Physical and Psychological Factors Associated with Poor Self-Reported Health Status in Older Adults with Falls


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
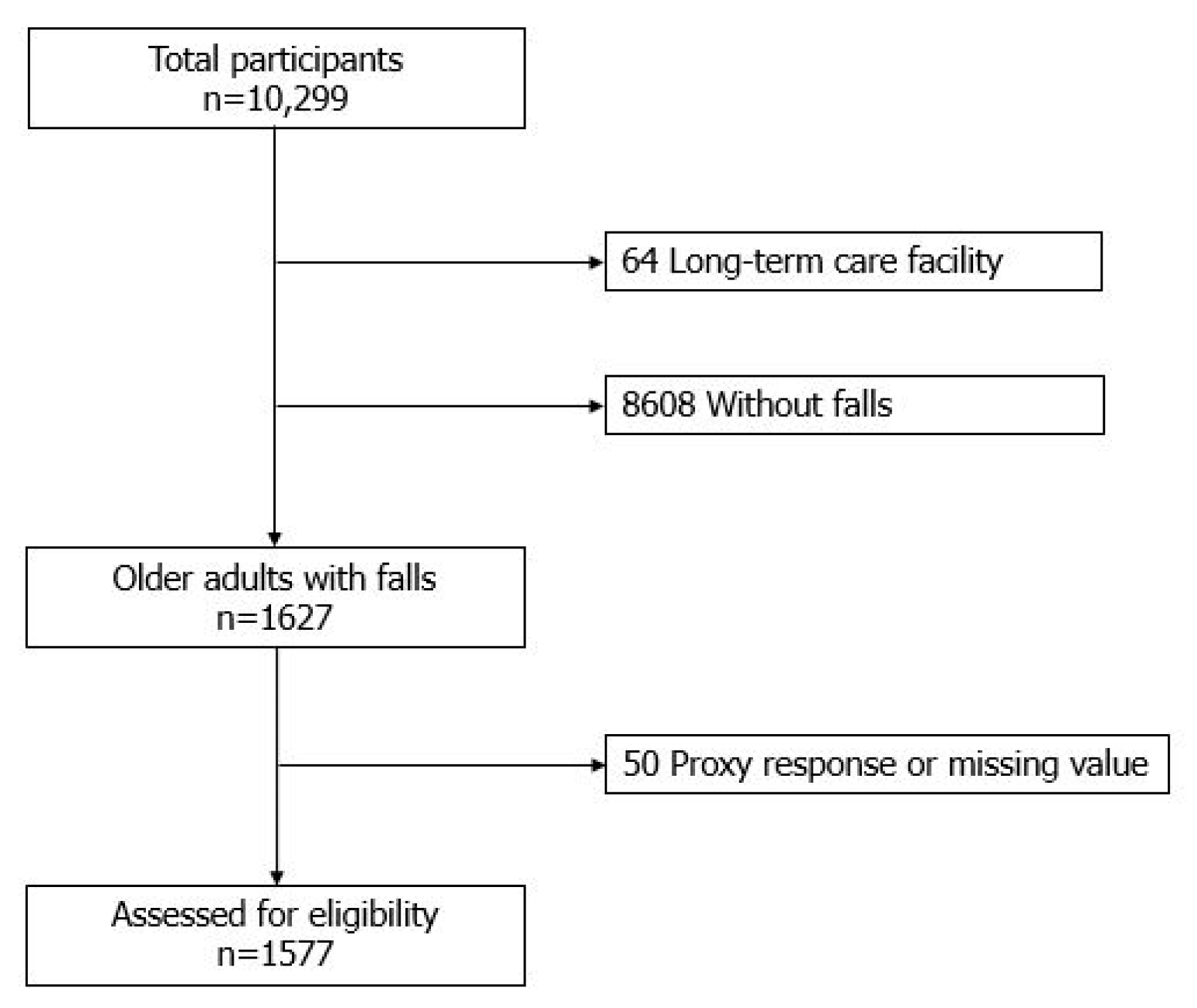
2.2. Patient Selection and Study Design
2.3. Ethical Considerations
2.4. Measurements
2.4.1. Subjective Assessments of Health
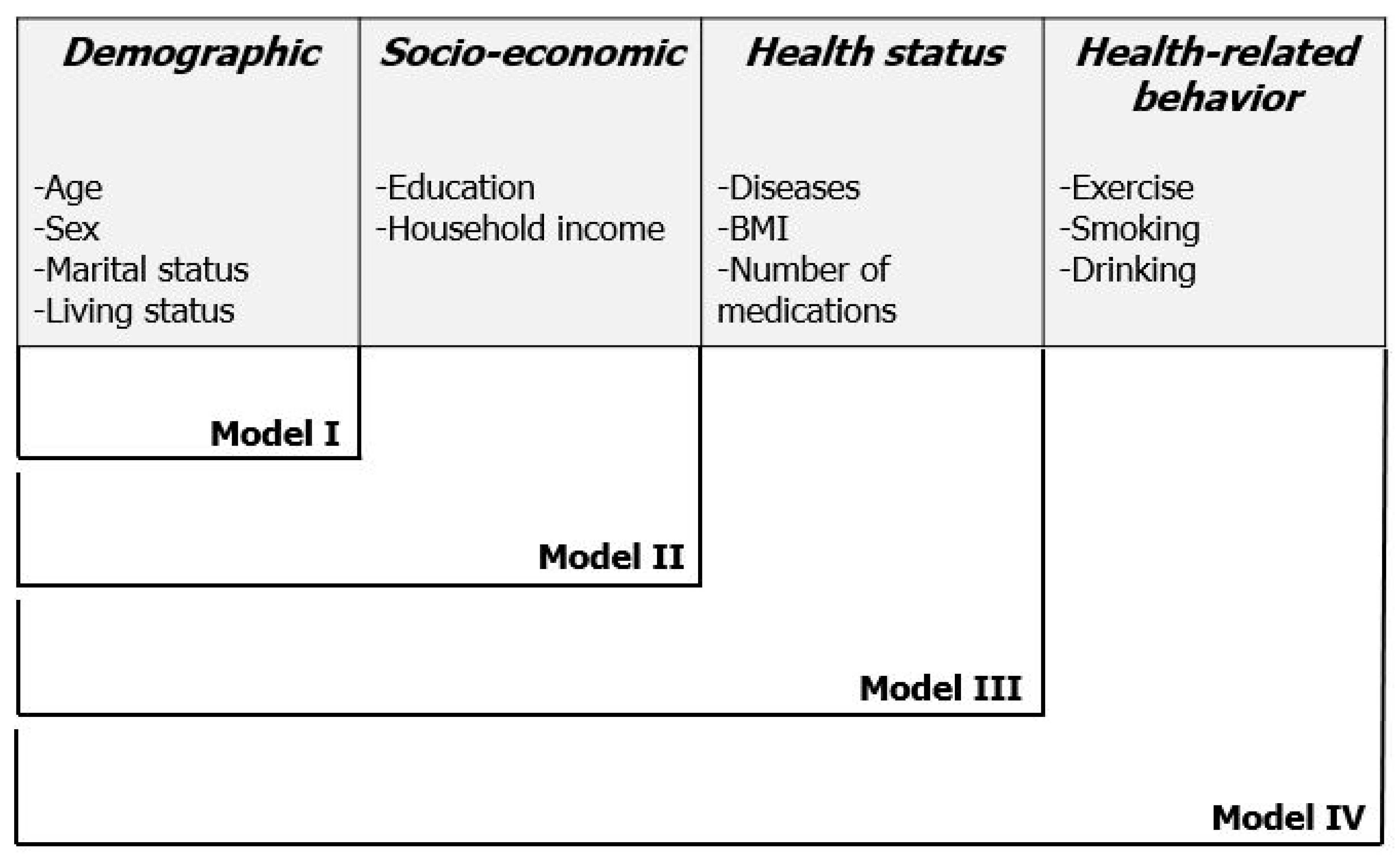
2.4.2. Individual Variables
2.4.3. Physical Variables
2.4.4. Psychological Variables
2.5. Data Analysis
3. Results
3.1. Incidence and Average Number of Falls
3.2. Subjective Assessments of Health
3.3. Differences in Individual Characteristics between Those with Good and Those with Poor Self-Reported Health Status
3.4. Differences in Physical and Psychological Characteristics between Those with Good and Poor Self-Reported Health Statuses
3.5. Multivariable Logistic Regression Analysis of Factors Associated with Poor Self-Reported Health Status Using Individual Variable-Adjusted Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Verma, S.K.; Willetts, J.L.; Corns, H.L.; Marucci-Wellman, H.R.; Lombardi, D.A.; Courtney, T.K. Falls and Fall-Related Injuries among Community-Dwelling Adults in the United States. PLoS ONE 2016, 11, e0150939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, E.R.; Stevens, J.A.; Lee, R. The direct costs of fatal and non-fatal falls among older adults—United States. J. Saf. Res. 2016, 58, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.G.; Kim, S.C.; Chang, M.; Nam, E.; Kim, S.G.; Cho, S.I.; Ryu, D.H.; Kam, S.; Choi, B.Y.; Park, S.B.; et