Is There a Link between Different Types of Alcoholic Drinks and Obesity? An Analysis of 280,183 UK Biobank Participants


 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Outcomes
2.2. Alcohol Consumption
2.3. Covariates
2.4. Statistical Analysis
- (a)
- Multiple logistic regression to investigate the associations between overall alcohol consumption and alcoholic drink types with dichotomous (BMI-defined) overweight (25 kg/m2) and obesity (30 kg/m2).
- (b)
- Additional adjustment for education as an individual-level indicator of socioeconomic status using age completed the highest education qualification.
- (c)
- Additional analysis by including 2389 participants who were underweight but had a BMI over 13 kg/m2.
- (d)
- We combined previous and never drinkers as a reference in order to compare the results with previous studies.
3. Results
3.1. Overall Alcohol Consumption, BMI and Body Fat
3.2. Individual Types of Alcohol Drinks, BMI and Body Fat
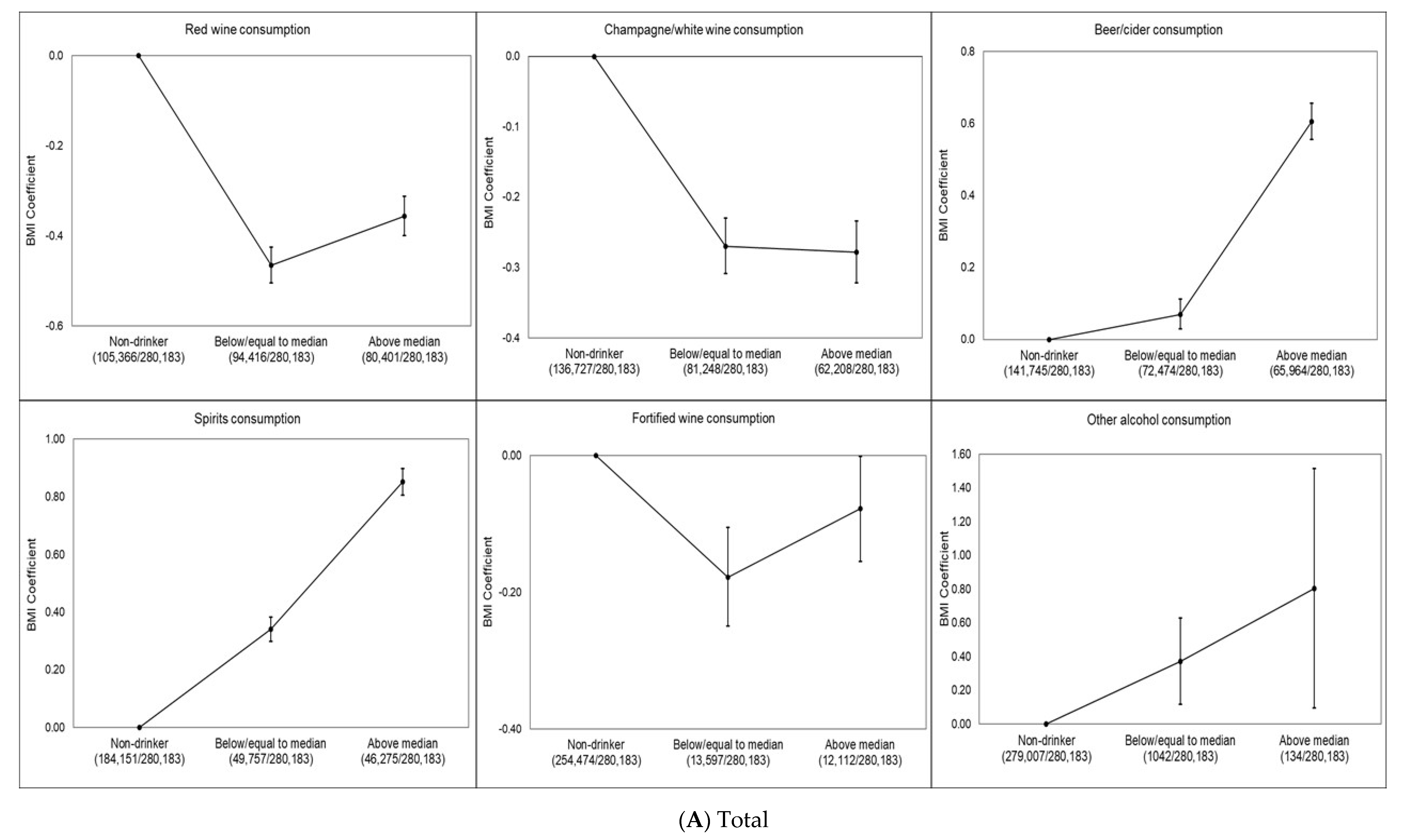
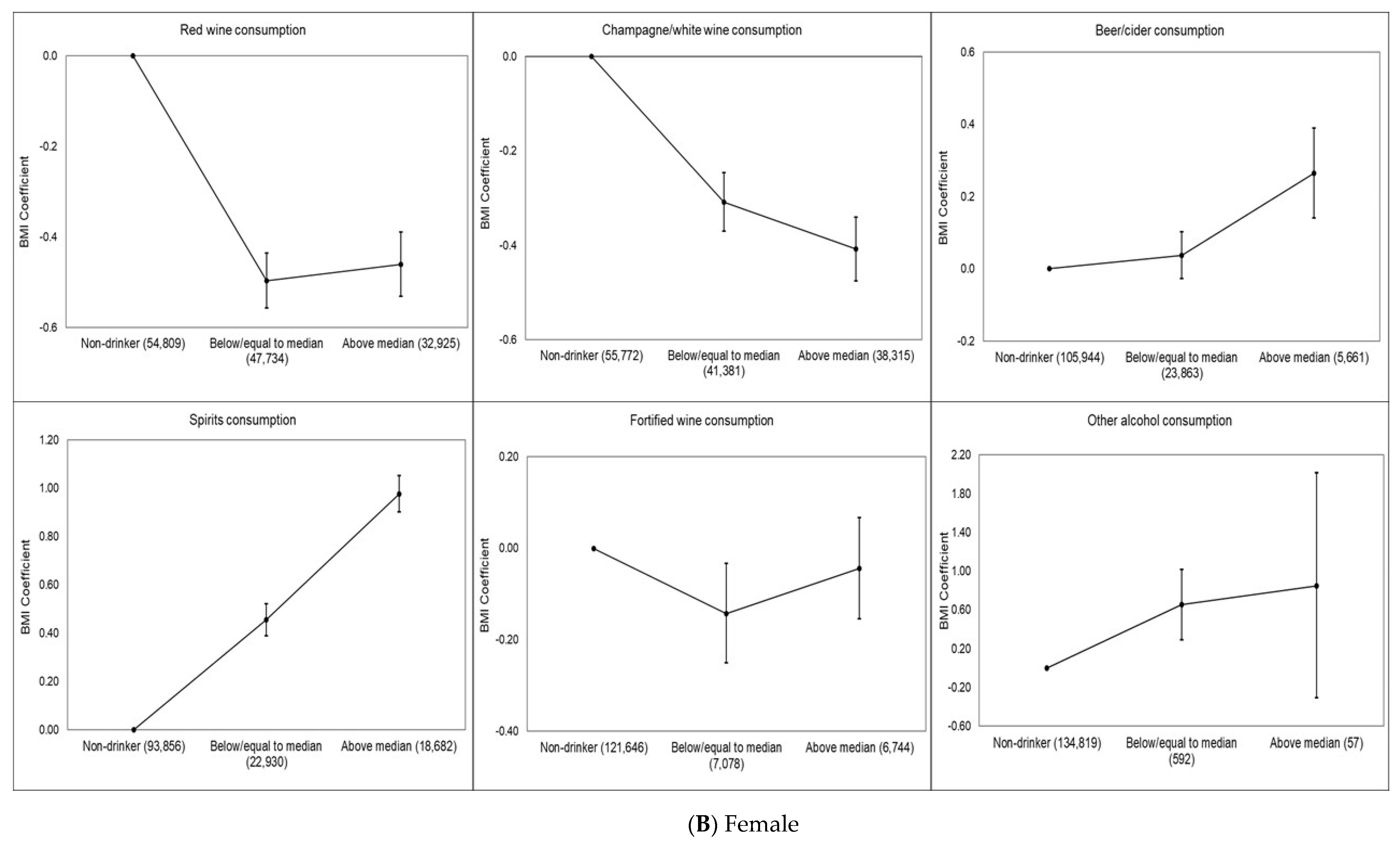
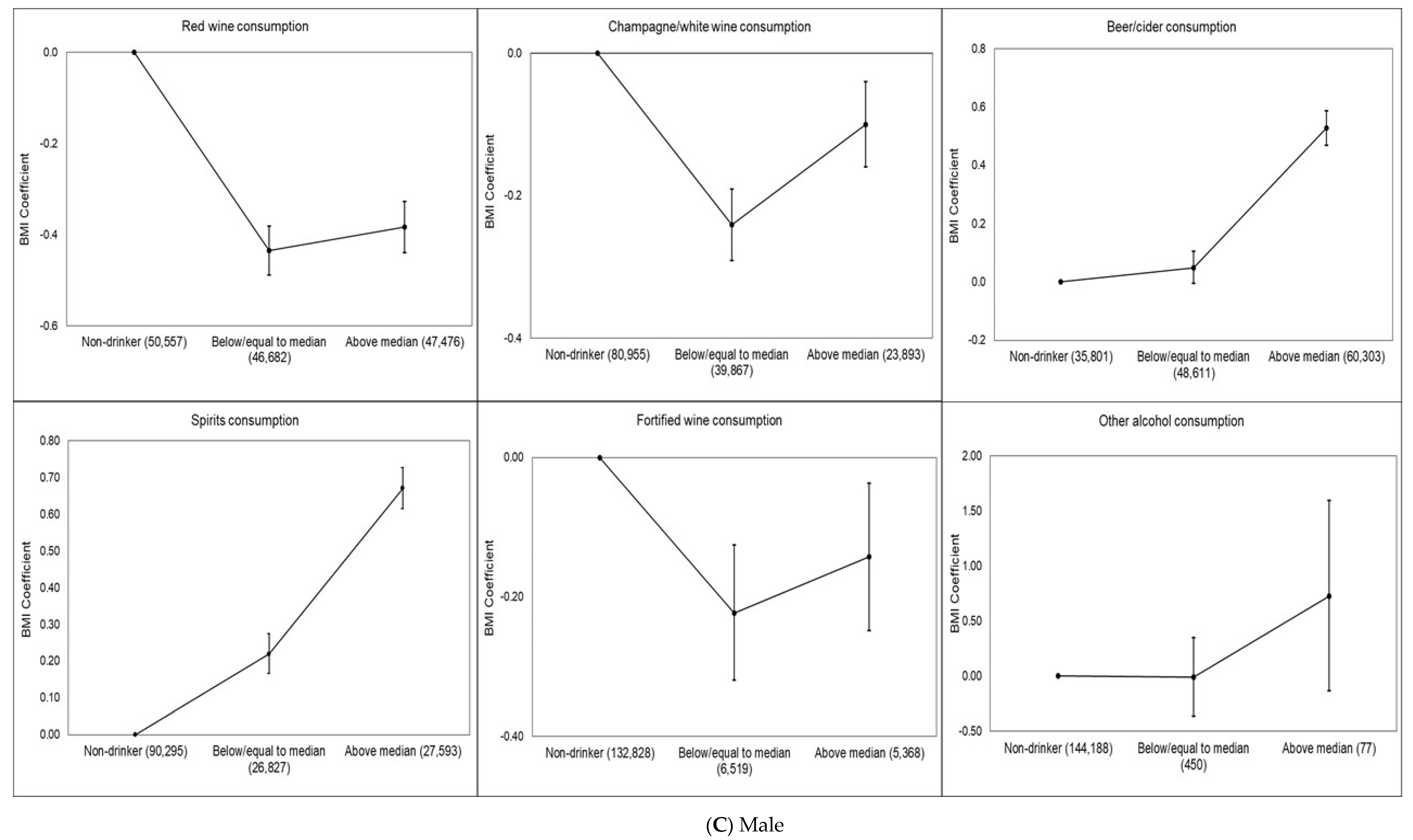
3.3. Dose–Response Associations of Specific Alcoholic Drink Types and BMI/obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Cancer Research UK. Overweright and Obesity Statistics. 2016. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/risk/overweight-and-obesity#heading-One (accessed on 5 April 2020).
- World Health Organization. Nutrition, Physical Activity and Obesity: United Kingdom of Great Britain and Northern Ireland. 2016. Available online: http://www.euro.who.int/__data/assets/pdf_file/0020/243335/United-Kingdom-WHO-Country-Profile.pdf?ua=1 (accessed on 5 April 2020).
