Online Resources for People Who Self-Harm and Those Involved in Their Informal and Formal Care: Observational Study with Content Analysis


Abstract
:1. Introduction
2. Materials and Methods
3. Results
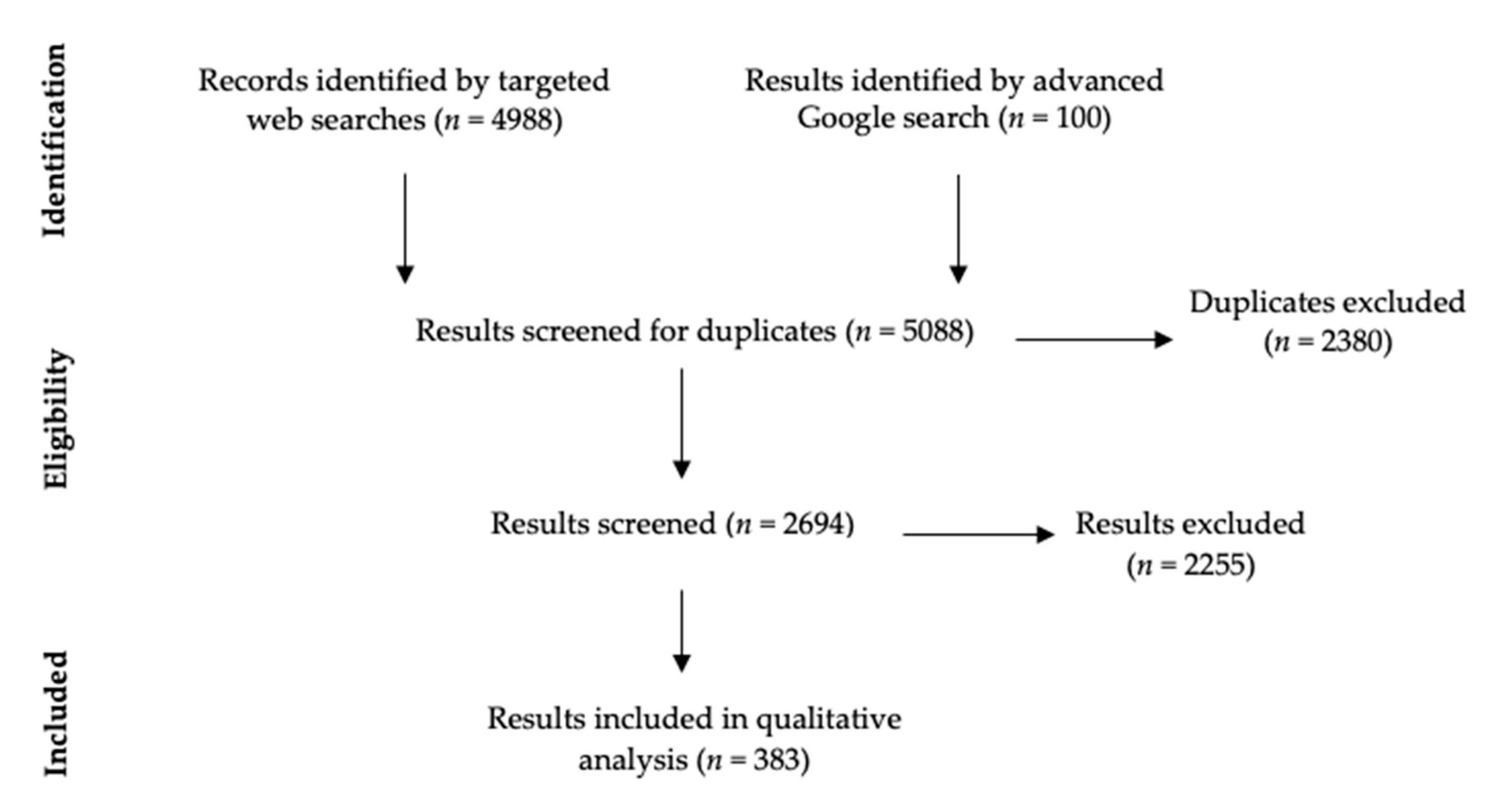
3.1. Searches
3.1.1. Help Offered by Professionals
“There is evidence that some ‘talking therapies’, e.g., problem-solving therapy, psychodynamic therapy and cognitive behavioural therapy (CBT) are useful in helping people who harm themselves.”(Improving the lives of people who self-harm, HSC Public Health Agency)
“My relationships with the psychotherapist and the psychologist were a lifeline, and my psychotherapist certainly kept me alive many times.”(Northern Ireland, United Kingdom: Caitriona Cassidy, World Health Organisation)
“A risk management plan can help people who self-harm reduce their risk of self-harming again. It should be based on a risk assessment and developed with the person who has self-harmed, who should have joint ownership of the plan.”(Self-harm [QS34], NICE)
“Primary care practitioners, in applying the recommend bio-psycho-social approach, should ensure prompt referrals to psychology (IAPT) services.”(Mental health: self-harming in older adults has distinct characteristics, Royal College of General Practitioners)
“Summarise the key areas of needs and risks identified in the assessment and use these to develop a care plan and a risk management plan in conjunction with the person who self-harms and their family, carers or significant others if this is agreed with the person. Provide printed copies for the service user and share them with the GP.”(Self-harm in over 8s: long-term management [CG133], NICE)
3.1.2. Help Offered by Non-Professionals
“Lots of young people have said that telling someone about their self-harm was one of the best ways of coping.”(Self-harm, Childline)
“If you can, try and stay calm and non-judgemental – it will help both you and your friend.”(How to react when your friend says they self-injure, LifeSIGNS)
“[People who self-harm] often report that the sympathy, tolerance and respect of those close to them is integral to getting their self-harm under control.”(Self-harm – what, who, why and how to help, British Psychological Society, identified via Self Injury Support Network)
“A group of people, who all self-harm, meet regularly to give each other emotional support and practical advice. Just sharing your problems in a group can help you to feel less alone - others in the group will almost certainly have had similar experiences.”(Self harm, Royal College of Psychiatrists)
“Sometimes joining a social activity or sports group can be helpful as a distraction. This can also provide a form of social support.”(Coping with self-harm; Royal College of General Practitioners)
“Mummé and her colleagues report that family support was the “predominant interpersonal” factor associated with stopping self-harming, including in studies that involved adults, not just those with teens and children.”(Family support in self-harming, British Psychological Society)
“Seek out online communities of people who are honestly looking to support each other overcome self-harm. Support from others is incredibly powerful and can help you refrain from hurting yourself.”(We Need To Talk About Online Self-Harm Content, The Mix)
“Reboot your social media by following different, positive accounts. By doing this you’ll fill your feed with positive content, coping strategies, images and messages that are going to raise you up rather than beat you down.”(We Need To Talk About Online Self-Harm Content, The Mix)
3.2. Strategies to Help Stop Self-Harming
3.3. Personal Accounts of Recovery
3.3.1. Self-Discovery and Development, whether Alone or through Help from Psychological Therapy
“The start of my healing came via creative writing. I was too ashamed and afraid to talk about what was happening so I put it onto paper instead.”(Terrible times, self-injury and recovery, LifeSIGNS)
“Other important factors that enabled people to stop harming included self-development, sometimes in the form of insight into reasons for harming gained through counselling, other times simply through growing older and benefiting from the increase in confidence, stability, self-knowledge and control over life associated with this.”(Self-harm, SANE)