al. Complications and Socioeconomic Costs Associated with Falls in the Elderly Population. Ann. Rehabil. Med. 2018, 42, 120–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiedemann, A.; Shimada, H.; Sherrington, C.; Murray, S.; Lord, S. The comparative ability of eight functional mobility tests for predicting falls in community-dwelling older people. Age Ageing 2008, 37, 430–435. [Google Scholar] [CrossRef] [Green Version]
- Shimada, H.; Suzukawa, M.; Tiedemann, A.; Kobayashi, K.; Yoshida, H.; Suzuki, T. Which neuromuscular or cognitive test is the optimal screening tool to predict falls in frail community-dwelling older people? Gerontology 2009, 55, 532–538. [Google Scholar] [CrossRef]
- Park, S.H. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Shimada, H.; Suzukawa, M.; Ishizaki, T.; Kobayashi, K.; Kim, H.; Suzuki, T. Relationship between subjective fall risk assessment and falls and fall-related fractures in frail elderly people. BMC Geriatr. 2011, 11, 40. [Google Scholar] [CrossRef] [Green Version]
- Samuel, D.; Rowe, P.; Hood, V.; Nicol, A. The relationships between muscle strength, biomechanical functional moments and health-related quality of life in non-elite older adults. Age Ageing 2012, 41, 224–230. [Google Scholar] [CrossRef] [Green Version]
- Knapik, A.; Brzek, A.; Famula-Waz, A.; Gallert-Kopyto, W.; Szydlak, D.; Marcisz, C.; Plinta, R. The relationship between physical fitness and health self-assessment in elderly. Medicine (Baltimore) 2019, 98, e15984. [Google Scholar] [CrossRef]