- McPherson, K.; Marsh, T.; Brown, M. Foresight report on obesity. Lancet 2007, 370, 1755. [Google Scholar] [CrossRef]
- Yeomans, M.R. Effects of alcohol on food and energy intake in human subjects: Evidence for passive and active over-consumption of energy. Br. J. Nutr. 2004, 92, S31–S34. [Google Scholar] [CrossRef][Green Version]
- Tayie, F.A.; Beck, G.L. Alcoholic beverage consumption contributes to caloric and moisture intakes and body weight status. Nutrition 2016, 32, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Lukasiewicz, E.; Mennen, L.I.; Bertrais, S.; Arnault, N.; Preziosi, P.; Galan, P.; Hercberg, S. Alcohol intake in relation to body mass index and waist-to-hip ratio: The importance of type of alcoholic beverage. Public Health Nutr. 2005, 8, 315–320. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Sharper, A.G.; Whincup, P.H. Alcohol and adiposity: Effects of quantity and type of drink and time relation with meals. Int. J. Obes. 2005, 29, 1436–1444. [Google Scholar] [CrossRef]
- Arif, A.A.; Rohrer, J.E. Patterns of alcohol drinking and its association with obesity: Data from the Third National Health and Nutrition Examination Survey, 1988–1994. BMC Public Health 2005, 5, 126. [Google Scholar] [CrossRef]
- Butler, L.; Popkin, B.M.; Poti, J.M. Associations of Alcoholic Beverage Consumption with Dietary Intake, Waist Circumference, and Body Mass Index in US Adults: National Health and Nutrition Examination Survey 2003–2012. J. Acad. Nutr. Diet. 2018, 118, 409–420. [Google Scholar] [CrossRef]
- Wang, L.; Lee, I.M.; Manson, J.E.; Buring, J.E.; Sesso, H.D. Alcohol consumption, weight gain, and risk of becoming overweight in middle-aged and older women. Arch. Intern. Med. 2010, 170, 453–461. [Google Scholar] [CrossRef]
- Breslow, R.A.; Smothers, B.A. Drinking Patterns and Body Mass Index in Never Smokers National Health Interview Survey, 1997–2001. Am. J. Epidemiol. 2005, 161, 368–376. [Google Scholar] [CrossRef]
- Fillmore, K.M.; Stockwell, T.; Chikritzhs, T.; Bostrom, A.; Kerr, W. Moderate alcohol use and reduced mortality risk: Systematic error in prospective studies and new hypotheses. Ann. Epidemiol. 2007, 17, S16–S23. [Google Scholar] [CrossRef]
- Poli, A.; Marangoni, F.; Avogaro, A.; Barba, G.; Bellentani, S.; Bucci, M.; Cambieri, R.; Catapano, A.L.; Costanzo, S.; Cricelli, C.; et al. Moderate alcohol use and health: A consensus document. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 487–504. [Google Scholar] [CrossRef] [PubMed]
- Traversy, G.; Chaput, J.P. Alcohol consumption and obesity: An update. Curr. Obes. Rep. 2015, 4, 122–130. [Google Scholar] [CrossRef]
- Sayon-Orea, C.; Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Alcohol consumption and body weight: A systematic review. Nutr. Rev. 2011, 69, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, M.R. Alcohol, appetite and energy balance: Is alcohol intake a risk factor for obesity? Physiol. Behav. 2010, 100, 82–89. [Google Scholar] [CrossRef]
- Sayon-Orea, C.; Bes-Rastrollo, M.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Buenza, J.J.; Martinez-Gonzalez, M.A. Type of alcoholic beverage and incidence of overweight/obesity in a Mediterranean cohort: The SUN project. Nutrition 2011, 27, 802–808. [Google Scholar] [CrossRef]
- Dumesnil, C.; Dauchet, L.; Ruidavets, J.B.; Bingham, A.; Arveiler, D.; Ferrieres, J.; Ducimetiere, P.; Haas, B.; Bongard, V.; Wagner, A.; et al. Alcohol consumption patterns and body weight. Ann. Nutr. Metab. 2013, 62, 91–97. [Google Scholar] [CrossRef]
- MacInnis, R.J.; Hodge, A.M.; Dixon, H.G.; Peeters, A.; Johnson, L.E.; English, D.R.; Giles, G.G. Predictors of increased body weight and waist circumference for middle-aged adults. Public Health Nutr. 2014, 17, 1087–1097. [Google Scholar] [CrossRef]
- Kwok, A.; Dordevic, A.L.; Paton, G.; Page, M.J.; Truby, H. Effect of alcohol consumption on food energy intake: A systematic review and meta-analysis. Br. J. Nutr. 2019, 121, 481–495. [Google Scholar] [CrossRef]
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- Baliunas, D.O.; Taylor, B.J.; Irving, H.; Roerecke, M.; Patra, J.; Mohapatra, S.; Rehm, J. Alcohol as a risk factor for type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2009, 32, 2123–2132. [Google Scholar] [CrossRef]
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 2011, 342, d671. [Google Scholar] [CrossRef] [PubMed]
- Boffetta, P.; Hashibe, M. Alcohol and cancer. Lancet Oncol. 2006, 7, 149–156. [Google Scholar] [CrossRef]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed]
- UK Biobank: Protocol for a Large-Scale Prospective Epidemiological Resource. 2007. Available online: https://www.ukbiobank.ac.uk/wp-content/uploads/2011/11/UK-Biobank-Protocol.pdf (accessed on 5 April 2020).