3.3.2. Contemplation about and Motivation to Stop Self-Harming
“An important step forward is making the decision to learn to live without self-harm, and being prepared to face underlying issues that may have caused the behaviours in the first place.”(Recovering from self-harm, SelfHarmUK)
3.3.3. The Impact of Self-Harm on Others
“My parents found out and made me feel bad about it… I’m glad I don’t do it anymore but only because I don’t want to upset anyone.”(Self-Harm, SANE)
“Interestingly, one study found that [people who used to self-harm] saw their self-harm as a useful coping mechanism, but had been motivated to stop because their loved ones wanted them to stop.”(Family support in self-harming, British Psychological Society)
3.3.4. The Negative Impact of Scars
“Another thing that made me break away from self-harming is the fact that my scars started to make me feel even more insecure than I already was.”(Self-harm is real, SelfHarmUK)
3.4. Specific Demographic Groups
“Complete a behaviour diary, which records what is occurring before, during and after the behaviour. This could help you to understand the purpose of the behaviour. Makes notes on the environment, including who was there, any change in the environment and how you think the person was feeling.”(Self-injurious behaviour, National Autistic Society)
“ACCT is a prisoner-centred, flexible care-planning system which, when used effectively, can reduce risk, primarily of self-harm.”(Mental health of adults in contact with the criminal justice system [NG66], NICE)
“The Listener scheme is a peer supportive service which aims to reduce suicide and self-harm in prisons. Prisoners are trained and supported by the Samaritans to become Listeners. Listeners can provide confidential emotional support to you when you are struggling to cope.”(Prisoners and Self Harm, Rethink Mental Illness)
“RCPsych recommends that children stop using technology at least an hour before going to bed and avoid using technology at mealtimes.”(Psychiatrists should consider impact of social media on all children they assess, Royal College of Psychiatrists)
“Find out who the Designated Safeguarding Lead Person is for the young person’s school and arrange to have a meeting with them so that you can address the situation. They will be able to help you put an action plan in place to keep the young person safe, and will explore ways you can work together to bring an end to the self-harming behaviour.”(Understanding Self-Harm in Young People, Child Protection Company)
3.5. Website Review
4. Discussion
Clinical and Research Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Clements, C.; Turnbull, P.; Hawton, K.; Geulayov, G.; Waters, K.; Ness, J.; Townsend, E.; Khundakar, K.; Kapur, N. Rates of self-harm presenting to general hospitals: A comparison of data from the Multicentre Study of Self-Harm in England and Hospital Episode Statistics. BMJ Open 2016, 6, e009749. [Google Scholar] [CrossRef] [PubMed]
- McManus, S.; Gunnell, D.; Cooper, C.; Bebbington, P.; Howard, L.; Brugha, T. Prevalence of non-suicidal self-harm and service contact in England, 2000–2014: Repeated cross-sectional surveys of the general population. Lancet Psych. 2019, 6, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Carr, M.J.; Ashcroft, D.M.; Kontopantelis, E.; Awenat, Y.; Cooper, J.; Chew-Graham, C.; Kapur, N.; Webb, R. The epidemiology of self-harm in a UK-wide primary care patient cohort, 2001–2013. BMC. Psych. 2016, 16, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mars, B.; Heron, J.; Biddle, L.; Donovan, J.L.; Holley, R.; Piper, M.; Potokar, J.; Wyllie, C.; Gunnell, D. Exposure to, and searching for, information about suicide and self-harm on the Internet: Prevalence and predictors in a population based cohort of young adults. J. Affect. Disord. 2015, 185, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, I.M.; Roberts, L.M.; Van Ballegooijen, W.; Wicks, P. Exploring the Use and Effects of Deliberate Self-Harm Websites: An Internet-Based Study. J. Med. Internet. Res. 2013, 15, e285. [Google Scholar] [CrossRef] [PubMed]
