Prices, Availability and Affordability of Medicines with Value-Added Tax Exemption: A Cross-Sectional Survey in the Philippines

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Study Setting and Sampling
2.2. Medicines Selection
2.3. Data Collection and Entry
2.4. Data Analysis
2.5. Ethical Approval and Consent to Participate
3. Results
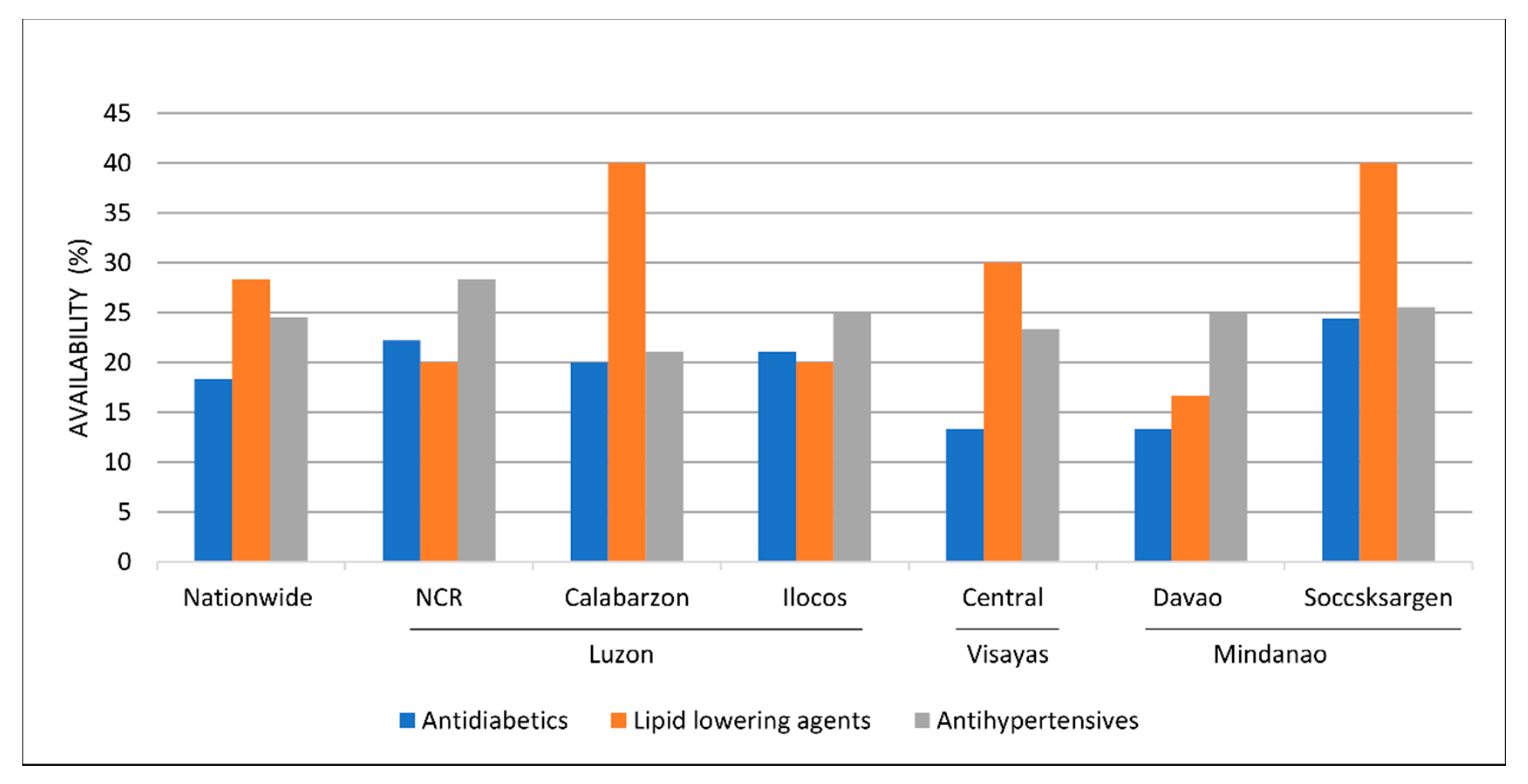
3.1. Availability
3.2. Prices
3.3. Affordability
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Island Group | Region | Population (million) | GRDP Per Capita ($) | Surveyed Public Outlets | Surveyed Private Outlets |
|---|---|---|---|---|---|
| Luzon (n = 3) | National Capital Region | 13.05 (12.2%) | 9579.73 | 6 | 7 |
| Calabarzon Region | 14.92 (14.0%) | 3295.13 | 6 | 7 | |
| Ilocos Region | 5.33 (5.0%) | 1966.23 | 6 | 7 | |
| Visayas (n = 1) | Central Visayas Region | 7.81 (7.3%) | 2831.52 | 6 | 7 |
| Mindanao (n = 2) | Davao Region | 5.25 (4.9%) | 2976.67 | 6 | 7 |
| Soccsksargen Region | 4.87 (4.6%) | 1855.60 | 6 | 7 | |
| TOTAL | 36 | 42 |
| Availability | Public Sector | Private Sector | ||
|---|---|---|---|---|
| Originator Brand | Lowest-Priced Generic | Originator Brand | Lowest-Priced Generic | |
| Medicines not found in any outlets (0%) | all excluding the eight medicines listed below (n = 37) | acarbose, candesartan, dapagliflozin, empagliflozin, enalapril + HCTZ, glimepiride, hydralazine, hydrochlorothiazide, indapamide, linagliptin, lisinopril, pioglitazone, pravastatin, sitagliptin, telmisartan + HCTZ, valsartan + HCTZ, verapamil (n = 17) | carvedilol (n = 1) | dapagliflozin, empagliflozin, hydralazine, linagliptin, sitagliptin (n = 5) |
| Medicines with very low availability (<30%) | clonidine, dapagliflozin, insulin glargine, insulin human regular, methyldopa, spironolactone, telmisartan, telmisartan + HCTZ (n = 8) | atenolol, bisoprolol, enalapril, felodipine, fenofibrate, glibenclamide, glipizide, insulin glargine, irbesartan + HCTZ, nifedipine, nimodipine, rosuvastatin, spironolactone, telmisartan, valsartan (n = 15) | acarbose, atenolol, candesartan, captopril, enalapril, enalapril + HCTZ, fenofibrate, glibenclamide, glipizide, indapamide, insulin glargine, insulin human mixed, lisinopril, losartan + HCTZ, nifedipine, nimodipine, pioglitazone, simvastatin (n = 18) | acarbose, bisoprolol, enalapril + HCTZ, glipizide, hydrochlorothiazide, indapamide, insulin glargine, insulin human isophane, insulin human mixed, insulin human regular, irbesartan + HCTZ, lisinopril, methyldopa, nifedipine, nimodipine, pravastatin, spironolactone, telmisartan, telmisartan + HCTZ, valsartan + HCTZ, verapamil (n = 21) |