- Vasold, K.L.; Parks, A.C.; Phelan, D.M.; Pontifex, M.B.; Pivarnik, J.M. Reliability and Validity of Commercially Available Low-Cost Bioelectrical Impedance Analysis. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 406–410. [Google Scholar] [CrossRef]
- Alcohol Guidelines Review—Report from the Guidelines Development Group to the UK Chief Medical Officers; Department of Health: London, UK, 2016.
- Perreault, K.; Bauman, A.; Johnson, N.; Britton, A.; Rangul, V.; Stamatakis, E. Does physical activity moderate the association between alcohol drinking and all-cause, cancer and cardiovascular diseases mortality? A pooled analysis of eight British population cohorts. Br. J. Sports Med. 2017, 51, 651–657. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and the North; Croom Helm: London, UK, 1988. [Google Scholar]
- McCarty, M.F. The insulin-sensitising activity of moderate alcohol consumption may promote leanness in women. Med. Hypotheses 2000, 54, 794–797. [Google Scholar] [CrossRef]
- Foster, R.K.; Marriott, H.E. Alcohol consumption in the new millennium—Weighing up the risks and benefits for our health. Nutr. Bull. 2006, 31, 286–331. [Google Scholar] [CrossRef]
- Teschke, R. Microsomal Ethanol-Oxidizing System: Success Over 50 Years and an Encouraging Future. Alcohol Clin. Exp. Res. 2019, 43, 386–400. [Google Scholar] [CrossRef]
- Newton, J.N.; Briggs, A.D.; Murray, C.J.; Dicker, D.; Foreman, K.J.; Wang, H.; Naghavi, M.; Forouzanfar, M.H.; Ohno, S.L.; Barber, R.M.; et al. Changes in health in England, with analysis by English regions and areas of deprivation, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2257–2274. [Google Scholar] [CrossRef]
- Public Health England. Social and Economic Inequalities in Diet and Physical Activity. 2013. Available online: https://webarchive.nationalarchives.gov.uk/20170110165944/https://www.noo.org.uk/NOO_pub/briefing_papers (accessed on 5 April 2020).
- The Public Health Burden of Alcohol and the Effectiveness and Cost-Effectiveness of Alcohol Control Policies: An Evidence Review; Public Health England: London, UK, 2016.
- Scottish Health Survey 2018: Volume One—Main Report; Chapter 3—Alcohol; Scottish Government: Edinburgh, UK, 2019.
- Office for National Statistics. Adult Drinking Habits in Great Britain. 2017. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/drugusealcoholandsmoking/bulletins/opinionsandlifestylesurveyadultdrinkinghabitsingreatbritain/2017 (accessed on 10 July 2020).
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Powell, L.; Vassallo, A.J.; Hamer, M.; Stamatakis, E. Does adequate physical activity attenuate the associations of alcohol and alcohol-related cancer mortality? A pooled study of 54,686 British adults. Cancer Epidemiol. 2020. [Google Scholar] [CrossRef]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Guo, W.; Cairns, B.J.; Armstrong, M.E.; Key, T.J. Association between physical activity and body fat percentage, with adjustment for BMI: A large cross-sectional analysis of UK Biobank. BMJ Open 2017, 7, e011843. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Ma, F.; Lou, H.; Liu, Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health 2013, 13, 629. [Google Scholar] [CrossRef]
- Colditz, G.A.; Giovannucci, E.; Rimm, E.B.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Gordis, E.; Willett, W.C. Alcohol in relation to diet and obesity in women and men. Am. J. Clin. Nutr. 1991, 54, 49–55. [Google Scholar] [CrossRef]