- Singh, D.K.A.; Shahar, S.; Vanoh, D.; Kamaruzzaman, S.B.; Tan, M.P. Diabetes, arthritis, urinary incontinence, poor self-rated health, higher body mass index and lower handgrip strength are associated with falls among community-dwelling middle-aged and older adults: Pooled analyses from two cross-sectional Malaysian datasets. Geriatr. Gerontol. Int. 2019, 19, 798–803. [Google Scholar] [CrossRef]
- Cwikel, J.; Kaplan, G.; Barell, V. Falls and subjective health rating among the elderly: Evidence from two Israeli samples. Soc. Sci. Med. 1990, 31, 485–490. [Google Scholar] [CrossRef]
- Li, Q.; Mpofu, E.; Yin, C.; Turner, K.W. Perception of Falls and Confidence in Self-Management of Falls among Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 5054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knox, A. Fall Risk Perceptions: A Study of Hospitalized Patients with Hematologic Malignancies. Clin. J. Oncol. Nurs. 2018, 22, E159–E165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 2018 Population and Housing Census; Statistics Korea (KOSTAT): Daejeon, Korea, 2019.
- Chung, K. 2017 National Survey of Older Koreans: Findings and Implications; The Korea Institute for Health and Social Affairs: Seoul, Korea, 2018. [Google Scholar]
- WHO Guidelines Approved by the Guidelines Review Committee. In Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010.
- Allen, J.P.; Wilson, V.B. Assessing Alcohol Problems: A Guide for Clinicians and Researchers, 2nd ed.; NIH Publication: Bethesda, MD, USA, 2003.
