Acute Effects of Open Kinetic Chain Exercise Versus Those of Closed Kinetic Chain Exercise on Quadriceps Muscle Thickness in Healthy Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
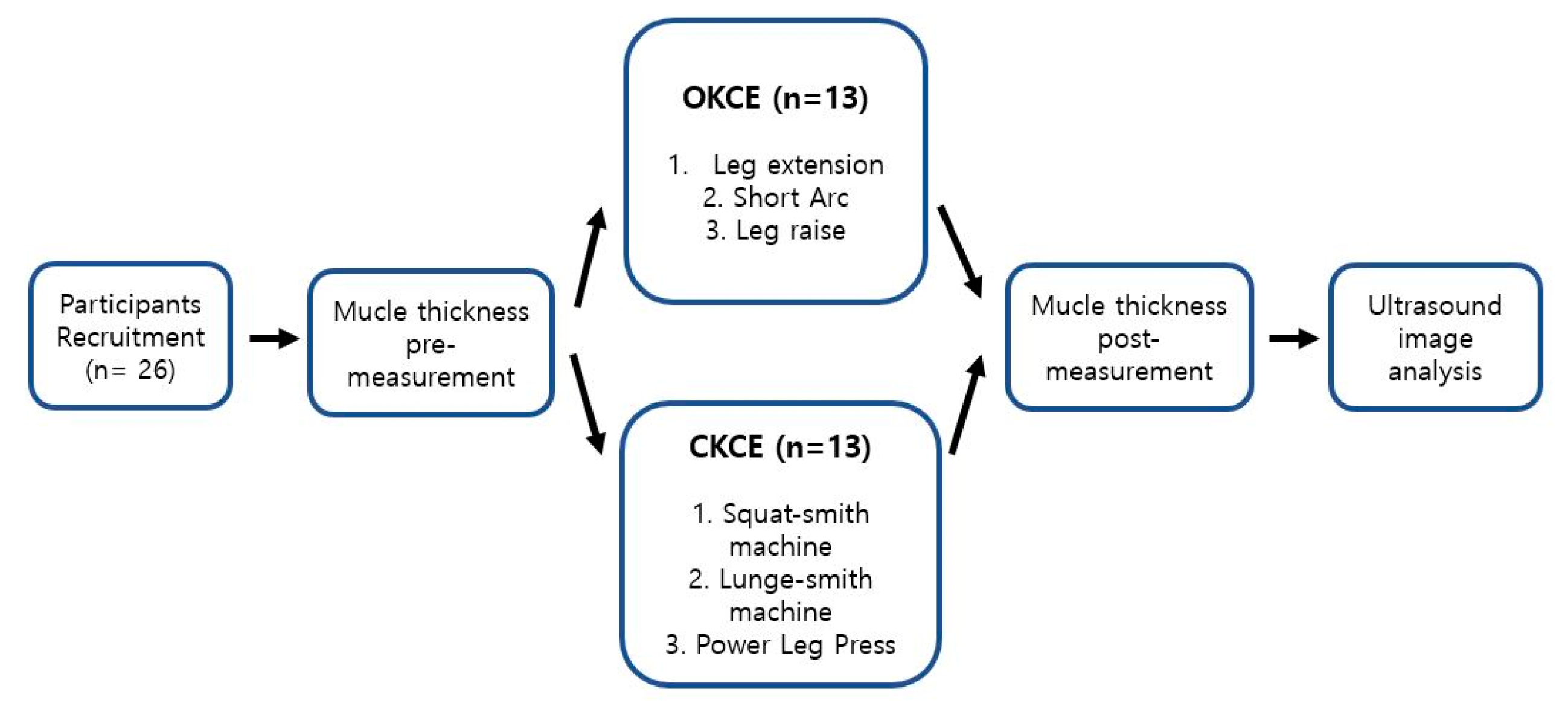
2.2. Study Design
2.3. Experimental Methods
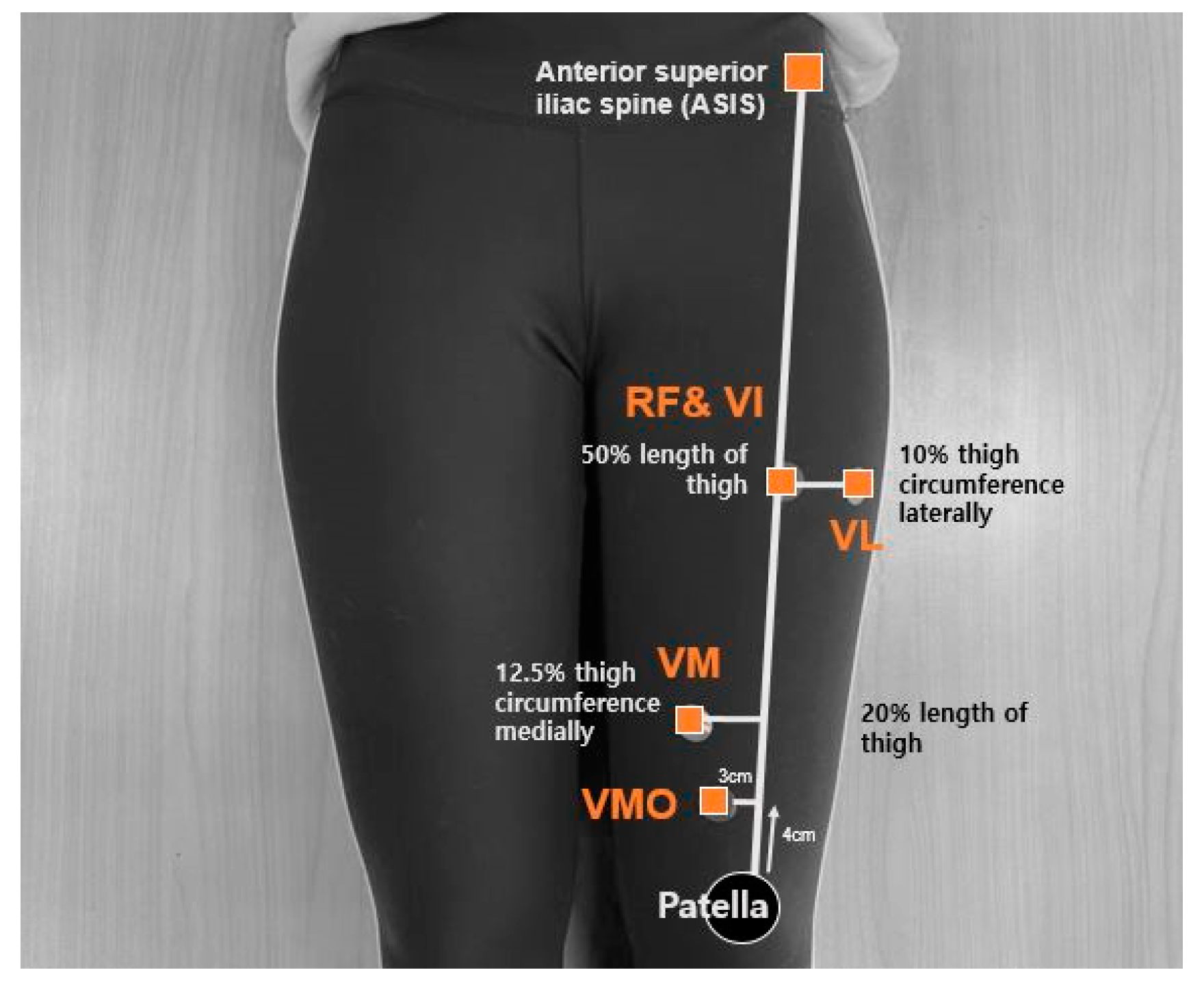
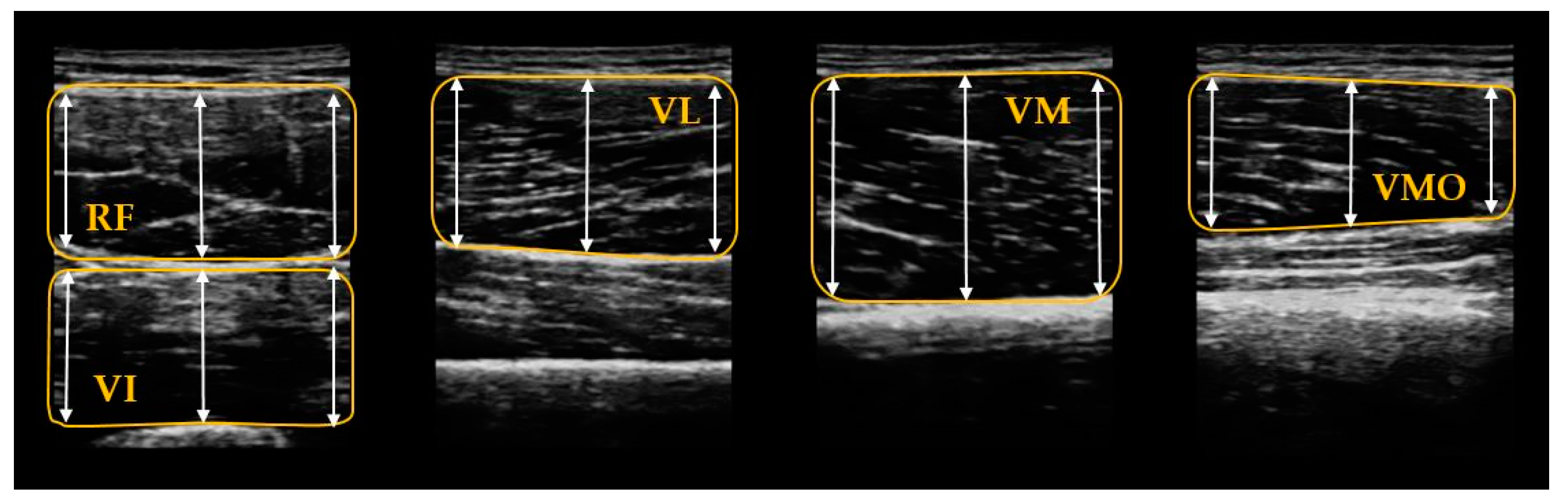
2.3.1. Muscular Thickness Measurement
2.3.2. Exercise
2.3.3. Open Kinetic Chain Exercise
- Leg extension exercise
- Participants were positioned on the center of the back of a machine such that their thighs, backs, and heads were not tilted on one side. Their knees were aligned in a straight line along the axis of the machine and their hips and thighs were positioned such that the back of their knees touched the edge of the chair. The starting position was set at a flexion of 90°. The knees of the participants were not in hyperextension or hyperflexion during the exercise and their upper body was stationary [27].