- Vadstrup, E.S.; Petersen, L.; Sørensen, T.I.A.; Grønbaek, M. Waist circumference in relation to history of amount and type of alcohol: Results from the Copenhagen City Heart Study. Int. J. Obes. 2003, 27, 238–246. [Google Scholar] [CrossRef]
- Shelton, N.J.; Knott, C.S. Association between alcohol calorie intake and overweight and obesity in English adults. Am. J. Public Health 2014, 104, 629–631. [Google Scholar] [CrossRef]
- Ruidavets, J.B.; Bataille, V.; Dallongeville, J.; Simon, C.; Bingham, A.; Amouyel, P.; Arveiler, D.; Ducimetière, P.; Ferrières, J. Alcohol intake and diet in France, the prominent role of lifestyle. Eur. Heart J. 2004, 25, 1153–1162. [Google Scholar] [CrossRef]
- Mortensen, E.L.; Jensen, H.H.; Sanders, S.A.; Reinisch, J.M. Better psychological functioning and higher social status may largely explain the apparent health benefits of wine: A study of wine and beer drinking in young Danish adults. Arch. Intern. Med. 2001, 161, 1844–1848. [Google Scholar] [CrossRef]
- Fischer-Posovszky, P.; Kukulus, V.; Tews, D.; Unterkircher, T.; Debatin, K.M.; Fulda, S.; Wabitsch, M. Resveratrol regulates human adipocyte number and function in a Sirt1-dependent manner. Am. J. Clin. Nutr. 2010, 92, 5–15. [Google Scholar] [CrossRef]
- Beulens, J.W.; van Beers, R.M.; Stolk, R.P.; Schaafsma, G.; Hendriks, H.F. The effect of moderate alcohol consumption on fat distribution and adipocytokines. Obesity 2006, 14, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Suter, P.M.; Häsler, E.; Vetter, W. Effects of alcohol on energy metabolism and body weight regulation: Is alcohol a risk factor for obesity? Nutr. Rev. 1997, 55, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Männistö, S.; Uusitalo, K.; Roos, E.; Fogelholm, M.; Pietinen, P. Alcohol beverage drinking, diet and body mass index in a cross-sectional survey. Eur. J. Clin. Nutr. 1997, 51, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Batty, G.D.; Shipley, M.; Tabák, A.; Singh-Manoux, A.; Brunner, E.; Britton, A.; Kivimäki, M. Generalizability of occupational cohort study findings. Epidemiology 2014, 25, 932–933. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Alcohol Consumption Categories | |||||
|---|---|---|---|---|---|
| Characteristic | Never Drinker (n = 13,143) | Previous Drinker (n = 11,676) | Within Guidelines (n = 175,812) | Hazardous (n = 75,626) | Harmful (n = 3926) |
| Alcohol consumption (number of UK units/week) 1 | N/A | N/A | 6.8 (3.2) | 21.4 (7.3) | 57.0 (22.8) |
| Red wine (percent who reported any consumption in the previous week) | N/A | N/A | 65.9 | 74.4 | 67.3 |
| Champagne/white wine (percent who reported any consumption in the previous week) | N/A | N/A | 55.2 | 58.2 | 60.4 |
| Beer/cider (percent who reported any consumption in the previous week) | N/A | N/A | 48.5 | 67.3 | 60.2 |
| Spirits (percent who reported any consumption in the previous week) | N/A | N/A | 32.2 | 49.0 | 61.8 |
| Fortified wine (percent who reported any consumption in the previous week) | N/A | N/A | 9.7 | 10.8 | 11.5 |
| Other alcohol (percent who reported any consumption in the previous week) | N/A | N/A | 0.5 | 0.4 | 0.7 |
| Physical activity2 | |||||
| Not meeting guidelines (%) | 21.2 | 21.1 | 16.8 | 16.8 | 23.0 |
| Meeting lower guidelines (%) | 17.8 | 16.3 | 18.1 | 17.0 | 17.0 |
