Sleep Quality, Anxiety, and Depression Are Associated with Fall Risk Factors in Older Women


 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
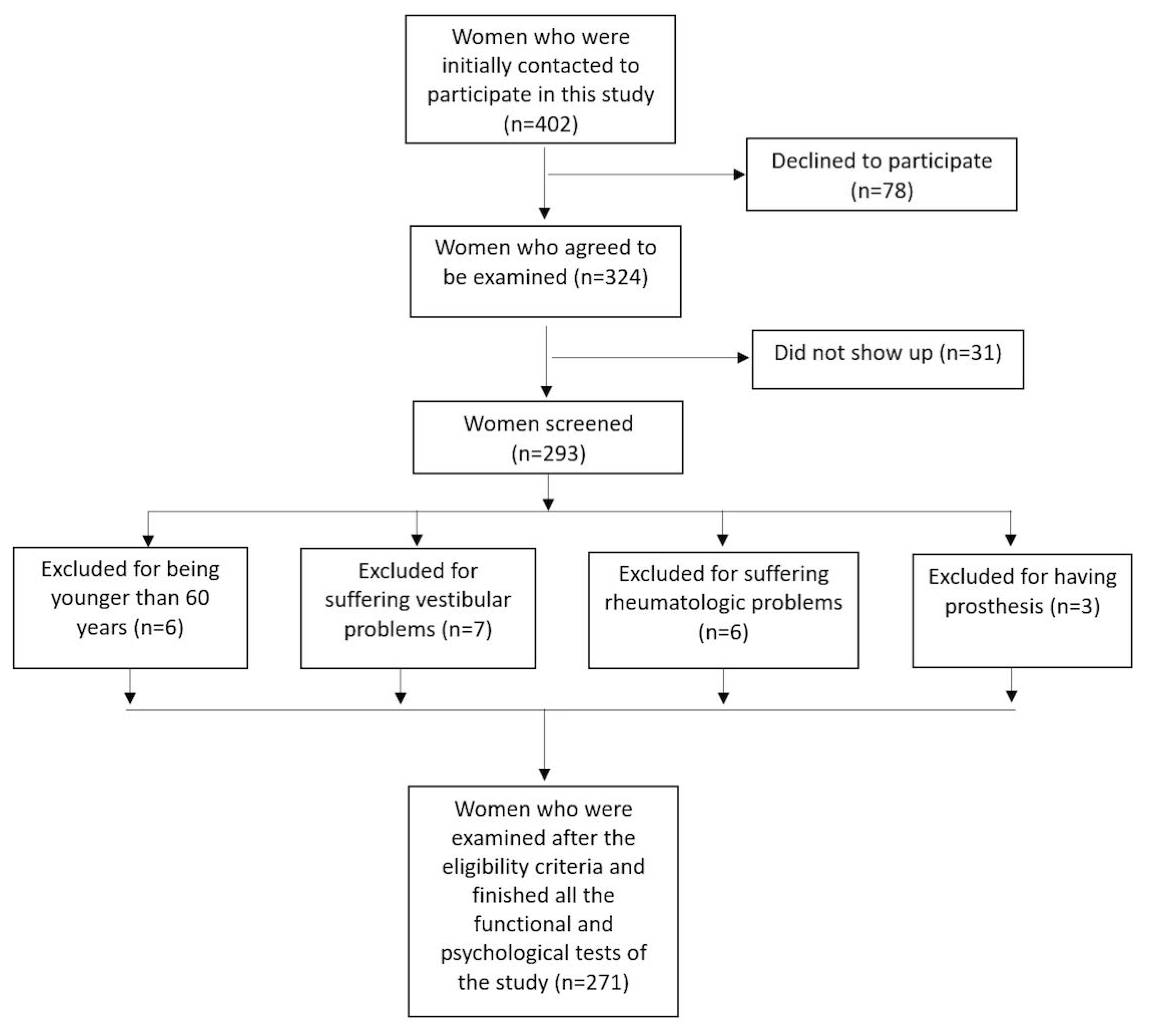
2.1. Study Participants
2.2. Outcomes
2.2.1. Sociodemographic and Anthropometric Data
2.2.2. Sleep Quality
2.2.3. Anxiety and Depression
2.2.4. Functional Mobility
2.2.5. Dynamic Balance
2.2.6. Gait Speed
2.3. Sample Size Calculation
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Terauchi, M.; Hiramitsu, S.; Akiyoshi, M.; Owa, Y.; Kato, K.; Obayashi, S.; Matsushima, E.; Kubota, T. Associations between anxiety, depression and insomnia in peri-and post-menopausal women. Maturitas 2012, 72, 61–65. [Google Scholar] [CrossRef]
- Llaneza, P.; García-Portilla, M.P.; Llaneza-Suárez, D.; Armott, B.; Pérez-López, F.R. Depressive disorders and the menopause transition. Maturitas 2012, 71, 120–130. [Google Scholar] [CrossRef]
- Naufel, M.F.; Frange, C.; Andersen, M.L.; Girão, M.J.B.C.; Tufik, S.; Beraldi Ribeiro, E.; Hachul, H. Association between obesity and sleep disorders in postmenopausal women. Menopause 2018, 25, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Shaver, J.L.; Woods, N.F. Sleep and menopause: A narrative review. Menopause 2015, 22, 899–915. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.E.; Stone, K.L.; Ancoli-Israel, S.; Blackwell, T.; Ewing, S.K.; Boudreau, R.; Cauley, J.A.; Newman, A.B. Poor sleep is associated with poorer physical performance and greater functional limitations in older women. Sleep 2007, 30, 1317–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hita-Contreras, F.; Zagalaz-Anula, N.; Martínez-Amat, A.; Cruz-Díaz, D.; Sánchez-Montesinos, I.; Aibar-Almazán, A.; Lomas-Vega, R. Sleep quality and its association with postural stability and fear of falling among Spanish postmenopausal women. Menopause 2018, 25, 62–69. [Google Scholar] [CrossRef]
- Wells, K.B.; Stewart, A.; Hays, R.D.; Burnam, M.A.; Rogers, W.; Daniels, M.; Berry, S.; Greenfield, S.; Ware, J. The functioning and well-being of depressed patients: Results from the Medical Outcomes Study. JAMA 1989, 262, 914–919. [Google Scholar] [CrossRef]
- Kouzis, A.C.; Eaton, W.W. Emotional disability days: Prevalence and predictors. Am. J. Public Health 1994, 84, 1304–1307. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; McGonagle, K.A.; Swartz, M.; Blazer, D.G.; Nelson, C.B. Sex and depression in the National Comorbidity Survey I: Lifetime prevalence, chronicity and recurrence. J. Affect Disord. 1994, 29, 85–96. [Google Scholar] [CrossRef] [Green Version]