- Short-arc exercise
- The short-arc exercise was performed using a knee extension exercise machine. Although the participant was positioned in the same way as that of the leg extension exercise, the starting position of the knee was at a flexion of 20°. Participants performed knee extensions and a hold of 2–3 s in the fully extended position.
- Leg Raises Exercise
- Sandbags with a predetermined weight of 10 RM were attached to ankle of each of the participant. They initiated a straight leg raise while lying on the table with both hands on their chest and one leg extended. The other leg was stabilized at the knee flexed with 90°.
2.3.4. Closed Kinetic Chain Exercise
- Squat—Smith machine
- Participants were made to stand while they held a bar in pronation grip across their shoulders. Their feet were positioned at a slightly wider distance than the shoulders and toes were pointed slightly outside. The participants initiated the exercise in the squat position while slowly flexing their hips and knees and keeping the body angle constant [27].
- Lunge—Smith machine
- Participants were made to stand and a bar was placed above the posterior deltoid and upper trapezius in pronation grip that was wider than their shoulder. They maintained a straight posture and one foot was placed forward and the other was placed behind. Their front leg was horizontal to the floor and their rear leg was vertical to the floor, while the knees and hips of their front legs were bent gradually. They were instructed not to bend the front knee past the front foot and not to bend the trunk forward. The trial was repeated if this requirement was not met [27].