| Meeting upper guidelines (%) | 60.9 | 62.5 | 65.1 | 66.2 | 59.9 |
| Age (years) | 56.8 (8.6) | 56.8 (8.0) | 56.2 (8.1) | 56.5 (7.9) | 55.6 (7.8) |
| Female (%) | 69.3 | 52.7 | 54.7 | 29.7 | 40.3 |
| Body mass index (BMI, kg/m2) 3 | 27.9 (5.4) | 28.1 (5.4) | 26.7 (4.3) | 27.5 (4.1) | 28.1 (4.7) |
| Body mass index (BMI, kg/m2) 3 categories | |||||
| Normal (%) | 31.5 | 30.6 | 37.3 | 27.7 | 25.7 |
| Overweight (%) | 39.5 | 39.4 | 43.5 | 48.6 | 43.0 |
| Obese (%) | 29.0 | 30.0 | 19.2 | 23.8 | 31.3 |
| Body fat percentage (BF%) | 31.4 (8.5) | 31.5 (8.6) | 31.4 (8.5) | 31.4 (8.5) | 31.6 (8.5) |
| Sleep duration (h) | 7.1 (1.3) | 7.2 (1.4) | 7.2 (1.0) | 7.2 (1.0) | 7.2 (1.3) |
| Cigarette smoking | |||||
| Never (%) | 82.5 | 45.1 | 58.5 | 38.5 | 24.4 |
| Previous (%) | 11.9 | 40.6 | 34.3 | 46.7 | 44.8 |
| Current (%) | 5.5 | 14.3 | 7.2 | 14.8 | 30.7 |
| Sedentary behavior (hours/day) | 4.7 (2.7) | 5.1 (2.8) | 4.6 (2.3) | 5.0 (2.4) | 5.4 (2.9) |
| Townsend deprivation index 4 | −0.5 (3.4) | −0.2 (3.5) | −1.8 (2.8) | −1.5 (2.9) | −0.6 (3.3) |
| Fruit and vegetable consumption (average number of servings/day) | 9.0 (6.2) | 8.7 (5.7) | 8.1 (4.4) | 7.6 (4.4) | 7.0 (5.1) |
| Chronic Illness | |||||
| Major CVD event (%) | 3.6 | 3.6 | 3.6 | 3.7 | 3.3 |
| Cancer (%) | 8.4 | 8.3 | 8.0 | 8.0 | 7.5 |
| Education 5 | 16.3 (4.5) | 16.3 (3.2) | 16.8 (2.8) | 16.8 (2.7) | 16.7 (2.9) |
| Employment Status (%) | |||||
| In paid employment/self-employed | 56.9 | 57.1 | 57.3 | 57.4 | 57.5 |
| Unemployed | 1.7 | 1.5 | 1.6 | 1.7 | 1.8 |
| Retired | 33.2 | 33.9 | 33.3 | 33.3 | 32.7 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| Coefficient (95% CI) | p | Coefficient (95%CI) | p | |
| Alcohol consumption | ||||
| BMI | ||||
| Never drinker | Referent | <0.001 | Referent | <0.001 |
| Previous drinker | −0.01 (−0.12, 0.10) | −0.11 (−0.22, −0.01) | ||
| Within guidelines | −1.34 (−1.42, −1.26) | −1.12 (−1.20, −1.05) | ||
| Hazardous | −0.85 (−0.93, −0.77) | −0.71 (−0.79, −0.63) | ||
| Harmful | −0.09 (−0.24, 0.07) | −0.28 (−0.43, −0.13) | ||
| Body fat percentage | ||||
| Never drinker | Referent | 0.63 | Referent | 0.55 |
| Previous drinker | 0.16 (−0.05, 0.37) | 0.16 (−0.05, 0.38) | ||
| Within guidelines | 0.06 (−0.09, 0.21) | 0.07 (−0.08, 0.23) | ||
| Hazardous | 0.06 (−0.10, 0.22) | 0.08 (−0.09, 0.24) | ||
| Harmful | 0.21 (−0.09, 0.52) | 0.23 (−0.08, 0.54) | ||
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| Coefficient (95% CI) | p | Coefficient (95% CI) | p | |
| Alcohol consumption (ref: not drinking this drink type) | ||||
| Total | ||||
| BMI | ||||
| Red wine | −0.75 (−0.78, −0.72) | <0.001 | −0.53 (−0.57, −0.50) | <0.001 |
| Champagne/white wine | −0.48 (−0.52, −0.45) | <0.001 | −0.38 (−0.41, −0.35) | <0.001 |
| Beer/cider | 0.18 (0.14, 0.22) | <0.001 | 0.20 (0.16, 0.24) | <0.001 |
| Spirits | 0.64 (0.61, 0.68) | <0.001 | 0.54 (0.51, 0.58) | <0.001 |
| Fortified wine | −0.24 (−0.29, −0.18) | <0.001 | −0.18 (−0.23, −0.12) | <0.001 |
| Other alcohol | 0.56 (0.31, 0.81) | <0.001 | 0.28 (0.04, 0.52) | 0.02 |
| Body fat percentage | ||||
| Red wine | 0.03 (−0.04, 0.10) | 0.37 | 0.03 (−0.04, 0.10) | 0.42 |
| Champagne/white wine | −0.06 (−0.13, 0.01) | 0.08 | −0.07(−0.14, 0.001) | 0.05 |
| Beer/cider | −0.03 (−0.11, 0.04) | 0.41 | −0.04 (−0.12, 0.04) | 0.29 |
| Spirits | 0.02 (−0.05, 0.09) | 0.61 | 0.02 (−0.06, 0.09) | 0.67 |
| Fortified wine | 0.01 (−0.10, 0.13) | 0.82 | 0.02 (−0.10, 0.13) | 0.79 |