- Amick, B.C., III; Kawachi, I.; Coakley, E.H.; Lerner, D.; Levine, S.; Colditz, G.A. Relationship of job strain and iso-strain to health status in a cohort of women in the United States. Scand. J. Work Environ. Health 1998, 24, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, P.J.; Murphy, J.H.; Haq, N.; Rubinow, D.R.; Danaceau, M.A. Stressful life events, personal losses, and perimenopause-related depression. Arch. Womens Ment. Health 2004, 7, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Caspi, A.; Sugden, K.; Moffitt, T.E.; Taylor, A.; Craig, I.W.; Harrington, H.; McClay, J.; Martin, J.; Braithwaite, A.; Poulton, R. Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science 2003, 301, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Woods, N.F.; Mariella, A.; Mitchell, E.S. Depressed mood symptoms during the menopausal transition: Observations from the Seattle Midlife Women’s Health Study. Climacteric 2006, 93, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Mulhall, S.; Andel, R.; Anstey, K.J. Variation in symptoms of depression and anxiety in midlife women by menopausal status. Maturitas 2018, 108, 7–12. [Google Scholar] [CrossRef]
- Mühlberg, W.; Sieber, C. Sarcopenia and frailty in geriatric patients: Implications for training and prevention. Z. Gerontol. Geriatr. 2004, 37, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.K.; Willetts, J.L.; Corns, H.L.; Marucci-Wellman, H.R.; Lombardi, D.A.; Courtney, T.K. Falls and fall-related injuries among community-dwelling adults in the United States. PLoS ONE 2016, 11, e0150939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granacher, U.; Muehlbaue, T.; Zahner, L.; Gollhofer, A.; Kressig, R.W. Comparison of traditional and recent approaches in the promotion of balance and strength in older adults. Sports Med. 2011, 41, 377–400. [Google Scholar] [CrossRef]
- Menant, J.C.; Schoene, D.; Sarofim, M.; Lord, S.R. Single and dual task tests of gait speed are equivalent in the prediction of falls in older people: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 16, 83–104. [Google Scholar] [CrossRef]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother. Res. Int. 2019, 24, e1743. [Google Scholar] [CrossRef] [Green Version]
- Lopes, K.T.; Costa, D.F.; Santos, L.F.; Castro, D.P.; Bastone, A.C. Prevalence of fear of falling among a population of older adults and its correlation with mobility, dynamic balance, risk and history of falls. Rev. Bras. Fisioter. 2009, 13, 223–229. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity: Preventing and Management of the Global Epidemic. Report of the WHO Consultation. Technical Report Series. No. 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatr. Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta. Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatr. 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Beekman, E.; Verhagen, A. Clinimetrics: Hospital anxiety and depression scale. J. Physiother. 2018, 64, 198. [Google Scholar] [CrossRef]
- Pisciottano, M.V.C.; Pinto, S.S.; Szejnfeld, V.L.; de Moura Castro, C.H. The relationship between lean mass, muscle strength and physical ability in independent healthy elderly women from the community. J. Nutr. Health Aging 2014, 18, 554–558. [Google Scholar] [CrossRef]
- Clark, S.; Parisi, J.; Kuo, J.; Carlson, M.C. Physical activity is associated with reduced risk of executive function impairment in older women. J. Aging Health 2016, 28, 726–739. [Google Scholar] [CrossRef]