- Daine, K.; Hawton, K.; Singaravelu, V.; Stewart, A.; Simkin, S.; Montgomery, P. The Power of the Web: A Systematic Review of Studies of the Influence of the Internet on Self-Harm and Suicide in Young People. PLoS ONE 2013, 8, e77555. [Google Scholar] [CrossRef] [PubMed]
- Dubicka, B.; Theodosieu, L. Technology Use and the Mental Health of Children and Young People; CR Royal College of Psychiatrists: London, UK, 2020; pp. 1–823. [Google Scholar]
- Department for Digital, Culture, Media & Sport, Home Office. Online Harms White Paper. 2019. Available online: https://www.gov.uk/government/consultations/online-harms-white-paper (accessed on 27 April 2020).
- Messina, E.S.; Iwasaki, Y. Internet Use and Self-Injurious Behaviors among Adolescents and Young Adults: An Interdisciplinary Literature Review and Implications for Health Professionals. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.; Fortune, S. Understanding Self-Harm and Suicide Websites. Crisis 2008, 29, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Stiglic, N.; Viner, R.M. Effects of screentime on the health and well-being of children and adolescents: A systematic review of reviews. BMJ Open 2019, 9, e023191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchant, A.; Hawton, K.; Stewart, A.; Montgomery, P.; Singaravelu, V.; Lloyd, K.; Purdy, N.; Daine, K.; John, A. A systematic review of the relationship between internet use, self-harm and suicidal behaviour in young people: The good, the bad and the unknown. PLoS ONE 2017, 12, e0181722. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, N.; Brennan, C.; House, A. Self-harm and social media: Thematic analysis of images posted on three social media sites. BMJ Open 2018, 9, e027006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, V.; Owens, D. Using the internet as a source of self-help for people who self-harm. Psychiatr. Bull. 2001, 25, 222–225. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 2, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J.C. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Heal. Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tezlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Ryan-Vig, S.; Gavin, J.; Rodham, K. The Presentation of Self-Harm Recovery: A Thematic Analysis of YouTube Videos. Deviant Behav. 2019, 40, 1596–1608. [Google Scholar] [CrossRef]
- Padmanathan, P.; Biddle, L.; Carroll, R.; Derges, J.; Potokar, J.; Gunnell, D. Suicide and self-arm related Internet use. Crisis 2018, 39, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Cooney, G.M.; Morris, J. Time to start taking an internet history? Br. J. Psychiatry 2009, 194, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimond, B. National Institute for Clinical Excellence. Br. J. Midwifery 2004, 12, 84. [Google Scholar] [CrossRef]
- Bailey, D.; Wright, N.; Kemp, L. Self-harm in young people: A challenge for general practice. Br. J. Gen. Pr. 2017, 67, 542–543. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Literature that Provides Information or Advice about what Helps to Stop or Reduce Self-Harming Behaviour Available in English Published by an Organisation within the United Kingdom Literature Related to or Aimed at Individuals with or without Co-Occurring Psychiatric Disorders Literature Across all Motives (Non-Suicidal or Suicidal) and Methods (Poisoning or Self-Injury) of Self-Harm | Empirical studies Online forums Social media Inaccessible to the public (page not available, requires log-in) |
| Strategy | Number of Websites | Examples |
|---|---|---|
| Delaying (The 5 Minute Rule) | 9 | “Some people find that putting off harming themselves can decrease or get rid of the urge.” (Coping with self-harm: a guide for parents and carers, Royal College of Psychiatrists) “If you find distraction doesn’t work, you could also try delaying. This means waiting for five minutes before you self-harm and see if the urge is as strong. Try to build up the amount of time you can put it off.” (Self-harm, Counselling Directory) |