- Won, C.W.; Yang, K.Y.; Rho, Y.G.; Kim, S.Y.; Lee, E.J.; Yoon, J.L. The development of Korean activities of daily living (K-ADL) and Korean instrumental activities of daily living (K-IADL) scale. J. Korean Geriatr. Soc. 2002, 6, 107–120. [Google Scholar]
- Dwyer, J. Strategies to detect and prevent malnutrition in the elderly: The Nutrition Screening Initiative. Nutr. Today 1994, 29, 14–24. [Google Scholar] [CrossRef]
- Cho, M.J.; Bae, J.N.; Suh, G.H.; Hahm, B.J.; Kim, J.K.; Lee, D.W.; Kang, M.H. Validation of geriatric depression scale, Korean version (GDS) in the assessment of DSM-III-R major depression. J. Korean Neuropsychiatr. Assoc. 1999, 38, 48–63. [Google Scholar]
- Lastrucci, V.; Lorini, C.; Rinaldi, G.; Bonaccorsi, G. Identification of fall predictors in the active elderly population from the routine medical records of general practitioners. Prim. Health Care Res. Dev. 2018, 19, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Van’t Hof, J.R.; Steffen, L.M.; Luepker, R.V. Estimation of Cardiovascular Risk from Self-Reported Knowledge of Risk Factors: Insights from the Minnesota Heart Survey. Clin. Epidemiol. 2020, 12, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Rantanen, A.T.; Korkeila, J.J.A.; Kautiainen, H.; Korhonen, P.E. Poor or fair self-rated health is associated with depressive symptoms and impaired perceived physical health: A cross-sectional study in a primary care population at risk for type 2 diabetes and cardiovascular disease. Eur. J. Gen. Pract. 2019, 25, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I.; Gayton, D. Measuring Balance in the Elderly: Preliminary Development of an Instrument; Physiotherapy Canada: Toronto, ON, Canada, 1989; Volume 41. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Downton, J.H. Falls in the Elderly; Edward Arnold: Stockport, UK, 1993. [Google Scholar]
- Oliver, D.; Britton, M.; Seed, P.; Martin, F.C.; Hopper, A.H. Development and evaluation of evidence based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: Case-control and cohort studies. BMJ 1997, 315, 1049–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrich, A.L.; Bender, P.S.; Nyhuis, A. Validation of the Hendrich II Fall Risk Model: A large concurrent case/control study of hospitalized patients. Appl. Nurs. Res. 2003, 16, 9–21. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Classification | Good | Poor | χ2 | p | |
|---|---|---|---|---|---|---|
| (n = 637) | (n = 940) | |||||
| n (%) or | n (%) or | |||||
| M ± SD * | M ± SD * | |||||
| Demographic | Age | 75.0 ± 6.3 | 76.2 ± 6.2 | 1191.31 | <0.001 | |
| Sex | Male | 208 (32.7) | 233 (24.8) | 11.66 | 0.001 | |
| Female | 429 (67.3) | 707 (75.2) | ||||
| Marital status | Living with spouse | 347 (54.5) | 433 (46.1) | 10.74 | 0.001 | |
| Living without spouse | 290 (45.5) | 507 (53.9) | ||||
| Living status | Alone | 193 (30.3) | 337 (35.8) | 12.14 | 0.007 | |
| Living with spouse | 285 (44.7) | 341 (36.3) | ||||
| Living with children | 138 (21.7) | 234 (24.9) | ||||
| Other | 21 (3.3) | 28 (3.0) | ||||
| Socio-economic | Education | 0–6 years | 410 (64.4) | 687 (73.1) | 32.95 | <0.001 |
| 7–9 years | 81 (12.7) | 127 (13.5) | ||||
| 10–12 years | 98 (15.4) | 104 (11.1) | ||||
| ≥13 years | 48 (7.5) | 22 (2.3) | ||||
| Quantiles of household income | Q1 (lowest) | 140 (22.0) | 312 (33.2) | 25.09 | <0.001 | |
| Q2 | 132 (20.7) | 182 (19.4) | ||||
| Q3 | 139 (21.8) | 180 (19.1) | ||||
| Q4 | 107 (16.8) | 134 (14.3) | ||||
| Q5 (highest) | 119 (18.7) | 132 (14.0) | ||||
| Health status | Disease | Hypertension | 368 (57.8) | 673 (71.6) | 32.35 | <0.001 |
| Diabetes | 109 (17.1) | 328 (34.9) | 59.94 | <0.001 | ||