- Leg press machine
- Participants were positioned on the center of the back of a machine such that their thigh, back, and head were not tilted on one side and they held the handle on both sides. Their knees were extended and their feet were positioned above the footpad within shoulder width. Participants were seated at an angle of approximately 120°. The knee of each participant extended and protracted back to the starting position. The heels of the participants remained on the footpads and the knees were not in hyperextension or hyperflexion. The upper body of the participants remained stationary [27].
2.3.5. Ultrasound Image Analysis
2.4. Statistical Analysis
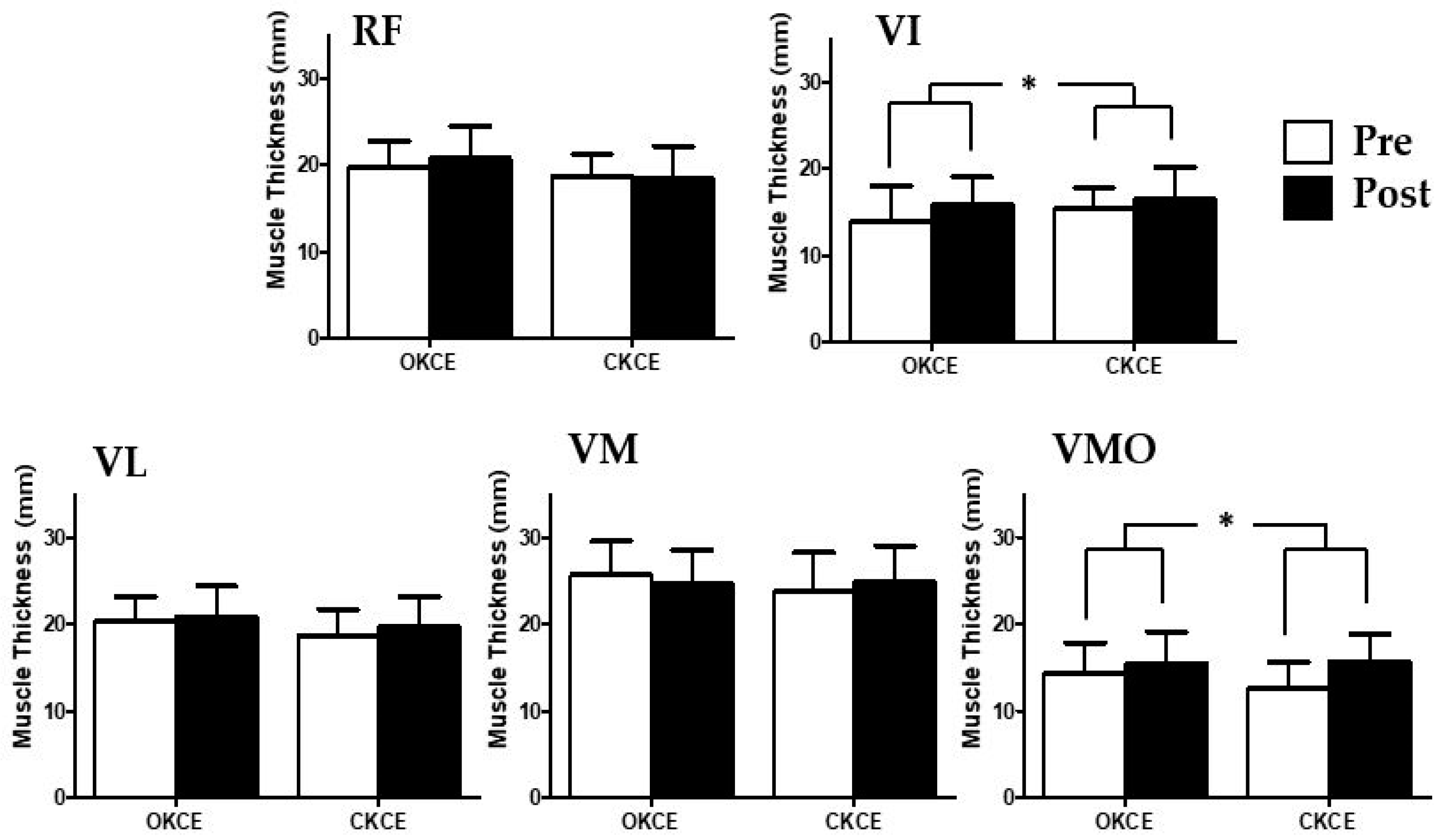
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Callaghan, M.; Oldham, J. Quadriceps atrophy: To what extent does it exist in patellofemoral pain syndrome? Br. J. Sports Med. 2004, 38, 295–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynch, A.D.; Logerstedt, D.S.; Axe, M.J.; Snyder-Mackler, L. Quadriceps activation failure after anterior cruciate ligament rupture is not mediated by knee joint effusion. J. Orthop. Sports Phys. Ther. 2012, 42, 502–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suter, E.; Herzog, W.; De Souza, K.; Bray, R. Inhibition of the quadriceps muscles in patients with anterior knee pain. J. Appl. Biomech. 1998, 14, 360–373. [Google Scholar] [CrossRef]
- Werner, S. An evaluation of knee extensor and knee flexor torques and EMGs in patients with patellofemoral pain syndrome in comparison with matched controls. Knee Surg. Sports Traumatol. Arthrosc. 1995, 3, 89–94. [Google Scholar] [CrossRef]
- Chmielewski, T.L.; Stackhouse, S.; Axe, M.J.; Snyder-Mackler, L. A prospective analysis of incidence and severity of quadriceps inhibition in a consecutive sample of 100 patients with complete acute anterior cruciate ligament rupture. J. Orthop. Res. 2004, 22, 925–930. [Google Scholar] [CrossRef]
- Eitzen, I.; Moksnes, H.; Snyder-Mackler, L.; Risberg, M.A. A progressive 5-week exercise therapy program leads to significant improvement in knee function early after anterior cruciate ligament injury. J. Orthop. Sports Phys. Ther. 2010, 40, 705–721. [Google Scholar] [CrossRef] [Green Version]
- Liu-Ambrose, T.; Taunton, J.; MacIntyre, D.; McConkey, P.; Khan, K. The effects of proprioceptive or strength training on the neuromuscular function of the ACL reconstructed knee: A randomized clinical trial. Scand. J. Med. Sci. Sports 2003, 13, 115–123. [Google Scholar] [CrossRef]
- Wilk, K.E.; Romaniello, W.T.; Soscia, S.M.; Arrigo, C.A.; Andrews, J.R. The relationship between subjective knee scores, isokinetic testing, and functional testing in the ACL-reconstructed knee. J. Orthop. Sports Phys. Ther. 1994, 20, 60–73. [Google Scholar] [CrossRef]
- Hyoungsu, K.; Eunyoung, K.; Jiwon, H. The effects of quadriceps femoris muscle activation by closed and open kinetic chain exercise. J. Korean Soc. Integr. Med. 2015, 3, 71–80. [Google Scholar]