| Distraction | 12 | “Distraction techniques can help you resist the urge to self-harm until the feeling passes” (Self-harm Rape Crisis, identified via Self Injury Support Network) Some guidance grouped distraction methods around different emotions to suggest ways that some techniques, such as writing or running, might be more effective depending on what might be behind an urge to self-harm”. (What to do if you get the urge to self-harm, Patient) Examples of distraction techniques were: Talking to someone you trust Writing letters Cleaning and tidying Exercise Reading a book Listening to music |
| Substitution (Replacement of the Act of SH with Other Acts that Satistfy the Urge) | 11 | “Replacing the cutting or other self -harm with safer activities can be a positive way of coping with the tension.” (Supporting Children and Young People who Self-Harm, Northamptonshire Children and Young People’s Partnership, identified via Self Injury Support Network) “Try to satisfy that urge without hurting yourself. It can be anything from flicking elastic bands against your wrist, rubbing ice cubes on your skin, or dropping hot sauce on your tongue.” (Self harm is an addictive way to cope with mental pain, The Mix) |
| Harm Minimisation | 4 | “If stopping self-harm is unrealistic in the short term, consider strategies aimed at harm reduction.” (Self-harm in over 8s: long-term management [CG133], NICE) |
| Hiding Objects | 4 | “Reducing the accessibility of objects that might be used for self-harm (e.g., pencil sharpeners, knives, medication etc.) may help to delay the impulse to self-harm.” (Coping with self-harm: a guide for parents and carers, Royal College of General Practitioners) |
| Relaxation Techniques | 7 | “Try relaxation and breathing exercises. Sit back comfortably in a chair or lie out on a bed. Relax all muscles in your body, beginning at the feet and working upwards. Concentrate on your breathing: breathe in for 5 s through your nose, hold your breath for 5 s, then breathe out slowly. Repeat this.” (Self-harm, Survivors Manchester, identified via SurvivorsUK) |
| Identifying and Avoiding Immediate Precipitants (E.G. Alcohol, or Looking at Websites that May Cause Distress) | 11 | “Identifying what triggers your self-harming can give you more control. Even if you can’t avoid those triggers altogether, you can develop strategies to deal with your emotions when things start becoming overwhelming.” (How to get control over your self-harm, SelfHarmUK) |
| Acknowledging Choice | 5 | “All behaviours are a choice, and if we stop to take a breath before self-injuring, and recognise that we are responsible for the continuation of our destructive cycles, then we become empowered to break them.” (Choice, LifeSIGNS) |
| Mindfulness | 4 | “Many people find mindfulness techniques very helpful in getting past the urge to self-injure.” (Self-Injury Awareness Day, Mental Health Matters) |
| Go to a Safe Place | 7 | “Most people self-harm when alone so go to a public place, be with a good friend or a safe family member. This may prevent you from harming yourself.” (Self-harm, a self-help guide, Survivors Manchester, identified via SurvivorsUK) |
| Planning Ahead | 10 | “Make a self-soothe box – work with the young person to collect a range of different things they can use to distract or soothe themselves when they feel the urge to self-harm. This might include music, colouring, books, bubbles, photographs or inspirational quotes.” (No Harm Done, Young Minds) “You may also find it helpful to write a list of all the people, organisations and websites that you can go to for help when you are finding things difficult.” (Helping yourself long-term, Mind) |
| Strategy | Number of Websites | Examples |
|---|---|---|
| Understanding Self-harm | 20 | “Perhaps the most important thing is to think about why you’ve started to self-harm in the first place and what purpose it serves for you.” (Steps to self-harm recovery, The Mix) |
