Integrated Family Planning and Immunization Service Delivery at Health Facility and Community Sites in Dowa and Ntchisi Districts of Malawi: A Mixed Methods Process Evaluation

 , , ,
, , ,
Abstract
:1. Introduction
- Is integration of family planning and immunization services at community sites and health facilities associated with a change in experience of care and uptake of modern contraception and routine infant immunization?
- How do contextual factors affect implementation, provision of care, and use of integrated services?
2. Materials and Methods
2.1. Quantitative Data Collection and Analysis
2.2. Qualitative Data Collection and Analysis
2.3. Ethics Approval and Consent to Participate
3. Results
3.1. Implementation of the Intervention
3.2. Effect of Integration on Service Delivery
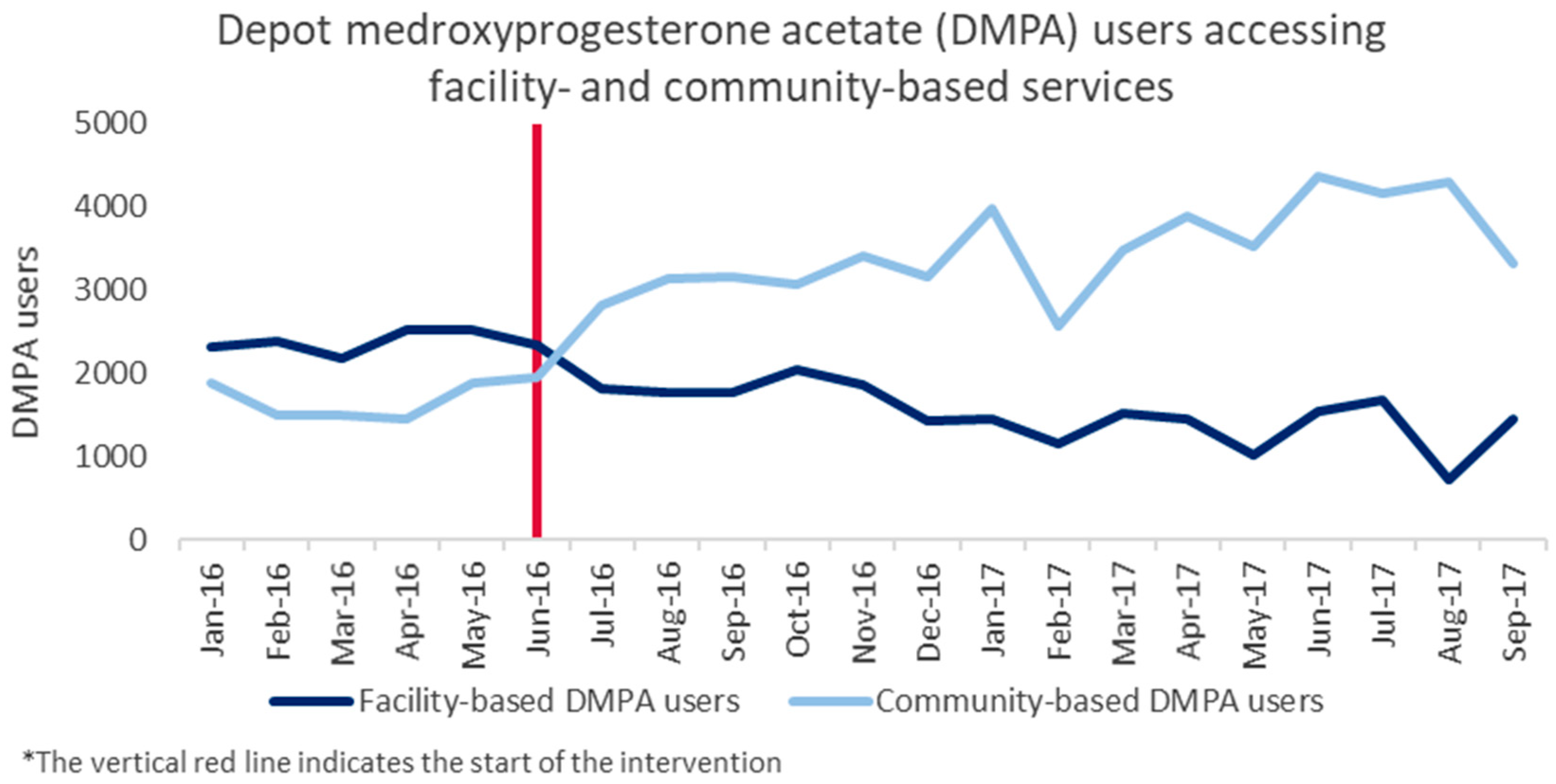
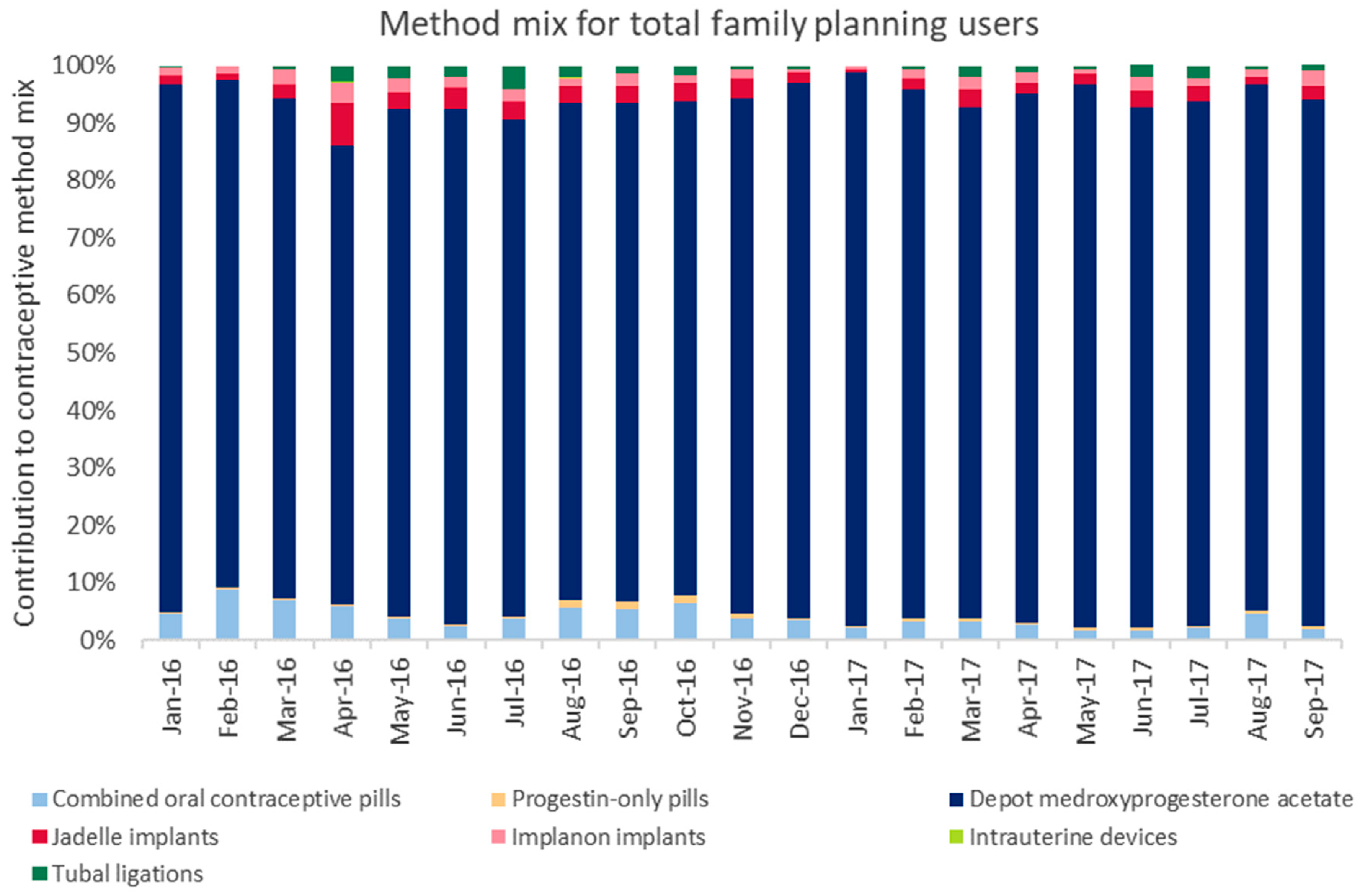