- Hubbard, J.K.; Sampson, H.W.; Elledge, J.R. Prevalence and morphology of the vastus medialis oblique muscle in human cadavers. Anat. Rec. 1997, 249, 135–142. [Google Scholar] [CrossRef]
- Irish, S.E.; Millward, A.J.; Wride, J.; Haas, B.M.; Shum, G.L. The effect of closed-kinetic chain exercises and open-kinetic chain exercise on the muscle activity of vastus medialis oblique and vastus lateralis. J. Strength Cond. Res. 2010, 24, 1256–1262. [Google Scholar] [CrossRef] [PubMed]
- Souza, D.R.; Gross, M.T. Comparison of vastus medialis obliquus: Vastus lateralis muscle integrated electromyographic ratios between healthy subjects and patients with patellofemoral pain. Phys. Ther. 1991, 71, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.-M. Recording the vastii muscle onset timing as a diagnostic parameter for patellofemoral pain syndrome: Fact or fad? Phys. Ther. Sport 2009, 10, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Fleisig, G.S.; Zheng, N.; Barrentine, S.W.; Wilk, K.E.; Andrews, J.R. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med. Sci. Sports Exer. 1998, 30, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Kisner, C.; Colby, L. Therapeutic Exercise: Foundations and Techniques; FA Davis Co: Philadelphia, PA, USA, 2007. [Google Scholar]
- Iwasaki, T.; Shiba, N.; Matsuse, H.; Nago, T.; Umezu, Y.; Tagawa, Y.; Nagata, K.; Basford, J.R. Improvement in knee extension strength through training by means of combined electrical stimulation and voluntary muscle contraction. Tohoku J. Exp. Med. 2006, 209, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Kwon, Y.J.; Bae, S.S.; Park, S.J. The Effect of Static Balance Recovery by Open Kinetic Chain and Closed Kinetic Chain Exercises. J. Korean Soc. Phys. Ther. 2009, 4, 23–30. [Google Scholar]
- Han, S.W. A SEMG analysis of knee joint angle during close kinetic chain exercise and open kinetic chain exercises in quadriceps muscle. J. Korean Soc. Phys. Ther. 2004, 16, 192–204. [Google Scholar]
- Ando, R.; Saito, A.; Umemura, Y.; Akima, H. Local architecture of the vastus intermedius is a better predictor of knee extension force than that of the other quadriceps femoris muscle heads. Clin. Physiol. Funct. Imaging 2015, 35, 376–382. [Google Scholar] [CrossRef]
- Cheon, S.; Chang, E. Inter-rater Reliability of a Portable Ultrasound for the Quadriceps and Hamstrings Thickness Measurement in Healthy Adults. Exerc. Sci. 2020, 29, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Ruas, C.V.; Pinto, R.S.; Lima, C.D.; Costa, P.B.; Brown, L.E. Test-retest reliability of muscle thickness, echo-intensity and cross sectional area of quadriceps and hamstrings muscle groups using B-mode ultrasound. Int. J. Kinesiol. Sports Sci. 2017, 5, 35–41. [Google Scholar] [CrossRef] [Green Version]