| Medicines with low availability (30–49%) | None | atorvastatin, carvedilol, insulin human isophane, insulin human mixed, insulin human regular, irbesartan, losartan + HCTZ, propranolol (n = 8) | bisoprolol, dapagliflozin, empagliflozin, felodipine, gliclazide, insulin human isophane, insulin human regular, irbesartan + HCTZ, losartan, metformin, propranolol, rosuvastatin, sitagliptin, valsartan, valsartan + HCTZ, verapamil (n = 16) | candesartan, felodipine, fenofibrate, glibenclamide, pioglitazone, propranolol, valsartan (n = 7) |
| Medicines with fairly high availability (50–80%) | None | captopril, clonidine, furosemide, gliclazide, methyldopa, metoprolol, simvastatin (n = 7) | amlodipine, atorvastatin, clonidine, furosemide, irbesartan, linagliptin, methyldopa, spironolactone, telmisartan, telmisartan + HCTZ (n = 12) | atenolol, carvedilol, clonidine, enalapril, furosemide, gliclazide, glimepiride, irbesartan, losartan + HCTZ, metoprolol, rosuvastatin (n = 11) |
| Medicines with high availability (>80%) | None | amlodipine, losartan, metformin (n = 3) | None | amlodipine, atorvastatin, captopril, losartan, metformin, simvastatin (n = 6) |
| Medicine Name | Brand Name | Dosage Strength | Price in MDRP/ GMAP (PHP) | Median Unit Price 2019 (PHP) |
|---|---|---|---|---|
| amlodipine * | Norvasc | 5 mg | 22.85 | 21.86 |
| atorvastatin * | Lipitor | 20 mg | 39.13 | 38.25 |
| gliclazide | Diamicron | 80 mg | 9.75 | 9.65 |
| irbesartan | Aprovel | 150 mg | 24.38 | 24.25 |
| irbesartan + HCTZ | Coaprovel | 150 mg + 12.5 mg | 25.13 | 31.50 |
| losartan | Cozaar | 50 mg | 21.50 | 19.35 |
| losartan + HCTZ | Hyzaar | 50 mg + 12.5 mg | 23.75 | 22.63 |
| telmisartan | Micardis | 40 mg | 25.75 | 25.00 |
| telmisartan + HCTZ | Micardis Plus | 40 mg + 12.5 mg | 25.00 | 24.85 |
| Medicines | Public | Private | ||||
|---|---|---|---|---|---|---|
| LPGs | LPGs | OBs | ||||
| 2009 | 2019 | 2009 | 2019 | 2009 | 2019 | |
| Antihypertensives | ||||||
| captopril | 1.1 | 0.5 | 1.9 | 0.6 | 7.5 | - |
| Antidiabetics | ||||||
| glibenclamide | 0.4 | 0.5 | 1.1 | 1.3 | 2.4 | 0.7 |
| metformin | 1.0 | 0.2 | 1.4 | 0.5 | 3.6 | 2.3 |
| Lipid-lowering Agent | ||||||
| simvastatin | 1.3 | 0.4 | 2.1 | 0.8 | 3.4 | 2.8 |
References
- World Health Organization. Intercountry Consultation on Improving Access to Essential Medicines, Diagnostics and Medical Devices for the Management of Noncommunicable Diseases. Available online: https://iris.wpro.who.int/handle/10665.1/9593 (accessed on 12 December 2019).