3.2.1. Family Planning
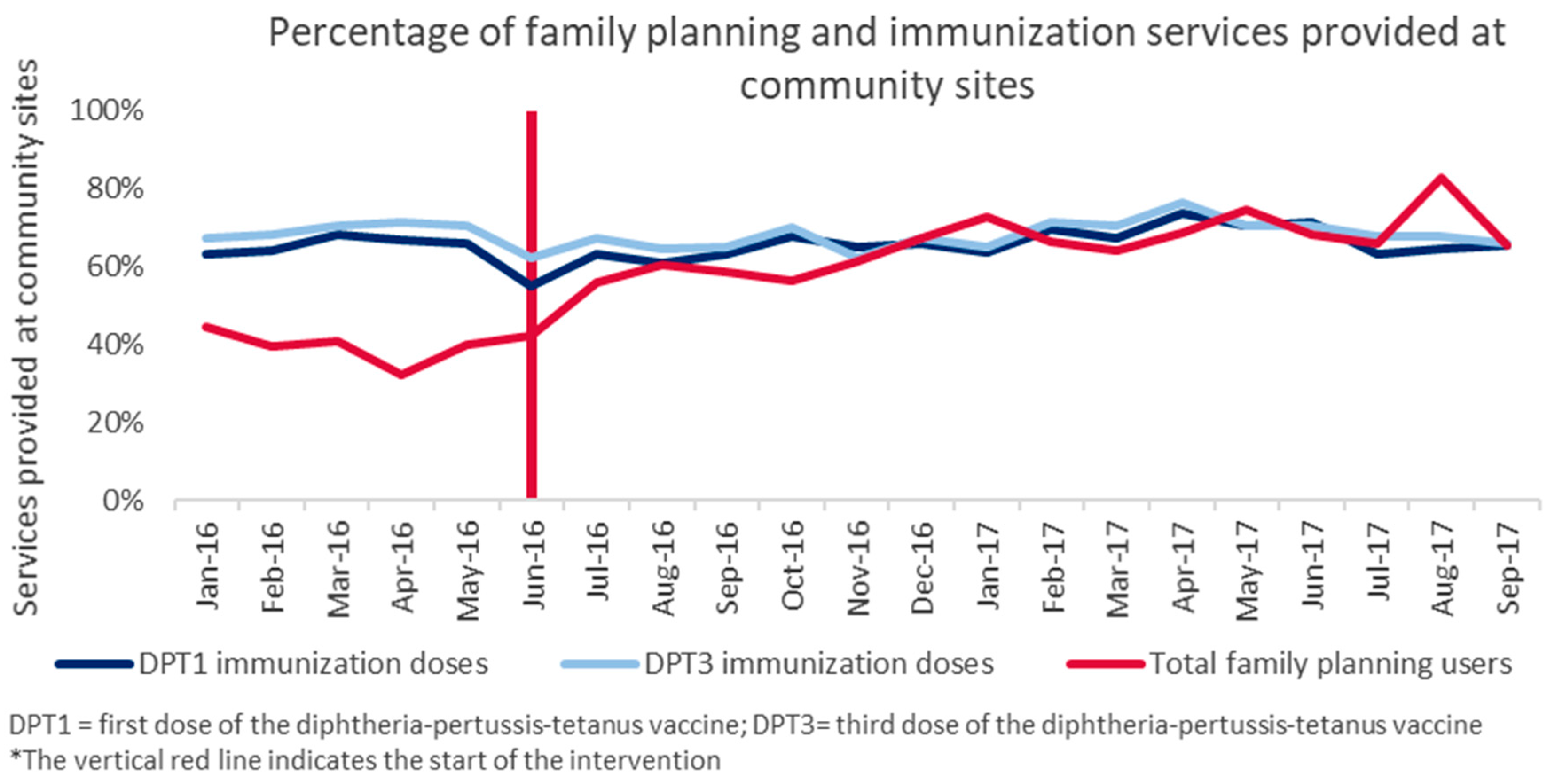
3.2.2. Immunization
3.3. Effect of Integration on Experience of Care
3.3.1. Benefits Perceived by Mothers and Fathers
There are some benefits because the baby gets immunized at the right time and I would also get my family planning at a good time, making me a happy and proud mum that my baby is growing healthy and I will be able to do other house chores.
