Social Capital and Preferences for Aging in Place Among Older Adults Living in Rural Northeast China


Abstract
:1. Introduction
1.1. Social Capital and Aging in Place
1.2. Population Aging and Filial Piety in Rural China
2. Materials and Methods
2.1. Sampling
2.2. Measurements
2.2.1. Outcome Variable
2.2.2. Social Capital Variable
2.2.3. Covariates
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics
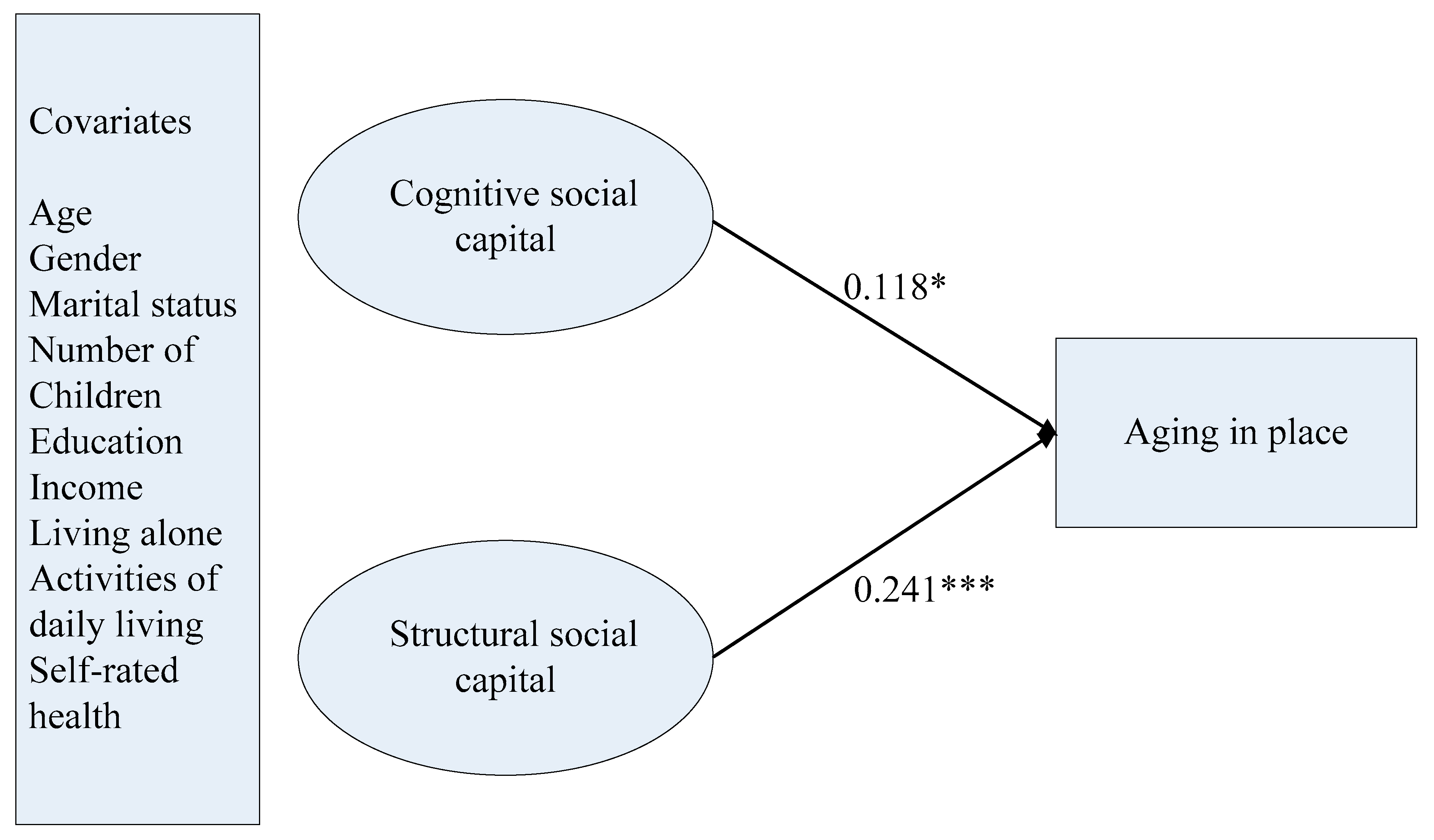
3.2. Structural Equation Modeling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E.S. The meaning of “aging in place” to older people. Gerontologist 2011, 52, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Sabia, J.J. There’s no place like home: A hazard model analysis of aging in place among older homeowners in the PSID. Res. Aging 2008, 30, 3–35. [Google Scholar] [CrossRef]
- Jiang, N.; Lou, V.W.Q.; Lu, N. Does social capital influence preferences for aging in place? Evidence from urban China. Aging Ment. Health 2018, 22, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.; Lee, Y. Social support networks and expectations for aging in place and moving. Res. Aging 2011, 33, 444–464. [Google Scholar] [CrossRef]
- Lum, T.; Lou, V.W.Q.; Chen, Y.; Wong, G.H.Y.; Luo, H.; Tong, T.L.W. Neighborhood support and aging-in-place preference among low-income elderly Chinese city-dwellers. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 71, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Chippendale, T.; Bearlehman, J. Enabling “aging in place” for urban dwelling seniors: An adaptive or remedial approach? Phys. Occup. Ther. Geriatr. 2010, 28, 57–62. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Putnam, R.D. Democracies in Flux: The Evolution of Social Capital in Contemporary Society; Oxford University Press: Oxford, UK, 2002. [Google Scholar] [CrossRef]
- Carver, L.F.; Beamish, R.; Phillips, S.P.; Villeneuve, M. A scoping review: Social participation as a cornerstone of successful aging in place among rural older adults. Geriatrics 2018, 3, 75. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.Y.; Lu, N. Community-based cognitive social capital and depressive symptoms among older adults in urban China: The moderating role of family social capital. Int. J. Aging Hum. Dev. 2019, 90, 297–316. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, N. What matters most for community social capital among older adults living in urban China: The role of health and family social capital. Int. J. Environ. Res. Public Health 2019, 16, 558. [Google Scholar] [CrossRef] [Green Version]
