res. Aging 2006, 28, 582–598. [Google Scholar] [CrossRef]
- Heylen, L. The Older, the Lonelier? Risk Factors for Social Loneliness in Old Age. Ageing Soc. 2010, 30, 1177–1196. [Google Scholar] [CrossRef]
- Mmotlane, R.; Struwig, M.; Roberts, B. The Glue That Binds or Divides: Social Trust in South Africa. Hum. Sci. Res. Counc. 2010, 8, 4–5. [Google Scholar]
- Edwards, L.M. Ideational Social Capital and the Civic Culture: Extricating Putnam’s Legacy from the Social Capital Debates. Soc. Epistemol. 2009, 23, 125–144. [Google Scholar] [CrossRef]
- Pope, H.C.; Miller, M.C.; Wolfer, T.A.; Mann, J.R.; McKeown, R.E. Psychometric Analysis of a Scale to Assess Norms of Reciprocity of Social Support in Community-Based and Congregation-Based Groups. SAGE Open 2013, 3, 1–12. [Google Scholar] [CrossRef]
- Stevens, N.L.; van Tilburg, T.G. Cohort Differences in Having and Retaining Friends in Personal Networks in Later Life. J. Soc. Pers. Relat. 2011, 28, 24–43. [Google Scholar] [CrossRef]
- Neves, B.B.; Franz, R.L.; Munteanu, C.; Baecker, R. Adoption and Feasibility of a Communication App to Enhance Social Connectedness amongst Frail Institutionalized Oldest Old: An Embedded Case Study. Inf. Commun. Soc. 2018, 21, 1681–1699. [Google Scholar] [CrossRef]
- Fokkema, T.; Knipscheer, K. Escape Loneliness by Going Digital: A Quantitative and Qualitative Evaluation of a Dutch Experiment in Using ECT to Overcome Loneliness among Older Adults. Aging Ment. Health 2007, 11, 496–504. [Google Scholar] [CrossRef]
- Mellor, D.; Firth, L.; Moore, K. Can the Internet Improve the Well-Being of the Elderly? Ageing Int. 2008, 32, 25–42. [Google Scholar] [CrossRef]
- Shapira, N.; Barak, A.; Gal, I. Promoting Older Adults’ Well-Being through Internet Training and Use. Aging Ment. Health 2007, 11, 477–484. [Google Scholar] [CrossRef]
- Perissinotto, C.M.; Stijacic Cenzer, I.; Covinsky, K.E. Loneliness in Older Persons. Arch. Intern. Med. 2012, 172. [Google Scholar] [CrossRef]
- Nicolaisen, M.; Thorsen, K. Who Are Lonely? Loneliness in Different Age Groups (18–81 Years Old), Using Two Measures of Loneliness. Int. J. Aging Hum. Dev. 2014, 78, 229–257. [Google Scholar] [CrossRef]


{kind=link}
| Item on YSQ-SF | Acknowledgment of Schema (Day 1) | Positively Framed Message Delivered on mLINCC (Voice Note and Text) (Day 2) |
|---|---|---|
| I am quite suspicious of other people’s motives | It is understandable that you may feel suspicious of other people and worry that they may hurt you, take advantage of you, or have ulterior motives, especially if these types of experiences have happened in the past. | Counter message; Not all people have negative intentions. There are genuine and trustworthy people in the world. Unfortunately, negative expectations can act as a barrier to your being able to reach out to others. You can change this. Try to evaluate the accuracy of your beliefs. Look back on your life and identify someone who really cared about you. Think about what made this person different. |
| It is only a matter of time before someone betrays me | ||
| I feel that people will take advantage of me | ||
| I feel that I cannot let my guard down in the presence of other people, or else they will intentionally hurt me | ||
| I am usually on the lookout for other people’s ulterior or hidden motives |
| Measure | Description |
|---|---|
| Usage | Frequency of mobile phone use to contact family or friends (less than monthly, monthly, weekly, or daily). Predominant function used on mobile phone. |
| Social Cognition | Disconnection and Rejection domain and related schemas of the YSQ-SF (Abandonment, Defectiveness, Emotional Deprivation, Mistrust and Social Isolation) [43]. Using a 6-point Likert scale rating the most accurate description over the past year from “Completely untrue of me” (1) to “Describes me perfectly” (6) [43,44,45]. YSQ-SF has established reliability and validity in Eastern (Cronbach α 0.72 –0.90) and Western settings (Cronbach α 0.81–0.94) [44] and with the elderly [45]. |
| Loneliness | The DJGLS is a 6-item scale (0–6) with two sub-scales of emotional (0–3) and social loneliness (0–3) [40]. A score of six represents extreme loneliness and three of extreme emotional or social loneliness, measured on its sub-scales [40]. It is recommended for use in the elderly [46], reliable and well validated [40]. |
| Mental well-being | The WHO-5 is a 5-item scale using a 6-point Likert rating and is a first screener for depression (raw score <13) [41,47]. The scale items are positive statements based on mood, vitality and general interest over a two-week period [41]. |
| Variable of Interest | Total Participants (n = 32) | IG n = 15 (46.88%) | CG n = 17 (53.13%) | Statistic | p-Value |
|---|---|---|---|---|---|
| Age group | X2 = 0.41 | p = 0.522 | |||
| Younger old (60–79) | 27 (84.4%) | 12 (80.0%) | 15 (88.2%) | ||
| Older old (80+) | 5 (15.6%) | 3 (20.0%) | 2 (11.8%) | ||
| Gender | X2 = 0.54 | p = 0.659 | |||
| Males | 6 (18.8%) | 2 (13.3%) | 4 (23.5%) | ||
| Females | 26 (81.3%) | 13 (86.7%) | 13 (76.5%) | ||
| Marital status | X2 = 1.31 | p = 0.726 | |||
| Never married | 7 (21.9%) | 3 (20.0%) | 4 (23.5%) | ||
| Married | 5 (15.6%) | 3 (20.0%) | 2 (11.8%) | ||
| Separated/divorced | 9 (28.1%) | 3 (20.0%) | 6 (35.3%) | ||
| Widowed | 11 (34.4%) | 6 (40.0%) | 5 (29.4%) | ||
| Highest Education | X2 = 1.00 | p = 0.755 | |||
| Pre-primary and lower | 18 (56.3%) | 8 (53.3%) | 10 (58.8%) | ||
| 2° and 3° education | 14 (43.8%) | 7 (46.7%) | 7 (41.2%) | ||
| Time living in res | X2 = 0.21 | p = 0.647 | |||
| 1–18 months | 12 (37.5%) | 5 (33.3%) | 7 (41.2%) | ||
| ≥19 months | 20 (62.5%) | 10 (66.7%) | 10 (58.8%) | ||
| Children | X2 = 0.03 | p = 0.589 | |||
| No children | 9 (28.1%) | 4 (26.7%) | 5 (29.4%) | ||
| Yes children | 23 (71.9%) | 11 (73.3%) | 12 (70.6%) | ||
| Grandchildren | X2 = 0.74 | p = 0.388 | |||
| No grandchildren | 11 (34.4%) | 4 (26.7%) | 7 (41.2%) | ||
| Yes grandchildren | 21 (65.6%) | 11 (73.3%) | 10 (58.8%) |
| Variable of Interest | Total Participants (n = 32) | IG n = 15 (46.88%) | CG n = 17 (53.13%) | Statistic | p-Value |
|---|---|---|---|---|---|
| Usage mobile phone | |||||
| Mobile function used most | X2 = 2.89 | p = 0.409 | |||
| Calls (n = 31) | 26 (83.87%) | 13 (92.86%) | 13 (76.5%) | ||
| Frequency network contact | X2 = 1.41 | p = 0.703 | |||
| with mobile phone | |||||
| Weekly (n = 31) | 17 (54.84%) | 7 (50.0%) | 10 (58.8%) | ||
| Cognition (YSQ-SF domain Disconnection and Rejection) | |||||
| Total YSQ-SF/150, α 0.75 | 78.38 ± 25.06 | 83.53 ± 19.30 | 73.82 ± 29.05 | U = 0.46 | p = 0.478 |
| Emotional dep./30, α 0.80 | 16.91 ± 6.16 | 18.93 ± 5.65 | 15.12 ± 6.18 | U = −1.52 | p = 0.128 |
| Social Isolation/30, α 0.78 | 16.72 ± 5.99 | 17.87 ± 5.68 | 15.71 ± 6.23 | U = −0.57 | p = 0.570 |
| Abandonment/30, α 0.81 | 15.28 ± 7.28 | 16.80 ± 5.98 | 13.94 ± 8.21 | U = −1.03 | p = 0.305 |
| Defectiveness/30, α 0.80 | 14.78 ± 5.66 | 14.80 ± 5.19 | 14.76 ± 6.21 | U = −0.11 | p = 0.910 |
| Mistrust/25, α 0.78 | 14.69 ± 5.50 | 15.13 ± 5.28 | 14.29 ± 5.82 | U = −0.30 | p = 0.762 |
| Loneliness (DJGLS) | |||||
| Loneliness total/6, α 0.61 | 3.56 ± 1.24 | 3.53 ± 1.30 | 3.59 ± 1.23 | U = −0.35 | p = 0.727 |
| Emotional loneliness/3, α 0.65 | 1.63 ± 0.83 | 1.73 ± 0.80 | 1.53 ± 0.87 | U = 0.48 | p = 0.477 |
| Social loneliness/3, α 0.55 | 1.94 ± 0.72 | 1.80 ± 0.68 | 2.06 ± 0.75 | U = −1.01 | p = 0.314 |
| Mental well-being (WHO-5) | |||||
| WHO-5/25, α 0.81 | 16.22 ± 5.32 | 15.07 ± 6.87 | 17.24 ± 3.35 | U = −1.01 | p = 0.314 |
| Scale Item | m, sd (T0) | m, sd (T1) | m, sd (T2) | p-Value (T0–T2) (F) | p-Value T0–T1 (W) | p-Value T1–T2 (W) | p-Value T0–T2 (W) | |
|---|---|---|---|---|---|---|---|---|
| IG (T0 n = 15, T1 and 2, n = 13) | Social Cognition (YSQ-SF) | |||||||
| Total YSQ-SF/150 | 83.53 ± 19.30 | 53.85 ± 25.30 | 52.62 ± 15.99 | 0.008 * | 0.019 * | 0.969 | 0.003 * | |
| Emotional Dep./30 | 18.93 ± 5.65 | 12.31 ± 8.29 | 10.23 ± 2.46 | 0.003 * | 0.014 * | 0.582 | 0.003 * | |
| Social Isolation/30 | 17.87 ± 5.68 | 10.38 ± 4.33 | 10.23 ± 3.59 | <0.001 * | 0.002 * | 0.755 | 0.002 * | |
| Abandonment/30 | 16.80 ± 5.98 | 10.23 ± 5.72 | 10.69 ± 5.17 | 0.193 | 0.037 * | 0.655 | 0.041 * | |
| Mistrust/30 | 15.13 ± 5.28 | 12.92 ± 6.65 | 12.08 ± 3.93 | 0.787 | 0.576 | 0.688 | 0.263 | |
| Defectiveness/30 | 14.80 ± 5.19 | 8.00 ± 4.08 | 9.38 ± 3.36 | 0.009 * | 0.007 * | 0.089 | 0.025 * | |
| Loneliness (DJGLS) | ||||||||
| Total loneliness/6 | 3.53 ± 1.30 | 2.31 ± 1.49 | 1.38 ± 1.33 | 0.001 * | 0.031 * | 0.028 * | 0.003 * | |
| Social loneliness/3 | 1.80 ± 0.68 | 1.69 ± 0.75 | 1.08 ± 0.86 | 0.086 | 0.655 | 0.054 | 0.058 | |
| Emotional loneliness/3 | 1.73 ± 0.80 | 0.62 ± 0.96 | 0.31 ± 0.63 | <0.001 * | 0.023 * | 0.157 | 0.003 * | |
| Mental well-being (WHO-5) | ||||||||
| WHO-5/25 | 15.07 ± 6.87 | 17.15 ± 6.31 | 16.54 ± 4.54 | 0.341 | 0.161 | 0.504 | 0.643 | |
| CG (T0 –T2 n = 17) | Social Cognition (YSQ-SF) | |||||||
| Total YSQ-SF/150 | 73.82 ± 29.05 | 70.59 ± 22.15 | 78.00 ± 14.77 | 0.275 | 0.642 | 0.170 | 0.413 | |
| Emotional Dep./30 | 15.12 ± 6.18 | 14.00 ± 5.40 | 16.06 ± 4.18 | 0.476 | 0.534 | 0.195 | 0.704 | |
| Abandonment/30 | 13.94 ± 8.21 | 13.82 ± 5.58 | 14.41 ± 5.08 | 0.570 | 0.887 | 0.670 | 0.932 | |
| Social Isolation/30 | 15.71 ± 6.23 | 14.41 ± 5.01 | 16.47 ± 3.69 | 0.279 | 0.377 | 0.129 | 0.660 | |
| Mistrust/30 | 14.29 ± 5.82 | 15.94 ± 5.32 | 17.65 ± 4.86 | 0.566 | 0.225 | 0.147 | 0.117 | |
| Defectiveness/30 | 14.76 ± 6.21 | 12.41 ± 5.43 | 13.41 ± 5.35 | 0.729 | 0.116 | 0.529 | 0.378 | |
| Loneliness (DJGLS) | ||||||||
| Total loneliness/6 | 3.59 ± 1.23 | 2.47 ± 2.10 | 4.00 ± 1.32 | 0.064 | 0.086 | 0.011 * | 0.282 | |
| Social loneliness/3 | 2.06 ± 0.75 | 1.47 ± 1.18 | 1.88 ± 0.57 | 0.414 | 0.080 | 0.176 | 0.386 | |
| Emotional loneliness/3 | 1.53 ± 0.87 | 1.00 ± 1.12 | 2.12 ± 0.70 | 0.002 * | 0.075 | 0.003 * | 0.704 | |
| Mental well-being (WHO-5) | ||||||||
| WHO-5/25 | 17.24 ± 3.35 | 16.76 ± 4.70 | 16.47 ± 4.00 | 0.591 | 0.584 | 0.699 | 0.413 | |
| T0–T1 | T1–T2 | T0–T2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Scale Item | IG (n = 13) (M, Sd of Differences) | CG (n = 17) (M, Sd of Differences) | p-Value | IG (n = 13) (M, Sd of Differences) | CG (n = 17) (M, Sd of Differences) | p-Value | IG (n = 13) (M, Sd of Differences) | CG (n = 17) (M, Sd of Differences) | p-Value | Effect Size (Hedge’s g) |
| Social Cognition (YSQ-SF) | ||||||||||
| Total YSQ-SF | 28.31 ± 34.13 | 3.24 ± 25.94 | 0.065 | 1.23 ± 15.79 | −7.41 ± 21.56 | 0.133 | −29.54 ± 25.18 | 4.18 ± 29.13 | 0.006 * | 1.23 *** |
| Emotional Dep. | 6.69 ± 7.58 | 1.12 ± 7.7,5 | 0.025 * | 2.08 ± 8.10 | −2.06 ± 6.80 | 0.229 | −8.77 ± 6.58 | 0.94 ± 8.64 | 0.002 * | 1.24 *** |
| Abandonment | 6.69 ± 7.58 | 1.12 ± 7.75 | 0.025 * | −0.46 ± 4.60 | −0.59 ± 7.29 | 0.805 | −5.77 ± 7.54 | 0.47 ± 8.78 | 0.053 | 0.75 ** |
| Social Isolation | 7.08 ± 5.62 | 1.29 ± 6.08 | 0.015 * | 0.15 ± 3.18 | −2.06 ± 5.86 | 0.183 | −7.23 ± 5.73 | 0.76 ± 6.58 | 0.002 * | 1.28 *** |
| Mistrust | 1.92 ± 10.16 | −1.65 ± 6.73 | 0.300 | 0.85 ± 4.78 | −1.71 ± 4.95 | 0.245 | −2.77 ± 7.93 | 3.35 ± 7.75 | 0.048 * | 0.78 ** |
| Defectiveness | 6.38 ± 5.85 | 2.35 ± 5.93 | 0.059 | −1.38 ± 2.63 | −1.00 ± 6.02 | 0.680 | −5.00 ± 6.58 | −1.35 ± 6.22 | 0.123 | 0.57 ** |
| Loneliness (DJGLS) | ||||||||||
| Total loneliness | 1.15 ± 1.57 | 1.12 ± 2.34 | 0.902 | 0.92 ± 1.26 | −1.53 ± 2.00 | 0.001 * | −2.08 ± 1.75 | 0.41 ± 1.58 | <0.001 * | 1.50 *** |
| Social loneliness | 0.08 ± 0.64 | 0.59 ± 1.50 | 0.408 | 0.62 ± 1.04 | −0.41 ± 1.18 | 0.028 * | −0.69 ± 1.18 | −0.18 ± 1.01 | 0.229 | 0.47 * |
| Emotional loneliness | 1.08 ± 1.26 | 0.53 ± 1.18 | 0.157 | 0.31 ± 0.75 | −1.12 ± 1.11 | 0.001 * | −1.38 ± 0.87 | 0.59 ± 0.87 | <0.001 * | 2.26 *** |
| Mental well-being (WHO-5) | ||||||||||
| WHO-5 | −1.92 ± 4.21 | 0.47 ± 4.26 | 0.113 | 0.62 ± 4.94 | 0.29 ± 4.43 | 0.621 | 1.31 ± 5.91 | −0.76 ± 4.40 | 0.363 | 0.41 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarvis, M.A.; Padmanabhanunni, A.; Chipps, J. An Evaluation of a Low-Intensity Cognitive Behavioral Therapy mHealth-Supported Intervention to Reduce Loneliness in Older People. Int. J. Environ. Res. Public Health 2019, 16, 1305. https://doi.org/10.3390/ijerph16071305
Jarvis MA, Padmanabhanunni A, Chipps J. An Evaluation of a Low-Intensity Cognitive Behavioral Therapy mHealth-Supported Intervention to Reduce Loneliness in Older People. International Journal of Environmental Research and Public Health. 2019; 16(7):1305. https://doi.org/10.3390/ijerph16071305
Chicago/Turabian StyleJarvis, Mary Ann, Anita Padmanabhanunni, and Jennifer Chipps. 2019. "An Evaluation of a Low-Intensity Cognitive Behavioral Therapy mHealth-Supported Intervention to Reduce Loneliness in Older People" International Journal of Environmental Research and Public Health 16, no. 7: 1305. https://doi.org/10.3390/ijerph16071305
APA StyleJarvis, M. A., Padmanabhanunni, A., & Chipps, J. (2019). An Evaluation of a Low-Intensity Cognitive Behavioral Therapy mHealth-Supported Intervention to Reduce Loneliness in Older People. International Journal of Environmental Research and Public Health, 16(7), 1305. https://doi.org/10.3390/ijerph16071305