This is very good because it has reduced the time the mothers were wasting instead of doing household chores due to coming different days for immunization and family planning services…. The health facility is also quite far in this area about 6 km so this integration is helping so the mother does not have to walk this distance twice to access the care. The men also escort the women to the hospital for these services, so the integration is also giving us [men] time to do some businesses and going the field to farm.
3.3.2. Challenges Perceived by Mothers and Fathers
Immunization comes from very far… [and] comes here late so we end up leaving this place very late. Our friends who are not immunizing their babies that day are long gone while we are still busy with immunization.
If we delay just by a little time we are told to go back home and come the next month.
3.3.3. Provider Perspectives
… before there was no integration; everyone was just concentrating on what they are doing. If it’s about family planning we would just assist the woman on family planning with no concern on the child; same way for those doing growth monitoring in the children, there would be no concern if she is doing family planning, but now they access all services so they save time and have no excuse.
The workload increases; we are few health workers here. Another thing is that people are kept waiting for longer, if you are alone then you have to give family planning and then you should take them for immunization, and search for someone who has to help them with that if you find that there is no one there.
3.4. Contextual Factors Affecting Implementation and Integration Outcomes
3.4.1. Commodity Availability
3.4.2. Community Linkages
To increase community sensitization to take a leading role we already started meeting with GVHs [group village headmen/women] to help us with sensitizing the community so that there should be uptake of services so that the community should know that when they go for vaccination service they can also receive family planning services…
3.4.3. Family Planning Concerns and Norms
If they hear rumors and have some fears about family planning, some women may not access the services… for example, people say that when you are taking family planning methods, it means you will never have a child, so there is need to dispel those rumors. If you counsel the person properly, she understands.
3.4.4. Partner Engagement and Male Involvement
In my view, I think the problems are coming due to lack of male involvement; there are some men that are restricting their wives from accessing family planning services so women have devised to use two health passports [client-held health records] where one health passport is strictly for family planning services; in that way the husband does not know that the wife is on family planning.
4. Discussion
Programs at this stage need to focus on long-term sustainability, continued improvements in service quality, and expanding the range of methods available. At this stage, rather than focusing on further growth, goals and objectives should be focused on equity indicators and government financial commitments.[3]
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Family Planning/Contraception. Available online: https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception (accessed on 17 May 2020).
- National Statistical Office (NSO) [Malawi]; ICF. Malawi Demographic and Health Survey 2015–16. Zomba, Malawi, and Rockville, Maryland, USA: NSO and ICF; 2017. Available online: https://dhsprogram.com/pubs/pdf/FR319/FR319.pdf (accessed on 5 March 2019).
- Exploring Opportunities for mCPR Growth in Malawi. Track20.org. 2017. Available online: http://www.track20.org/download/pdf/2017%20Opportunity%20Briefs/english/Malawi%20FP%20Opportunity%20Brief.pdf (accessed on 5 March 2019).
- Health Sector Strategic Plan II (2017–2022). Lilongwe: Malawi Ministry of Health; April 2017. Available online: http://www.nationalplanningcycles.org/sites/default/files/planning_cycle_repository/malawi/health_sector_strategic_plan_ii_030417_smt_dps.pdf (accessed on 6 December 2017).