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.; van Cingel, R.E. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, H.; Tedner, B.; Tesch, P. Changes in lower limb muscle cross-sectional area and tissue fluid volume after transition from standing to supine. Acta Physiol. Scand. 1993, 148, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.S.; Correa, C.S.; Radaelli, R.; Cadore, E.L.; Brown, L.E.; Bottaro, M. Short-term strength training improves muscle quality and functional capacity of elderly women. AGE 2014, 36, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Giles, L.; Webster, K.; McClelland, J.; Cook, J. Can ultrasound measurements of muscle thickness be used to measure the size of individual quadriceps muscles in people with patellofemoral pain? Phys. Ther. Sport 2015, 16, 45–52. [Google Scholar] [CrossRef]
- Miao, P.; Xu, Y.; Pan, C.; Liu, H.; Wang, C. Vastus medialis oblique and vastus lateralis activity during a double-leg semisquat with or without hip adduction in patients with patellofemoral pain syndrome. BMC Musculoskelet. Disord. 2015, 16, 289. [Google Scholar] [CrossRef]
- Coburn, J.W.; Malek, M.H. NSCA’s Essentials of Personal Training, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- Ouellette, M.M.; LeBrasseur, N.K.; Bean, J.F.; Phillips, E.; Stein, J.; Frontera, W.R.; Fielding, R.A. High-intensity resistance training improves muscle strength, self-reported function, and disability in long-term stroke survivors. Stroke 2004, 35, 1404–1409. [Google Scholar] [CrossRef] [Green Version]
- Scanlon, T.C.; Fragala, M.S.; Stout, J.R.; Emerson, N.S.; Beyer, K.S.; Oliveira, L.P.; Hoffman, J.R. Muscle architecture and strength: Adaptations to short-term resistance training in older adults. Muscle Nerve 2014, 49, 584–592. [Google Scholar] [CrossRef]
- Cadore, E.L.; Izquierdo, M.; Conceição, M.; Radaelli, R.; Pinto, R.S.; Baroni, B.M.; Vaz, M.A.; Alberton, C.L.; Pinto, S.S.; Cunha, G. Echo intensity is associated with skeletal muscle power and cardiovascular performance in elderly men. Exp. Gerontol. 2012, 47, 473–478. [Google Scholar] [CrossRef]
- Rosenberg, J.G.; Ryan, E.D.; Sobolewski, E.J.; Scharville, M.J.; Thompson, B.J.; King, G.E. Reliability of panoramic ultrasound imaging to simultaneously examine muscle size and quality of the medial gastrocnemius. Muscle Nerve 2014, 49, 736–740. [Google Scholar] [CrossRef]
- Palmer, T.B.; Akehi, K.; Thiele, R.M.; Smith, D.B.; Thompson, B.J. Reliability of panoramic ultrasound imaging in simultaneously examining muscle size and quality of the hamstring muscles in young, healthy males and females. Ultrasound Med. Biol. 2015, 41, 675–684. [Google Scholar] [CrossRef]