- Piccoli, A.; Codognotto, M.; Piasentin, P.; Naso, A. Combined evaluation of nutrition and hydration in dialysis patients with bioelectrical impedance vector analysis (BIVA). Clin. Nutr. 2014, 33, 673–677. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Chauhan, K.; Sheth, M.; Vyas, N. Comparison of the effect of chair rising exercise and one-leg standing exercise on dynamic body balance in geriatrics: An experimental study. Indian. J. Phys. Ther. 2014, 2, 22–26. [Google Scholar]
- Carter, V.; Jain, T.; James, J.; Cornwall, M.; Aldrich, A.; de Heer, H.D. The 3-m backwards walk and retrospective falls: Diagnostic accuracy of a novel clinical measure. J. Geriatr. Phys. Ther. 2019, 42, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Concato, J.; Peduzzi, P.; Holford, T.R.; Feinstein, A.R. Importance of events per independent variable in proportional hazards analysis. I. Background, goals, and general strategy. J. Clin. Epidemiol. 1995, 48, 1495–1501. [Google Scholar] [CrossRef]
- Cohen, J.A. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-García, J.D.; Martínez-Amat, A.; De la Torre-Cruz, M.J.; Fábrega-Cuadros, R.; Cruz-Díaz, D.; Aibar-Almazán, A.; Achalandabaso-Ochoa, A.; Hita-Contreras, F. Suspension Training HIIT improves gait speed, strength and quality of life in older adults. Int. J. Sports Med. 2019, 40, 116–124. [Google Scholar] [CrossRef]
- Jiménez-García, J.D.; Hita-Contreras, F.; de la Torre-Cruz, M.; Fábrega-Cuadros, R.; Aibar-Almazán, A.; Cruz-Díaz, D.; Martínez-Amat, A. Risk of falls in healthy older adults: Benefits of high-intensity interval training using lower body suspension exercises. J. Aging Physical. Act. 2019, 27, 325–333. [Google Scholar] [CrossRef]
- Aibar-Almazán, A.; Hita-Contreras, F.; Cruz-Díaz, D.; de la Torre-Cruz, M.; Jiménez-García, J.D.; Martínez-Amat, A. Effects of Pilates training on sleep quality, anxiety, depression and fatigue in postmenopausal women: A randomized controlled trial. Maturitas 2019, 124, 62–67. [Google Scholar] [CrossRef]
- Pace-Schott, E.F.; Spencer, R.M. Age-Related changes in the cognitive function of sleep. Prog. Brain Res. 2011, 191, 75–89. [Google Scholar]
- Eysenck, M.W.; Derakshan, N.; Santos, R.; Calvo, M.G. Anxiety and cognitive performance: Attentional control theory. Emotion 2007, 7, 336. [Google Scholar] [CrossRef] [Green Version]
- Kurose, S.; Miyauchi, T.; Yamashita, R.; Tamaki, S.; Imai, M.; Nakashima, Y.; Umeda, Y.; Sato, S.; Kimura, Y.; Masuda, I. Association of locomotive activity with sleep latency and cognitive function of elderly patients with cardiovascular disease in the maintenance phase of cardiac rehabilitation. J. Cardiol. 2019, 73, 530–535. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Mera, R.M.; Sedler, M.J.; Zambrano, M.; Nieves, J.L.; Cagino, K.; Fanning, K.D.; Milla-Martínez, M.F.; Castillo, P.R. The effect of age in the association between frailty and poor sleep quality: A population-based study in community-dwellers (The Atahualpa Project). J. Med. Dir. Assoc. 