- Nugent, R.; Bertram, M.Y.; Jan, S.; Niessen, L.W.; Sassi, F.; Jamison, D.T.; Pier, E.G.; Beaglehole, R. Investing in non-communicable disease prevention and management to advance the Sustainable Development Goals. Lancet 2018, 391, 2029–2035. [Google Scholar] [CrossRef]
- United Nations. Transforming Our World: The 2030 Agenda fo Sustainable Development. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld/publication (accessed on 18 February 2020).
- Beran, D.; Pedersen, H.B.; Robertson, J. Noncommunicable diseases, access to essential medicines and universal health coverage. Glob. Health Action 2019, 12, 1670014. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases Country Profiles 2018. Available online: https://www.who.int/publications/i/item/9789241514620 (accessed on 9 December 2019).
- Institute for Health Metrics and Evaluation. Top 10 Causes of Death in 2017 and Percent Change, 2007–2017, in the Philippines. Available online: http://www.healthdata.org/philippines (accessed on 18 October 2019).
- Batangan, D.; Juban, N. Philippines Pharmaceutical Situation 2009 WHO Health Facility Survey on Medicines. Available online: https://www.researchgate.net/publication/268043176_Philippines_Pharmaceutical_Situation_2009_WHO_Household_Survey_on_Medicines (accessed on 18 June 2019).
- Philippines Official Gazette. Republic Act No. 6675: Generics Act of 1988. Available online: https://www.officialgazette.gov.ph/1988/09/13/republic-act-no-6675/ (accessed on 25 November 2019).
- Philippines Official Gazette. Republic Act No. 9502: Universally Accessible Cheaper and Quality Medicines Act of 2008. Available online: https://www.officialgazette.gov.ph/2008/06/06/republic-act-no-9502/ (accessed on 25 November 2019).
- Access to Medicines in the Philippines: Overcoming the Barriers. Available online: https://think-asia.org/handle/11540/7967 (accessed on 6 July 2020).
- Ulep, V.G.; Dela Cruz, N.A. Analysis of Out-of-Pocket Expenditures in the Philippines. Philipp. J. Dev. 2013, 40, 93–123. [Google Scholar]
- Philippine Statistics Authority. Total Health Expenditures Grew by 10.5 Percent in 2016. Available online: https://psa.gov.ph/pnha-press-release/node/128109 (accessed on 18 February 2020).
- Philippine Statistics Authority. Total Health Expenditures Grew by 8.0 Percent in 2017. Available online: https://psa.gov.ph/pnha-press-release/node/136135 (accessed on 18 February 2020).
- Philippine Institute for Development Studies. High Cost of Medicines in Philippines. Available online: https://www.pids.gov.ph/pids-in-the-news/2487 (accessed on 20 November 2019).
- Creese, A. WHO/HAI Project on Medicine Prices and Availablity Review Series on Pharmaceutical Pricing Policies and Intervention Working Paper 5: Sales Taxes on Medicines. Available online: https://haiweb.org/wp-content/uploads/2015/08/Taxes-final-May2011a1.pdf (accessed on 16 November 2019).