- Rech, A.; Radaelli, R.; Goltz, F.R.; da Rosa, L.H.T.; Schneider, C.D.; Pinto, R.S. Echo intensity is negatively associated with functional capacity in older women. Age 2014, 36, 9708. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, C.; Tamaki, A.; Yamada, E.; Matsuoka, H. Influence of gender on muscle fatigue during dynamic knee contractions. Phys. Ther. Res. 2017, 20, E9889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical power analysis. Curr. Direct. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Thomas, A.C.; Wojtys, E.M.; Brandon, C.; Palmieri-Smith, R.M. Muscle atrophy contributes to quadriceps weakness after anterior cruciate ligament reconstruction. J. Sci. Med. Sport 2016, 19, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Wurtzel, C.N.; Gumucio, J.P.; Grekin, J.A.; Khouri, R.K., Jr.; Russell, A.J.; Bedi, A.; Mendias, C.L. Pharmacological inhibition of myostatin protects against skeletal muscle atrophy and weakness after anterior cruciate ligament tear. J. Orthop. Res. 2017, 35, 2499–2505. [Google Scholar] [CrossRef]
- Panagiotopoulos, E.; Strzelczyk, P.; Herrmann, M.; Scuderi, G. Cadaveric study on static medial patellar stabilizers: The dynamizing role of the vastus medialis obliquus on medial patellofemoral ligament. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 7–12. [Google Scholar] [CrossRef]
- Yang, J.-H.; Eun, S.-P.; Park, D.-H.; Kwak, H.-B.; Chang, E. The Effects of Anterior Cruciate Ligament Reconstruction on Individual Quadriceps Muscle Thickness and Circulating Biomarkers. Int. J. Environ. Res. Public Health 2019, 16, 4895. [Google Scholar] [CrossRef] [Green Version]
- Powers, C.M. Patellar kinematics, part I: The influence of vastus muscle activity in subjects with and without patellofemoral pain. Phys. Ther. 2000, 80, 956–964. [Google Scholar] [CrossRef] [Green Version]
- Jan, M.-H.; Lin, D.-H.; Lin, J.-J.; Lin, C.-H.J.; Cheng, C.-K.; Lin, Y.-F. Differences in sonographic characteristics of the vastus medialis obliquus between patients with patellofemoral pain syndrome and healthy adults. Am. J. Sports Med. 2009, 37, 1743–1749. [Google Scholar] [CrossRef]
- Fulkerson, J.P. Diagnosis and treatment of patients with patellofemoral pain. Am. J. Sports Med. 2002, 30, 447–456. [Google Scholar] [CrossRef]
- Koh, E.-K.; Lee, K.-H.; Jung, D.-Y. The effect of isometric hip adduction and abduction on the muscle activities of vastus medialis oblique and vastus lateralis during leg squat exercises. Korean J. Sport Biomech. 2011, 21, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Hanten, W.P.; Schulthies, S.S. Exercise effect on electromyographic activity of the vastus medialis oblique and vastus lateralis muscles. Phys. Ther. 1990, 70, 561–565. [Google Scholar] [CrossRef] [Green Version]
- van Melick, N.; van Cingel, R.E.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [Green Version]
- RL, D.; Vogl, A. Gray’s Anatomy for Students; Churchill Livingstone/Elsevier: Philadelphia, PA, USA, 2015; pp. 592–594. [Google Scholar]
- Zhang, L.Q.; Wang, G.; Nuber, G.W.; Press, J.M.; Koh, J.L. In vivo load sharing among the quadriceps components. J. Orthop. Res. 2003, 21, 565–571. [Google Scholar] [CrossRef]