| Other alcohol | 0.23 (−0.27, 0.72) | 0.37 | 0.23 (−0.27, 0.72) | 0.37 |
| Females | ||||
| BMI | ||||
| Red wine | −0.88 (−0.93, −0.83) | <0.001 | −0.52 (−0.58, −0.47) | <0.001 |
| Champagne/white wine | −0.69 (−0.74, −0.64) | <0.001 | −0.41 (−0.47, −0.36) | <0.001 |
| Beer/cider | 0.03 (−0.03, 0.09) | 0.32 | 0.06 (0.002, 0.12) | 0.04 |
| Spirits | 0.71 (0.65, 0.76) | <0.001 | 0.68 (0.63, 0.73) | <0.001 |
| Fortified wine | −0.24 (−0.33, −0.16) | <0.001 | −0.12 (−0.20, −0.04) | 0.01 |
| Other alcohol | 0.73 (0.37, 1.09) | <0.001 | 0.49 (0.15, 0.84) | 0.01 |
| Body fat percentage | ||||
| Red wine | 0.01 (−0.08, 0.11) | 0.78 | 0.02 (−0.09, 0.12) | 0.76 |
| Champagne/white wine | −0.02 (−0.11, 0.08) | 0.75 | −0.02 (−0.12, 0.09) | 0.77 |
| Beer/cider | −0.05 (−0.16, 0.07) | 0.41 | −0.05 (−0.16, 0.06) | 0.39 |
| Spirits | −0.01 (−0.11, 0.09) | 0.84 | 0.003 (−0.10, 0.11) | 0.95 |
| Fortified wine | 0.04 (−0.12, 0.19) | 0.66 | 0.04 (−0.12, 0.19) | 0.65 |
| Other alcohol | −0.07 (−0.73, 0.60) | 0.85 | −0.04 (−0.70, 0.63) | 0.91 |
| Males | ||||
| BMI | ||||
| Red wine | −0.64 (−0.68, −0.59) | <0.001 | −0.55 (−0.60, −0.51) | <0.001 |
| Champagne/white wine | −0.30 (−0.35, −0.26) | <0.001 | −0.28 (−0.32, −0.23) | <0.001 |
| Beer/cider | 0.32 (0.27, 0.37) | <0.001 | 0.19 (0.14, 0.24) | <0.001 |
| Spirits | 0.57 (0.53, 0.62) | <0.001 | 0.40 (0.36, 0.44) | <0.001 |
| Fortified wine | −0.26 (−0.34, −0.19) | <0.001 | −0.24 (−0.31, −0.16) | <0.001 |
| Other alcohol | 0.32 (−0.02, 0.66) | 0.07 | 0.03 (−0.31, 0.36) | 0.88 |
| Body fat percentage | ||||
| Red wine | 0.06 (−0.04, 0.16) | 0.25 | 0.06 (−0.04, 0.16) | 0.26 |
| Champagne/white wine | −0.11 (−0.20, −0.02) | 0.02 | −0.11 (−0.21, −0.02) | 0.02 |
| Beer/cider | −0.02 (−0.12, 0.08) | 0.71 | −0.04 (−0.15, 0.07) | 0.47 |
| Spirits | 0.04 (−0.05, 0.14) | 0.37 | 0.03 (−0.07, 0.13) | 0.53 |
| Fortified wine | −0.01 (−0.17, 0.15) | 0.91 | −0.01 (−0.17, 0.16) | 0.94 |
| Other alcohol | 0.59 (−0.15, 1.33) | 0.12 | 0.57 (−0.16, 1.31) | 0.13 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inan-Eroglu, E.; Powell, L.; Hamer, M.; O'Donovan, G.; Duncan, M.J.; Stamatakis, E. Is There a Link between Different Types of Alcoholic Drinks and Obesity? An Analysis of 280,183 UK Biobank Participants. Int. J. Environ. Res. Public Health 2020, 17, 5178. https://doi.org/10.3390/ijerph17145178
Inan-Eroglu E, Powell L, Hamer M, O'Donovan G, Duncan MJ, Stamatakis E. Is There a Link between Different Types of Alcoholic Drinks and Obesity? An Analysis of 280,183 UK Biobank Participants. International Journal of Environmental Research and Public Health. 2020; 17(14):5178. https://doi.org/10.3390/ijerph17145178
Chicago/Turabian StyleInan-Eroglu, Elif, Lauren Powell, Mark Hamer, Gary O'Donovan, Mitch J. Duncan, and Emmanuel Stamatakis. 2020. "Is There a Link between Different Types of Alcoholic Drinks and Obesity? An Analysis of 280,183 UK Biobank Participants" International Journal of Environmental Research and Public Health 17, no. 14: 5178. https://doi.org/10.3390/ijerph17145178
APA StyleInan-Eroglu, E., Powell, L., Hamer, M., O'Donovan, G., Duncan, M. J., & Stamatakis, E. (2020). Is There a Link between Different Types of Alcoholic Drinks and Obesity? An Analysis of 280,183 UK Biobank Participants. International Journal of Environmental Research and Public Health, 17(14), 5178. https://doi.org/10.3390/ijerph17145178