2016, 17, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Jia, L.; Zhang, W.; Han, P.; Kang, L.; Ma, Y.; Yu, H.; Zhai, T.; Chen, X.; Guo, Q. The association between sleep duration and physical performance in Chinese community-dwelling elderly. PLoS ONE 2017, 12, e0174832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roepke, S.K.; Ancoli-Israel, S. Sleep disorders in the elderly. Indian J. Med. Res. 2010, 131, 302. [Google Scholar] [PubMed]
- Hill, E.L.; Cumming, R.G.; Lewis, R.; Carrington, S.; Couteur, D.G.L. Sleep disturbances and falls in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 62–66. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, D.; Neves, M. Falls Efficacy Scale-International: Exploring psychometric properties with adult day care users. Arch. Gerontol. Geriatr. 2018, 79, 145–150. [Google Scholar] [CrossRef]
- Herman, T.; Giladi, N.; Hausdorff, J.M. Properties of the ‘timed up and go’test: More than meets the eye. Gerontology 2011, 57, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Carral, J.M.C.; Ayan, C.; Sturzinger, L.; Gonzalez, G. Relationships between body mass index and static and dynamic balance in active and inactive older adults. J. Geriatr. Phys. Ther. 2019, 42, E85–E90. [Google Scholar] [CrossRef]
- Lin, C.H.; Liao, K.C.; Pu, S.J.; Chen, Y.C.; Liu, M.S. Associated factors for falls among the community-dwelling older people assessed by annual geriatric health examinations. PLoS ONE 2011, 6, e18976. [Google Scholar] [CrossRef]
- Follis, S.; Cook, A.; Bea, J.W.; Going, S.B.; Laddu, D.; Cauley, J.A.; Shadyab, A.H.; Stefanick, M.L.; Chen, Z. Association between sarcopenic obesity and falls in a multiethnic cohort of postmenopausal women. J. Am. Geriatr. Soc. 2018, 66, 2314–2320. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Values | ||
|---|---|---|---|
| Mean | SD | ||
| Age (years) | 69.18 | 5.69 | |
| Time since menopause (years) | 20.41 | 8.34 | |
| Waist circumference (cm) | 94.54 | 9.59 | |
| BMI (kg/m2) | 29.96 | 4.22 | |
| Frequency | Percentage | ||
| Occupational status | Retired | 221 | 81.54 |
| Working | 20 | 7.38 | |
| Unemployed | 30 | 11.07 | |
| Marital status | Single | 3 | 1.11 |
| Married/cohabiting | 160 | 59.04 | |
| Separated/divorced/Widowed | 108 | 39.85 | |
| Educational status | No formal education | 83 | 30.63 |
| Primary education | 138 | 50.92 | |
| Secondary education | 34 | 12.55 | |
| University | 16 | 5.90 | |
| Smoker | Yes | 11 | 4.06 |
| No | 260 | 95.94 | |
| Mean | SD | ||
| HADS Anxiety score | 6.86 | 4.21 | |
| HADS Depression score | 5.58 | 3.59 | |
| PSQI | Sleep quality | 1.14 | 0.83 |
| Sleep latency | 1.38 | 1.02 | |
| Sleep duration | 0.87 | 0.92 | |
| Sleep efficiency | 0.94 | 1.13 | |
| Sleep disturbances | 1.56 | 0.72 | |
| Use of sleeping medication | 1.02 | 1.33 | |
| Daytime dysfunction | 0.65 | 0.69 | |
| Total score | 7.57 | 4.31 | |
| Gait speed (m/s) | 1.16 | 0.27 | |