| Dementia | 7 (1.1) | 33 (3.5) | 8.93 | 0.003 | ||
| Arthritis | 208 (32.7) | 517 (55.0) | 76.34 | <0.001 | ||
| BMI ** | Underweight (<18.5) | 27 (4.3) | 55 (5.9) | 6.39 | 0.094 | |
| Normal (≥18.5, <25) | 428 (67.1) | 583 (62.0) | ||||
| Overweight (≥25) | 182 (28.6) | 302 (32.1) | ||||
| Number of medication(s) | 0 | 128 (20.1) | 29 (3.1) | 258.00 | <0.001 | |
| 1 | 79 (12.4) | 29 (3.1) | ||||
| 2 | 104 (16.3) | 64 (6.8) | ||||
| ≥3 | 326 (51.2) | 818 (87.0) | ||||
| Health-related Behavior | Exercise | None | 183 (28.7) | 429 (45.6) | 53.67 | <0.001 |
| <150 min a week | 144 (22.6) | 206 (21.9) | ||||
| ≥150 min a week | 310 (48.7) | 305 (32.5) | ||||
| Smoking | Past/Never | 585 (91.8) | 872 (92.8) | 0.47 | 0.495 | |
| Current | 52 (8.2) | 68 (7.2) | ||||
| Drinking | None | 455 (71.4) | 794 (84.5) | 40.36 | <0.001 | |
| ≤1 standard drink/day | 79 (12.4) | 72 (7.6) | ||||
| >1 standard drink/day | 103 (16.2) | 74 (7.9) | ||||
| Physical & Psychological Variables | Classification | Good | Poor | χ2 | p | |
|---|---|---|---|---|---|---|
| (n = 637) | (n = 940) | |||||
| n (%) | n (%) | |||||
| Physical | Visual impairment | No | 410 (64.4) | 488 (51.9) | 24.00 | <0.001 |
| Yes | 227 (35.6) | 452 (48.1) | ||||
| Hearing impairment | No | 524 (82.3) | 656 (69.8) | 31.36 | <0.001 | |
| Yes | 113 (17.7) | 284 (30.2) | ||||
| ADL * limitation | No | 604 (94.8) | 738 (78.5) | 79.64 | <0.001 | |
| Yes | 33 (5.2) | 202 (21.5) | ||||
| IADL ** limitation | No | 502 (78.8) | 445 (47.3) | 156.71 | <0.001 | |
| Yes | 135 (21.2) | 495 (52.7) | ||||
| Nutrition | Good | 369 (57.9) | 284 (30.2) | 120.21 | <0.001 | |
| Poor | 268 (42.1) | 656 (69.8) | ||||
| Psychological | Depression | No | 540 (84.8) | 473 (50.3) | 196.19 | <0.001 |
| Yes | 97 (15.2) | 467 (49.7) | ||||
| Variables | Model I | Model II | Model III | Model IV |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Visual impairment | 1.31 (1.03–1.65) * | 1.30 (1.03–1.65) * | 1.26 (0.98–1.63) | 1.26 (0.99–3.42) |
| Hearing impairment | 1.51 (1.13–2.02) * | 1.50 (1.12–2.00) * | 1.51 (1.11–2.05) * | 1.51 (1.12–2.03) * |
| ADL limitation | 1.94 (1.256–3.00) * | 1.95 (1.28–3.05) * | 1.84 (1.16–2.91) * | 1.77 (1.11–2.81) * |
| IADL limitation | 2.66 (2.01–3.52) * | 2.62 (1.98–3.47) * | 2.34 (1.74–3.15) * | 2.27 (1.68–3.06) * |
| Poor nutrition | 1.89 (1.49–2.39) * | 1.87 (1.47–2.37) * | 1.36 (1.05–1.76) * | 1.36 (1.05–1.77) * |
| Depression | 3.84 (2.94–5.02) * | 3.68 (2.81–4.83) * | 3.87 (2.89–5.18) * | 3.77 (2.81–5.06) * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Byun, M.; Kim, M. Physical and Psychological Factors Associated with Poor Self-Reported Health Status in Older Adults with Falls. Int. J. Environ. Res. Public Health 2020, 17, 3548. https://doi.org/10.3390/ijerph17103548
Kim J, Byun M, Kim M. Physical and Psychological Factors Associated with Poor Self-Reported Health Status in Older Adults with Falls. International Journal of Environmental Research and Public Health. 2020; 17(10):3548. https://doi.org/10.3390/ijerph17103548
Chicago/Turabian StyleKim, Jiyeon, Mikyong Byun, and Moonho Kim. 2020. "Physical and Psychological Factors Associated with Poor Self-Reported Health Status in Older Adults with Falls" International Journal of Environmental Research and Public Health 17, no. 10: 3548. https://doi.org/10.3390/ijerph17103548
APA StyleKim, J., Byun, M., & Kim, M. (2020). Physical and Psychological Factors Associated with Poor Self-Reported Health Status in Older Adults with Falls. International Journal of Environmental Research and Public Health, 17(10), 3548. https://doi.org/10.3390/ijerph17103548