- Government of Malawi. Malawi Costed Implementation Plan for Family Planning, 2016–2020; Government of Malawi: Lilongwe, Malawi, 2015. Available online: https://www.healthpolicyproject.com/ns/docs/Malawi_CIP_FINAL.pdf (accessed on 6 December 2017).
- USAID. Family Planning and Immunization Integration: Reaching Postpartum Women with Family Planning Services. In High-Impact Practices in Family Planning (HIP); USAID: Washington, DC, USA, 2013. Available online: http://www.fphighimpactpractices.org/briefs/family-planning-and-immunization-integration (accessed on 6 December 2017).
- Cooper, C.; Fields, R.; Mazzeo, C.; Taylor, N.; Pfitzer, A.; Momolu, M.; Jabbeh-Howe, C. Successful Proof of Concept of Family Planning and Immunization Integration in Liberia. Glob. Health Sci. Pract. 2015, 3, 71–84. Available online: http://www.ghspjournal.org/content/3/1/71 (accessed on 6 December 2017). [CrossRef] [PubMed] [Green Version]
- National Statistical Office [Malawi]. Statistical Yearbook 2015. Available online: http://www.nsomalawi.mw/images/stories/data_on_line/general/yearbook/2015%20Statistical%20Yearbook.pdf (accessed on 6 December 2017).
- Nelson, A.R.; Cooper, C.M.; Kamara, S.; Taylor, N.D.; Zikeh, T.; Kanneh-Kesselly, C.; Fields, R.; Hossain, I.; Oseni, L.; Getahun, B.S.; et al. Operationalizing Integrated Immunization and Family Planning Services in Rural Liberia: Lessons Learned from Evaluating Service Quality and Utilization. Glob. Health Sci. Pract. 2019, 7, 418–434. [Google Scholar] [CrossRef] [Green Version]
- Dulli, L.; Eichleay, M.; Rademacher, K.; Sortijas, S.; Nsengiyumva, T. Meeting Postpartum Women’s Family Planning Needs Through Integrated Family Planning and Immunization Services: Results of a Cluster-Randomized Controlled Trial in Rwanda. Glob. Health Sci. Pract. 2016, 4, 73–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huntington, D.; Aplogan, A. The Integration of Family Planning and Childhood Immunization Services in Togo. Stud. Fam. Plan. 1994, 25, 176. [Google Scholar] [CrossRef]
- Malawi Ministry of Health. Family Planning Register; Malawi Ministry of Health: Lilongwe, Malawi, 2013.
- World Health Organization. Immunization in Practice. A Practical Guide for Health Staff. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/193412/9789241549097_eng.pdf;jsessionid=5E715EB3FE5B1F7A6531A156D7E9BC2C?sequence=1 (accessed on 5 March 2019).
- Michaels-Igbokwe, C.; Terris-Prestholt, F.; Lagarde, M.; Chipeta, E.; The Integra Initiative; Cairns, J. Young People’s Preferences for Family Planning Service Providers in Rural Malawi: A Discrete Choice Experiment. PLoS ONE 2015, 12, e0143287. [Google Scholar] [CrossRef]
- Burke, H.; Chen, M.; Buluzi, M.; Fuchs, R.; Wevill, S.; Venkatasubramanian, L.; Santo, L.D.; Ngwira, B. Effect of self-administration versus provider-administered injection of subcutaneous depot medroxyprogesterone acetate on continuation rates in Malawi: A randomised controlled trial. Lancet Glob. Health 2018, 6, e568–e578. [Google Scholar] [CrossRef] [Green Version]
- Charyeva, Z.; Oguntunde, O.; Orobaton, N.; Otolorin, E.; Inuwa, F.; Alalade, O.; Abegunde, D.; Danladi, S. Task Shifting Provision of Contraceptive Implants to Community Health Extension Workers: Results of Operations Research in Northern Nigeria. Glob. Health Sci. Pract. 2015, 3, 382–394. [Google Scholar] [CrossRef] [Green Version]