- Hooper, D.M.; Morrissey, M.C.; Drechsler, W.; Morrissey, D.; King, J. Open and closed kinetic chain exercises in the early period after anterior cruciate ligament reconstruction: Improvements in level walking, stair ascent, and stair descent. Am. J. Sports Med. 2001, 29, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Perry, M.C.; Morrissey, M.C.; King, J.B.; Morrissey, D.; Earnshaw, P. Effects of closed versus open kinetic chain knee extensor resistance training on knee laxity and leg function in patients during the 8-to 14-week post-operative period after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 357–369. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | OKCE (n = 13) | CKCE (n = 13) | p-Value |
|---|---|---|---|
| Age (years) | 23.5 ± 1.7 | 25.1 ± 5.1 | 0.30 |
| Height (cm) | 170.2 ± 6.5 | 168.4 ± 8.0 | 0.53 |
| Mass (kg) | 67.8 ± 15.6 | 65.1 ± 9.8 | 0.61 |
| BMI (kg/m2) | 23.2 ± 4.6 | 22.9 ± 2.5 | 0.82 |
| Muscles | OKCE | CKCE | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | ES | Pre | Post | ES | ||
| RF(mm) | 19.72 ± 2.98 | 20.70 ± 3.70 | 0.29 | 18.71 ± 2.47 | 18.45 ± 3.68 | −0.08 | 0.59 |
| VI(mm) | 13.92 ± 4.08 | 15.86 ± 3.13 | 0.53 | 15.30 ± 2.46 | 16.47 ± 3.66 | 0.38 | * 0.01 |
| VL(mm) | 20.39 ± 2.77 | 20.87 ± 3.46 | 0.15 | 18.68 ± 3.00 | 19.77 ± 3.36 | 0.34 | 0.20 |
| VM(mm) | 25.61 ± 3.92 | 24.58 ± 3.95 | −0.26 | 23.71 ± 4.51 | 24.83 ± 4.20 | 0.26 | 0.98 |
| VMO(mm) | 14.37 ± 3.50 | 15.42 ± 3.70 | 0.29 | 12.59 ± 2.96 | 15.72 ± 3.19 | 1.02 | * 0.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheon, S.; Lee, J.-H.; Jun, H.-P.; An, Y.W.; Chang, E. Acute Effects of Open Kinetic Chain Exercise Versus Those of Closed Kinetic Chain Exercise on Quadriceps Muscle Thickness in Healthy Adults. Int. J. Environ. Res. Public Health 2020, 17, 4669. https://doi.org/10.3390/ijerph17134669
Cheon S, Lee J-H, Jun H-P, An YW, Chang E. Acute Effects of Open Kinetic Chain Exercise Versus Those of Closed Kinetic Chain Exercise on Quadriceps Muscle Thickness in Healthy Adults. International Journal of Environmental Research and Public Health. 2020; 17(13):4669. https://doi.org/10.3390/ijerph17134669
Chicago/Turabian StyleCheon, Soul, Joo-Hyun Lee, Hyung-Pil Jun, Yong Woo An, and Eunwook Chang. 2020. "Acute Effects of Open Kinetic Chain Exercise Versus Those of Closed Kinetic Chain Exercise on Quadriceps Muscle Thickness in Healthy Adults" International Journal of Environmental Research and Public Health 17, no. 13: 4669. https://doi.org/10.3390/ijerph17134669
APA StyleCheon, S., Lee, J. -H., Jun, H. -P., An, Y. W., & Chang, E. (2020). Acute Effects of Open Kinetic Chain Exercise Versus Those of Closed Kinetic Chain Exercise on Quadriceps Muscle Thickness in Healthy Adults. International Journal of Environmental Research and Public Health, 17(13), 4669. https://doi.org/10.3390/ijerph17134669