- Lu, N.; Zhang, J. Social capital and self-rated health among older adults living in urban China: A mediation model. Sustainability 2019, 11, 5566. [Google Scholar] [CrossRef] [Green Version]
- Lu, N.; Jiang, N.; Lou, V.W.Q.; Zeng, Y.; Liu, M. Does gender moderate the relationship between social capital and life satisfaction? Evidence from urban China. Res. Aging 2018, 40, 740–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putnam, R.D.; Leonardi, R.; Nanetti, R. Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1993. [Google Scholar]
- Bourdieu, P. The forms of capital. In Handbook of Theory and Research for the Sociology of Education; Richardson, J.G., Ed.; Greenwood Press: New York, NY, USA, 1986. [Google Scholar]
- Coleman, J.S. Social capital in the creation of human capital. Am. J. Sociol. 1988, 94, 95–120. [Google Scholar] [CrossRef]
- Coleman, J.S. Foundations of Social Theory; Harvard University Press: Cambridge, MA, USA, 1990. [Google Scholar]
- Lin, N. Building a network theory of social capital. Connections 1999, 22, 28–51. [Google Scholar]
- Nyqvist, F.; Forsman, A.K.; Giuntoli, G.; Cattan, M. Social capital as a resource for mental well-being in older people: A systematic review. Aging Ment. Health 2012, 17, 394–410. [Google Scholar] [CrossRef] [PubMed]
- De Silva, M.J.; Huttly, S.R.; Harpham, T.; Kenward, M.G. Social capital and mental health: A comparative analysis of four low income countries. Soc. Sci. Med. 2007, 64, 5–20. [Google Scholar] [CrossRef]
- Versey, H.S. A tale of two Harlems: Gentrification, social capital, and implications for aging in place. Soc. Sci. Med. 2018, 214, 1–11. [Google Scholar] [CrossRef]
- Lehning, A.J.; Smith, R.J.; Dunkle, R.E. Do age-friendly char- acteristics influence the expectation to age in place? A comparison of low-income and higher income Detroit elders. J. Appl. Gerontol. 2013, 34, 158–180. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics of China. China Statistical Yearbook–2019; China Statistics Press: Beijing, China, 2019.