| TUG test (s) | 8.35 | 2.08 | |
| 3MTW (s) | 2.58 | 0.77 | |
| Variable | Gait Speed (m/s) | TUG Test (s) | 3MTW (s) | |
|---|---|---|---|---|
| PSQI | Sleep quality | −0.220 ** | 0.171 ** | 0.179 ** |
| Sleep latency | −0.197 ** | 0.162 ** | 0.161 ** | |
| Sleep duration | −0.133 * | −0.020 | −0.009 | |
| Sleep efficiency | −0.250 ** | 0.019 | 0.051 | |
| Sleep disturbances | −0.044 | 0.188 ** | 0.099 | |
| Use of sleeping medication | −0.170 ** | 0.198 ** | 0.110 | |
| Daytime dysfunction | −0.031 | 0.265 ** | 0.122 * | |
| Total score | −0.248 ** | 0.205 ** | 0.154 * | |
| HADS Anxiety score | −0.133 * | 0.318 ** | 0.270 ** | |
| HADS Depression score | −0.135 * | 0.294 ** | 0.283 ** | |
| Age (years) | −0.018 | 0.073 | 0.213 ** | |
| BMI (kg/m2) | −0.074 | 0.202 ** | 0.178 ** | |
| Waist circumference (cm) | −0.220 ** | 0.171 ** | 0.179 ** | |
| Variable | B | β | t | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|---|
| Gait speed (m/s) | Sleep efficiency | −0.05 | −0.23 | −3.79 | −0.08 | −0.03 | 0.000 |
| Use of sleeping medication | −0.03 | −0.13 | −2.15 | −0.05 | 0.00 | 0.032 | |
| TUG test (s) | Age | 0.10 | 0.29 | 5.04 | 0.06 | 0.15 | 0.000 |
| Depression | 0.10 | 0.18 | 3.05 | 0.04 | 0.17 | 0.003 | |
| Waist circumference | 0.03 | 0.14 | 2.47 | 0.01 | 0.06 | 0.014 | |
| Use of sleeping medication | 0.21 | 0.13 | 2.29 | 0.03 | 0.39 | 0.023 | |
| 3MTW (s) | Depression | 0.03 | 0.14 | 1.93 | 0.00 | 0.06 | 0.054 |
| Age | 0.03 | 0.21 | 3.65 | 0.01 | 0.04 | 0.000 | |
| Anxiety | 0.04 | 0.19 | 2.57 | 0.01 | 0.06 | 0.011 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano-Checa, R.; Hita-Contreras, F.; Jiménez-García, J.D.; Achalandabaso-Ochoa, A.; Aibar-Almazán, A.; Martínez-Amat, A. Sleep Quality, Anxiety, and Depression Are Associated with Fall Risk Factors in Older Women. Int. J. Environ. Res. Public Health 2020, 17, 4043. https://doi.org/10.3390/ijerph17114043
Serrano-Checa R, Hita-Contreras F, Jiménez-García JD, Achalandabaso-Ochoa A, Aibar-Almazán A, Martínez-Amat A. Sleep Quality, Anxiety, and Depression Are Associated with Fall Risk Factors in Older Women. International Journal of Environmental Research and Public Health. 2020; 17(11):4043. https://doi.org/10.3390/ijerph17114043
Chicago/Turabian StyleSerrano-Checa, Rodrigo, Fidel Hita-Contreras, José Daniel Jiménez-García, Alexander Achalandabaso-Ochoa, Agustín Aibar-Almazán, and Antonio Martínez-Amat. 2020. "Sleep Quality, Anxiety, and Depression Are Associated with Fall Risk Factors in Older Women" International Journal of Environmental Research and Public Health 17, no. 11: 4043. https://doi.org/10.3390/ijerph17114043
APA StyleSerrano-Checa, R., Hita-Contreras, F., Jiménez-García, J. D., Achalandabaso-Ochoa, A., Aibar-Almazán, A., & Martínez-Amat, A. (2020). Sleep Quality, Anxiety, and Depression Are Associated with Fall Risk Factors in Older Women. International Journal of Environmental Research and Public Health, 17(11), 4043. https://doi.org/10.3390/ijerph17114043