| Identifying and Managing Emotions | 19 | “Try to be clear about what you are feeling – is the emotion you are feeling: fear, shame or guilt, anxiety, anger, rage, sadness or depression? Try and observe, label and accept the emotion. Ask yourself why you are feeling it.” (Self-harm, Survivors Manchester, identified via SurvivorsUK) “Many people who self-harm do so repetitively, because although it is destructive it releases the unbearable tension and therefore it seems to ‘work’. Self-harmers need to learn a different means of expressing emotion”. (Self-harm, what, who, why, and how to help, British Psychological Society, identified via Self Injury Support Network) |
| Positive Thinking | 5 | “It may also be helpful to try and encourage the student to think about some positive things about themselves and their life and develop a ‘hope box’ where they can store things that make them feel better, such as photos, memories, nice things people have said etc.” (Young people who self-harm, University of Oxford, identified via Self Injury Support Network) |
| Mindfulness | 4 | “Mindfulness may teach you to be more aware of your thoughts and feelings. Once you are more aware of your thoughts and feelings, you can learn to deal with them better.” (Prisoners and Self Harm, Rethink Mental Illness) |
| Improving General Well Being | 10 | “When we’re taking care of ourselves and are seeking help and support for the issues that are causing us distress, we feel good that we are helping ourselves and are taking steps along a path of recovery” (Choice, LifeSIGNS) |
| Developing New Ways of Coping | 17 | “Moving away from self-injury however requires learning new coping mechanisms that can help you move towards change” (New Year, new you?, LifeSIGNS) |
| Tackling Underlying Issues | 16 | “I think the best way to stop self-harm is to focus on the underlying issues which trigger you to do it. If you work on these issues, then the self-harm will stop naturally”. (Understanding self-harm, Scottish Association for Mental Health) |
| Treating Mental Illness | 8 | “Untreated mental health problems may contribute to an increased risk of continuing self-harm or even suicide”. (Study looks at self-harm in young people, NHS) |
| Faith and Religion | 1 | “It’s hard to explain the awesomeness and the powerfulness of what God did inside me that week. He gently gave me the strength to ask for help, protecting me and showing me how His strength was better than anything I could ever get from self-harming, showing me I was worth a lot more to Him.” (Survivors’ stories, Adullam Ministries) |
| Developing a Creative Outlet | 10 | “Do something creative: make a collage of colours to represent your mood or to remind you of your favourite things.” (The truth about self-harm, Mental Health Foundation) |
| Seek Professional Help | 15 | “Encourage them, if they have not already done so, to seek professional help. Offer to go with them to their GP or a counsellor. If you’re at school, perhaps there is a teacher they trust of the school nurse.”. (How to react when your friend says they self-injure, LifeSIGNS) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeu, D.; Guthrie, E.; Brennan, C.; Farley, K.; House, A. Online Resources for People Who Self-Harm and Those Involved in Their Informal and Formal Care: Observational Study with Content Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3532. https://doi.org/10.3390/ijerph17103532
Romeu D, Guthrie E, Brennan C, Farley K, House A. Online Resources for People Who Self-Harm and Those Involved in Their Informal and Formal Care: Observational Study with Content Analysis. International Journal of Environmental Research and Public Health. 2020; 17(10):3532. https://doi.org/10.3390/ijerph17103532
Chicago/Turabian StyleRomeu, Daniel, Elspeth Guthrie, Cathy Brennan, Kate Farley, and Allan House. 2020. "Online Resources for People Who Self-Harm and Those Involved in Their Informal and Formal Care: Observational Study with Content Analysis" International Journal of Environmental Research and Public Health 17, no. 10: 3532. https://doi.org/10.3390/ijerph17103532
APA StyleRomeu, D., Guthrie, E., Brennan, C., Farley, K., & House, A. (2020). Online Resources for People Who Self-Harm and Those Involved in Their Informal and Formal Care: Observational Study with Content Analysis. International Journal of Environmental Research and Public Health, 17(10), 3532. https://doi.org/10.3390/ijerph17103532