- Bangalee, V.; Suleman, F. Cost-savings accruable to removing value added tax from antiretrovirals in the South African private health sector. Health SA Gesondheid 2017, 22, 150–156. [Google Scholar] [CrossRef]
- Philippines Official Gazette. Republic Act No. 10963: Tax Reform for Acceleration and Inclusion (TRAIN). Available online: https://www.officialgazette.gov.ph/2017/12/27/republic-act-no-10963/ (accessed on 7 March 2019).
- Department of Health Philippines. Joint Administrative Order No. 22018: Implementing Guideline on the Value-Added Tax (VAT) Exemption of the Sale of Drugs Prescribed for Diabetes, High Cholesterol and Hypertension. Available online: https://edpms.doh.gov.ph/download/DOF-DOH-BIR-FDA%20Joint%20Administrative%20Order%20No.%202.2018.pdf (accessed on 13 May 2019).
- World Health Organization. Measuring Medicine Prices, Availability, Affordability and Price Components, 2nd Edition. Available online: https://www.who.int/medicines/areas/access/OMS_Medicine_prices.pdf (accessed on 5 March 2019).
- Department of Health, Pharmaceutical Division. Philippine National Formulary 8th Edition Essential Medicines List. Available online: http://caro.doh.gov.ph/wp-content/uploads/2018/04/PNF-8th-edition.pdf (accessed on 13 May 2019).
- World Health Organization. 2017 Model List of Essential Medicines, 20th. Available online: https://www.who.int/medicines/news/2017/20th_essential_med-list/en/ (accessed on 21 May 2019).
- Food and Drug Administration Philippines. VAT-Exempt Drugs List for Hypertension, Diabetes and High Cholesterol. Available online: https://www.fda.gov.ph/vat-exempt-drugs-list/ (accessed on 21 May 2019).
- World Health Organization, Regional Office for the Eastern Mediterranean. Price, Availability and Affordability: An International Comparison of Chronic Disease Medicines. Available online: https://apps.who.int/iris/handle/10665/116493 (accessed on 12 December 2019).
- Ewen, M.; Zweekhorst, M.; Regeer, B.; Laing, R. Baseline assessment of WHO’s target for both availability and affordability of essential medicines to treat non-communicable diseases. PLoS ONE 2017, 12, e0171284. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Wagner, A.K.; Yang, S.; Jiang, M.; Zhang, F.; Ross-Degnan, D. Access to affordable medicines after health reform: Evidence from two cross-sectional surveys in Shaanxi Province, western China. Lancet Glob. Health 2013, 1, e227–e237. [Google Scholar] [CrossRef]
- Yang, C.; Hu, S.; Zhu, Y.; Zhu, W.; Li, Z.; Fang, Y. Evaluating access to oral anti-diabetic medicines: A cross-sectional survey of prices, availability and affordability in Shaanxi Province, Western China. PLoS ONE 2019, 14, e0223769. [Google Scholar] [CrossRef] [PubMed]
- Government PH. Salary Grade 2019: Fourth Tranche of Salary Standardization Law. Available online: https://governmentph.com/salary-grade-2019-table/ (accessed on 18 October 2019).
- FX-HISTORY OANDA. Exchange Rate US Dollar to Philippine Peso in August 1, 2019. Available online: https://www.oanda.com/fx-for-business/historical-rates/plans (accessed on 4 August 2019).
- Kaiser, A.H.; Hehman, L.; Forsberg, B.C.; Simangolwa, W.M.; Sundewall, J. Availability, prices and affordability of essential medicines for treatment of diabetes and hypertension in private pharmacies in Zambia. PLoS ONE 2019, 14, e0226169. [Google Scholar] [CrossRef] [PubMed]
- Ashigbie, P.G.; Rockers, P.C.; Laing, R.O.; Cabral, H.J.; Onyango, M.A.; Buleti, J.P.L.; Wirtz, V.J. Availability and prices of medicines for non-communicable diseases at health facilities and retail drug outlets in Kenya: A cross-sectional survey in eight counties. BMJ Open 2020, 10, e035132. [Google Scholar] [CrossRef] [PubMed]
- Ball, D.; Salenga, R. Pharmaceutical Policy in the Philippines. In Pharmaceutical Policy in Countries with Developing Healthcare Systems; Babar, Z.U., Ed.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 45–73. ISBN 978-3-319-51673-8. [Google Scholar]
- Khuluza, F.; Haefele-Abah, C. The availability, prices and affordability of essential medicines in Malawi: A cross-sectional study. PLoS ONE 2019, 14, e0212125. [Google Scholar] [CrossRef] [PubMed]
- Saeed, A.; Saeed, H.; Saleem, Z.; Fang, Y.; