Prevalence of Noise-Induced Hearing Loss Among Tanzanian Iron and Steel Workers: A Cross-Sectional Study


Abstract
:
1. Introduction
2. Materials and Methods
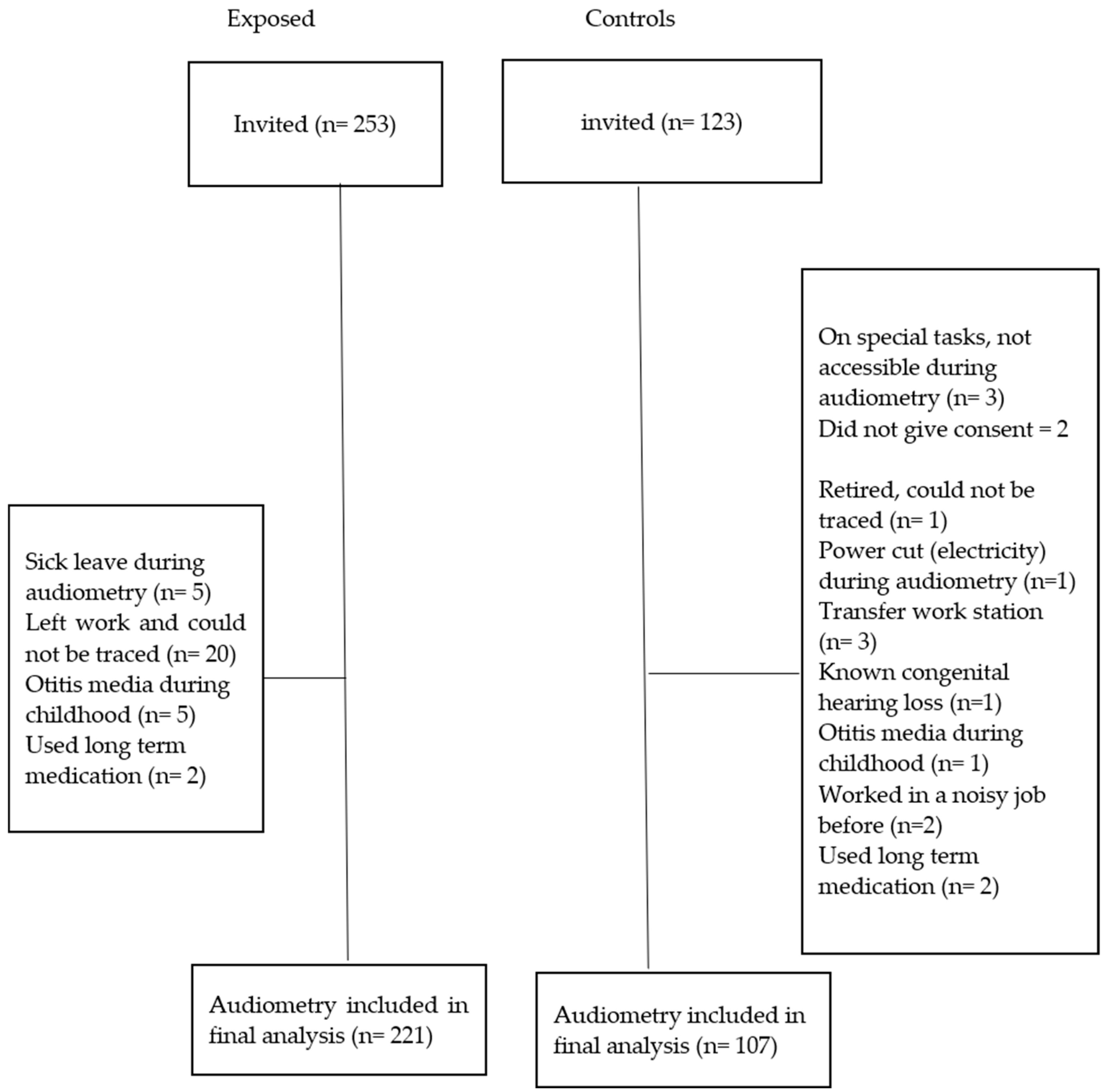
2.1. Study Population
2.2. Study Participants
2.3. Interview Questionnaire and Checklist
2.4. Pure Tone Audiometry
2.5. Data Analysis
2.6. Ethical Clearance
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rabinowitz, P.M. The Public Health Significance of Noise-Induced Hearing Loss. In Noise-Induced Hearing Loss: Scientific Advances; Springer Handbook of Auditory Research 40; le Prell, C.G., Henderson, D., Fay, R.R., Popper, A.N., Eds.; Springer Science + Business Media, LLC: New York, NY, USA, 2012; pp. 13–25. ISBN 978-1-4419-9523-0. [Google Scholar]
- Daniell, W.E.; Swan, S.S.; McDaniel, M.M.; Camp, J.E.; Cohen, M.A.; Stebbins, J.G. Noise exposure and hearing loss prevention programmes after 20 years of regulations in the United States. Occup. Environ. Med. 2006, 63, 343–351. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Prevention of Blindness and Deafness: Global Estimates on Prevalence of Hearing Loss, Estimates 2018. Available online: http://www.who.int/pbd/deafness/estimates/en/ (accessed on 14 August 2018).
- Nelson, D.I.; Nelson, R.Y.; Concha-Barrientos, M.; Fingerhut, M. The global burden of occupational noise-induced hearing loss. Am. J. Ind. Med. 2005, 48, 446–458. [Google Scholar] [CrossRef] [Green Version]
- Lie, A.; Skogstad, M.; Johannessen, H.A.; Tynes, T.; Mehlum, I.S.; Nordby, K.C.; Engdahl, B.; Tambs, K. Occupational noise exposure and hearing: A systematic review. Int. Arch. Occup. Environ. Health 2015, 89, 351–372. [Google Scholar] [CrossRef]
- Macca, I.; Scapellato, M.L.; Carrieri, M.; Maso, S.; Trevisan, A.; Bartolucci, G.B. High-frequency hearing thresholds: Effects of age, occupational ultrasound and noise exposure. Int. Arch. Occup. Environ. Health 2015, 88, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Strauss, S.; Swanepoel, D.W.; Becker, P.; Eloff, Z.; Hall, J.W., III. Noise and age-related hearing loss: A study of 40 123 gold miners in South Africa. Int. J. Audiol. 2014, 53, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Strauss, S.; Swanepoel, D.W.; Becker, P.; Eloff, Z.; Hall, J.W., III. Prevalence and degree of noise-induced hearing loss in South African gold miners: Original research. Occup. Health South. Afr. 2012, 18, 20–25. [Google Scholar]
- Campo, P.; Morata, T.C.; Hong, O. Chemical exposure and hearing loss. Dis. Mon. 2013, 59, 119–138. [Google Scholar] [CrossRef] [Green Version]
- Westerberg, B.D.; Lee, P.K.; Lukwago, L.; Zaramba, S.; Bubikere, S.; Stewart, I. Cross-sectional survey of hearing impairment and ear disease in Uganda. J. Otolaryngol. Head Neck Surg. 2008, 37, 753–758. [Google Scholar]
- Chang, T.Y.; Liu, C.S.; Young, L.H.; Wang, V.S.; Jian, S.E.; Bao, B.Y. Noise frequency components and the prevalence of hypertension in workers. Sci. Total Environ. 2012, 416, 89–96. [Google Scholar] [CrossRef]
- Fischer, M.E.; Schubert, C.R.; Nondahl, D.M.; Dalton, D.S.; Huang, G.H.; Keating, B.J.; Klein, B.E.K.; Klein, R.; Tweed, T.S.; Cruickshanks, K.J. Subclinical atherosclerosis and increased risk of hearing impairment. Atherosclerosis 2015, 238, 344–349. [Google Scholar] [CrossRef]
- Ismaila, S.O.; Odusote, A. Noise exposure as a factor in the increase of blood pressure of workers in a sack manufacturing industry. Beni-Suef Univ. J. Basic Appl. Sci. 2014, 3, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Kang, W.; Yaang, S.R.; Choy, N.; Lee, C.R. Cohort study for the effect of chronic noise exposure on blood pressure among male workers in Busan, Korea. Am. J. Ind. Med. 2009, 52, 509–517. [Google Scholar] [CrossRef]
- Musiba, Z. The prevalence of noise-induced hearing loss among Tanzanian miners. Occup. Med. 2015, 65, 386–390. [Google Scholar] [CrossRef] [Green Version]
- Chadambuka, A.; Mususa, F.; Muteti, S. Prevalence of noise induced hearing loss among employees at a mining industry in Zimbabwe. Afr. Health Sci. 2013, 13, 899–906. [Google Scholar] [CrossRef]
- Kitcher, E.D.; Ocansey, G.; Tumpi, D.A. Early occupational hearing loss of workers in a stone crushing industry: Our experience in a developing country. Noise health 2012, 14, 68–71. [Google Scholar] [CrossRef]
- Ologe, F.E.; Akande, T.M.; Olajide, T.G. Occupational noise exposure and sensorineural hearing loss among workers of a steel rolling mill. Eur. Arch. Otorhinolaryngol. 2006, 263, 618–621. [Google Scholar] [CrossRef]
- World Steel Association. Worlds Steel in Figures 2015. Available online: https://www.worldsteel.org/media-centre/press-releases/2015/world-Steel-in-figures-2015-is-available-online.html (accessed on 22 April 2018).
- Nyarubeli, I.P.; Tungu, A.M.; Bråtveit, M.; Sunde, E.; Kayumba, A.V.; Moen, B.E. Variability and determinants of occupational noise exposure among iron and steel factory workers in Tanzania. Ann. Work Expo. Health 2018, 62, 1109–1122. [Google Scholar] [CrossRef]
- Shield, B.; Dockrell, J.E. External and internal noise surveys of London primary schools. J. Acoust. Soc. Am. 2004, 115, 730–738. [Google Scholar] [CrossRef]
- Sarantopoulos, G.; Lykoudis, S.; Kassomenos, P. Noise levels in primary schools of medium sized city in Greece. Sci. Total Environ. 2014, 482–483, 493–500. [Google Scholar] [CrossRef]
- Silva, L.T.; Oliveira, I.S.; Silva, J.F. The impact of urban noise on primary schools. Perceptive evaluation and objective assessment. Appl. Acoust. 2016, 106, 2–9. [Google Scholar] [CrossRef]
- Dean, A.G.; Soe, M.M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version 3.03a. Available online: http://www.openepi.com/ (accessed on 7 March 2019).
- National Institute for Occupational Safety and Health (NIOSH). Criteria for A Recommended Standard: Occupational Noise Exposure Revised Criteria 1998. NIOSH, Ed.; Cincinnati, Ohio. Available online: https://www.cdc.gov/niosh/docs/98-126/pdfs/98-126.pdf (accessed on 1 August 2018).
- Franks, J.R. Hearing measurement. In Occupational Exposure to Noise: Evaluation, Prevention and Control; World Health Organization, Ed.; WHO Electronic Book; WHO: Dortmund, The Netherlands, 2001; Chapter 8; pp. 183–232. [Google Scholar]
- International Organization for Standardization (ISO). Acoustics-Audiometric Test Methods—Part1: Pure Tone Air and Borne Conduction Audiometry; ISO standard 8253-1:2010; ISO: Geneva, Switzerland, 2010. [Google Scholar]
- British Society of Audiology (BSA). Recommended Procedure: Pure Tone Air Conduction and Borne Conduction Threshold Audiometry with or without Masking. 80 Brighton Road, Reading Berkshire, RG6 1PS, UK: British Society of Audiology; 2011. Available online: http://www.thebsa.org.uk/wp- content/uploads/2014/04/BSA_RP_PTA_FINAL_24Sept11_MinorAmend06Feb12.pdf (accessed on 9 November 2017).
- The Norwegian Labour Inspection Authority. Audiometric Testing in Noise Exposed Workers; The Norwegian Labour Inspection Authority: Trondheim, Norway, 2013. (In Nowegian) [Google Scholar]
- International Organization for Standardization (ISO). Acoustics-Estimation of Noise-Induced Hearing Loss; ISO standard 1999:2013; ISO: Geneva, Switzerland, 2013. [Google Scholar]
- Rabinowitz, P.M.; Galusha, D.; McTague, M.F.; Slade, M.D.; Wesdock, J.C.; Dixon-Ernst, C. Tracking occupational hearing loss across global industries: A comparative analysis of metrics. Noise Health 2012, 14, 21–27. [Google Scholar] [CrossRef]
- Lutman, M.E. What is the risk of noise-induced hearing loss at 80, 85, 90 dB(A) and above? Occup. Med. 2000, 50, 274–275. [Google Scholar] [CrossRef]
- Singh, L.P.; Bhardwaj, A.; Kumar, D.K. Prevalence of permanent hearing threshold shift among workers of Indian iron and steel small and medium enterprises: A study. Noise health 2012, 14, 119–128. [Google Scholar]
- Mantysalo, S.; Vuori, J. Effects of impulse noise and continuous steady state noise on hearing. Br. J. Ind. Med. 1984, 4, 122–132. [Google Scholar] [CrossRef]
- Agarwal, G.; Nagpure, P.S.; Gadge, S.V. Noise Induced Hearing Loss in Steel Factory workers. Int. J. Occup. Saf. Health 2015, 4, 34–43. [Google Scholar] [CrossRef]
- Whittaker, J.D.; Robinson, T.; Acharya, A.; Singh, D.; Smith, M. Noise-induced hearing loss in small-scale metal industry in Nepal. J. Laryngol. Otol. 2014, 128, 871–880. [Google Scholar] [CrossRef]
- Dobie, R.A. The burdens of age-related and occupational noise-induced hearing loss in the United States. Ear Hear. 2008, 29, 565–577. [Google Scholar] [CrossRef]
- Sulkowski, W.J. Hearing impairment caused by impulse noise: Survey in the drop forging industry. Scand. Audiol. Suppl. 1980, 12, 307–317. [Google Scholar]
- Kamal, A.A.; Mikael, R.A.; Faris, R. Follow-up of hearing thresholds among forge hammering workers. Am. J. Ind. Med. 1989, 16, 645–658. [Google Scholar] [CrossRef]
- McBride, D.I.; Williams, S. Audiometric notch as a sign of noise induced hearing loss. Occup. Environ. Med. 2001, 58, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Kirchner, D.B.; Evenson, C.E.; Dobie, R.A.; Rabinowitz, P.M.; Crawford, J.; Kopke, R.; Hudson, T.W. Occupational Noise Induced Hearing Loss. ACOEM task force on Occupational Hearing Loss. ACOEM guidance statement. J. Occup. Environ. Med. 2012, 54, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, P.M.; Galusha, D.; Slade, M.D.; Dixon-Ernst, C.; Sircar, K.D.; Dobie, R.A. Audiogram Notches in Noise-Exposed Workers. Ear Hear. 2006, 27, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Dobie, R.A. Noise-induced permanent threshold shifts in occupational noise and hearing survey: An explanation for elevated risk estimates. Ear Hear. 2007, 28, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Mulwafu, W.; Kuper, H.; Ensink, R.J. Prevalence and causes of hearing impairment in Africa. Trop. Med. Int. Health 2016, 21, 158–165. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Descriptive | p-Value | |
|---|---|---|---|
| Exposed (n (%)) | Controls (n (%)) | ||
| Age: Mean (SD) | 32 (8) | 40 (7) | <0.001 a |
| Age group (years) (group mean for Exposed)) | |||
| 18–35 (27) | 149 (67.4) | 36 (33.6) | <0.001 b |
| 36–43 (39) | 58 (26.2) | 37 (34.6) | |
| 44–59 (47) | 14 (6.3) | 34 (31.8) | |
| Total | 221 (100.0) | 107 (100.0) | |
| Duration of work (years) (group mean for Exposed) | |||
| ≤2 (1) | 86 (38.9) | - | <0.001 b |
| 3–10 (5) | 108 (48.9) | 27 (25.2) | |
| 11–37 (17) | 27 (12.2) | 80 (74.8) | |
| Current smoking | |||
| no | 183 (82.8) | 96 (89.7) | |
| yes | 38 (17.2) | 11 (10.3) | 0.07 |
| Previous noisy work | |||
| no | 178 (80.5) | 107 (100.0) | |
| yes | 43 (19.5) | - | <0.001 b |
| Tinnitus | |||
| no | 202 (91.4) | 104 (97.2) | |
| yes | 19 (8.6) | 3 (2.8) | 0.06 |
| Relative with hearing impairment | |||
| no | 199 (90.0) | 96 (89.7) | |
| yes | 22 (10.0) | 11 (10.3) | 0.9 |
| History of ear-related medical condition | |||
| no | 176 (79.6) | 93 (86.9) | |
| yes | 45 (20.4) | 14 (13.1) | 0.01 b |
| Variable | Hearing Loss a (n (%)) | |||
|---|---|---|---|---|
| Exposed | Controls | Chi-Square Test (p-Value) | Prevalence Ratio 95% Confidence Interval) † | |
| Age group (years) | ||||
| 18–35 | 63 (42.3) | 5 (13.9) | 0.002 * | 2.5 (0.93, 6.76) |
| 36–43 | 34 (58.6) | 12 (32.4) | 0.013 * | 1.7 (0.79, 3.47) |
| 44–59 | 10 (71.4) | 16 (47.0) | 0.124 | 1.5 (0.58, 3.70) |
| All | 107 (48.4) | 33 (30.8) | 1.3 (1.10, 1.62) | |
| Workers’ Group | Number of Workers | Mean Hearing Thresholds in Decibel (dB) for Each Frequency | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 250 | 500 | 1000 | 2000 | 3000 | 4000 | 6000 | 8000 | ||
| Exposed | 221 | 17.0 (6.1) | 19.0 (5.2) | 19.4 (6.0) | 19.6 (7.3) | 23.6 (8.9) a | 25.0 (9.7) a | 24.3 (10.6) a | 16.0 (9.7) a |
| Control | 107 | 17.2 (5.5) | 18.0 (5.7) | 19.7 (5.2) | 18.8 (8.1) | 20.8 (8.0) | 21.7 (8.8) | 19.6 (9.2) | 13.6 (9.8) |
| Age Group | Audiometry Frequency (Hz) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 250 | 500 | 1000 | 3000 | 4000 | 6000 | 8000 | ||||||||
| β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI | |
| 18–35 | ||||||||||||||
| 0.16 | −2.31, 2.63 | −1.54 | −3.47, 0.39 | −0.53 | −2.57, 1.52 | −3.05 | −6.19, 0.11 | −4.94 * | −8.57, −1.31 | −5.84 * | −10.16, −1.52 | −4.90 * | −8.66, −1.14 | |
| 36–43 | ||||||||||||||
| −0.14 | −3.06, 2.77 | −1.92 | −4.63, 0.79 | −1.45 | −4.54, 1.64 | −5.70 * | −10.11, −2.27 | −6.37 * | −10.93, −1.81 | −4.32 * | −8.73, 0.09 | −3.36 | −7.51, 0.79 | |
| 44–59 | ||||||||||||||
| −0.72 | −5.51, 4.07 | −2.47 | −6.52, 1.59 | −1.07 | 0.67, −6.20 | −6.85 | −14.66, 0.95 | −4.95 | −13.23, 3.33 | −10.22 * | −18.87, −1.58 | −6.00 | −15.41, 3.41 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nyarubeli, I.P.; Tungu, A.M.; Moen, B.E.; Bråtveit, M. Prevalence of Noise-Induced Hearing Loss Among Tanzanian Iron and Steel Workers: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 1367. https://doi.org/10.3390/ijerph16081367
Nyarubeli IP, Tungu AM, Moen BE, Bråtveit M. Prevalence of Noise-Induced Hearing Loss Among Tanzanian Iron and Steel Workers: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(8):1367. https://doi.org/10.3390/ijerph16081367
Chicago/Turabian StyleNyarubeli, Israel P., Alexander M. Tungu, Bente E. Moen, and Magne Bråtveit. 2019. "Prevalence of Noise-Induced Hearing Loss Among Tanzanian Iron and Steel Workers: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 8: 1367. https://doi.org/10.3390/ijerph16081367
APA StyleNyarubeli, I. P., Tungu, A. M., Moen, B. E., & Bråtveit, M. (2019). Prevalence of Noise-Induced Hearing Loss Among Tanzanian Iron and Steel Workers: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 16(8), 1367. https://doi.org/10.3390/ijerph16081367