- Mjelde-Mossey, L.A.; Chi, I.; Lou, V.W.Q. Relationship between adherence to tradition and depression in Chinese elders in China. Aging Ment. Health 2006, 10, 19–26. [Google Scholar] [CrossRef]
- Hu, Z.; Peng, X. Household changes in contemporary China: An analysis based on the four recent censuses. J. Chin. Sociol. 2015, 2, 9. [Google Scholar] [CrossRef]
- Ramesh, M.; Wu, X. Health policy reform in China: Lessons from Asia. Soc. Sci. Med. 2009, 68, 2256–2262. [Google Scholar] [CrossRef]
- Cai, Y.; Cheng, Y. Pension reform in China: Challenges and opportunities. J. Econ. Surv. 2014, 28, 636–651. [Google Scholar] [CrossRef]
- Hu, S.; Tang, S.; Liu, Y.; Zhao, Y.; Escobar, M.L.; de Ferranti, D. Reform of how health care is paid for in China: Challenges and opportunities. Lancet 2008, 372, 1846–1853. [Google Scholar] [CrossRef]
- Yip, W.; Hsiao, W.C. What drove the cycles of Chinese health system reforms. Health Syst. Reform 2015, 1, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, E. A Short Portable Mental Status Questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Grootaert, C.; Narayan, D.; Jones, V.N.; Woolcock, M. Integrated Questionnaire for the Measurement of Social Capital; World Bank: Washington, DC, USA, 2004. [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Muthén, L.K.; Muthén, B. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Sun, Q.; Lou, V.W.Q.; Dai, A.; To, C.; Wong, S.Y. The effectiveness of the Young-Old Link and Growth intergenerational program in reducing age stereotypes. Res. Soc. Work Pract. 2019, 29, 519–528. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | n (%) | Mean (SD) |
|---|---|---|
| Age | 69.41 (6.21) | |
| 60–69 | 270 (59.0) | |
| 70 or above | 188 (41.0) | |
| Gender | ||
| Men | 235 (51.3) | |
| Women | 223 (48.7) | |
| Married | 322 (70.3) | |
| Education | ||
| Illiterate | 169 (36.9) | |
| Primary school or above | 289 (63.1) | |
| Annual household income | ||
| Equal or less than RMB10000 | 241 (52.6) | |
| RMB10001 or above | 217 (47.4) | |
| Self-rated health | ||
| Very poor/poor/fair | 191 (41.7) | |
| Good/very good | 266 (58.1) | |
| ADL | 98.08 (6.62) | |
| Number of Children | 2.42 (1.31) | |
| Living alone | 72 (15.7) | |
| Prefer to continue to live in the community | 343 (74.9) |
| Factor Indicator | Estimate | SD | Standardized Estimate | SD |
|---|---|---|---|---|
| Cognitive social capital | ||||
| Trust in local community | 1.000 | 0.000 | 0.671 *** | 0.016 |
| Willingness to cooperate with others | 1.324 *** | 0.057 | 0.927 *** | 0.009 |
| Perceived helpfulness of others | 1.082 *** | 0.066 | 0.840 *** | 0.011 |
| Feelings of belonging | 1.265 *** | 0.052 | 0.891 *** | 0.009 |
| Structural social capital | ||||
| Organization memberships | 1.000 | 0.000 | 0.723 *** | 0.723 |
| Social participation | 2.788 *** | 0.498 | 0.915 *** | 0.915 |
| Volunteering | 0.683 *** | 0.141 | 0.390 *** | 0.390 |
| Citizenship activities | 0.839 *** | 0.119 | 0.479 *** | 0.479 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, N.; Xu, S.; Zhou, Q. Social Capital and Preferences for Aging in Place Among Older Adults Living in Rural Northeast China. Int. J. Environ. Res. Public Health 2020, 17, 5085. https://doi.org/10.3390/ijerph17145085
Lu N, Xu S, Zhou Q. Social Capital and Preferences for Aging in Place Among Older Adults Living in Rural Northeast China. International Journal of Environmental Research and Public Health. 2020; 17(14):5085. https://doi.org/10.3390/ijerph17145085
Chicago/Turabian StyleLu, Nan, Shicun Xu, and Qinghong Zhou. 2020. "Social Capital and Preferences for Aging in Place Among Older Adults Living in Rural Northeast China" International Journal of Environmental Research and Public Health 17, no. 14: 5085. https://doi.org/10.3390/ijerph17145085
APA StyleLu, N., Xu, S., & Zhou, Q. (2020). Social Capital and Preferences for Aging in Place Among Older Adults Living in Rural Northeast China. International Journal of Environmental Research and Public Health, 17(14), 5085. https://doi.org/10.3390/ijerph17145085