- Pattanaik, A.; Mohan, D.; Chipokosa, S.; Wachepa, S.; Katengeza, H.; Misomali, A.; Marx, M.A. Testing the validity and feasibility of using a mobile phone-based method to assess the strength of implementation of family planning programs in Malawi. BMC Health Serv. Res. 2020, 20, 221. [Google Scholar] [CrossRef] [PubMed]
- Government of Malawi. EPI Comprehensive Multi-Year Plan (cMYP) 2016–2020. September 2015. Available online: http://www.nationalplanningcycles.org/sites/default/files/planning_cycle_repository/malawi/malawi_cmyp_2016-2020.pdf (accessed on 6 December 2017).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Collection Activity | Participant Type | Number of Participants: Dowa | Number of Participants: Ntchisi | Number of Participants: Total (Dowa + Ntchisi) |
|---|---|---|---|---|
| Focus group discussions | Men with infants < 1 year | 1 FGD (7 respondents) | 1 FGD (6 respondents) | 2 FGD (13 respondents) |
| Women with infants < 1 year who accepted immunization referrals | 4 FGDs (36 respondents) | 4 FGDs (23 respondents) | 8 FGDs (59 respondents) | |
| Women with infants < 1 year who accepted FP referrals | 8 FGDs (48 respondents) | 8 FGDs (64 respondents) | 16 FGDs (112 respondents) | |
| Women with infants < 1 year who declined FP referrals | 8 FGDs (37 respondents) | 3 FGDs (20 respondents) | 11 FGDs (57 respondents) | |
| In-depth interviews | Women with infants < 1 year who declined FP referrals | 0 | 3 | 3 |
| Community-based HSAs | 2 | 2 | 4 | |
| Facility-based HSAs | 4 | 4 | 8 | |
| FP providers (nurses) | 4 | 4 | 8 | |
| Facility supervisors | 4 | 3 | 7 | |
| Program managers: district | 3 | 3 | 6 | |
| Program managers: national | 2 | |||
| Indicator | Coefficient * | Standard Error | 95% Confidence Interval | Rho |
|---|---|---|---|---|
| New community-based FP users | 12.0 | 2.43 | 7.12–16.86 | 0.328 |
| Total community-based FP users | 186.6 | 23.86 | 138.8–234.4 | 0.350 |
| New facility-based FP users | −9.0 | 5.3 | −19.6–1.5 | 0.376 |
| Total facility-based FP users | −63.3 | 16.3 | −95.9–−30.7 | 0.512 |
| All new FP users | 2.9 | 5.4 | −8.9–13.9 | 0.390 |
| All FP users | 123.3 | 24.5 | 74.2–172.4 | 0.571 |
| DPT1 doses | 3.1 | 2.6 | −2.1–8.2 | 0.875 |
| DPT3 doses | 9.2 | 2.9 | 3.4–15.0 | 0.810 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cooper, C.M.; Wille, J.; Shire, S.; Makoko, S.; Tsega, A.; Schuster, A.; Hausi, H.; Gibson, H.; Tappis, H. Integrated Family Planning and Immunization Service Delivery at Health Facility and Community Sites in Dowa and Ntchisi Districts of Malawi: A Mixed Methods Process Evaluation. Int. J. Environ. Res. Public Health 2020, 17, 4530. https://doi.org/10.3390/ijerph17124530
Cooper CM, Wille J, Shire S, Makoko S, Tsega A, Schuster A, Hausi H, Gibson H, Tappis H. Integrated Family Planning and Immunization Service Delivery at Health Facility and Community Sites in Dowa and Ntchisi Districts of Malawi: A Mixed Methods Process Evaluation. International Journal of Environmental Research and Public Health. 2020; 17(12):4530. https://doi.org/10.3390/ijerph17124530
Chicago/Turabian StyleCooper, Chelsea M., Jacqueline Wille, Steven Shire, Sheila Makoko, Asnakew Tsega, Anne Schuster, Hannah Hausi, Hannah Gibson, and Hannah Tappis. 2020. "Integrated Family Planning and Immunization Service Delivery at Health Facility and Community Sites in Dowa and Ntchisi Districts of Malawi: A Mixed Methods Process Evaluation" International Journal of Environmental Research and Public Health 17, no. 12: 4530. https://doi.org/10.3390/ijerph17124530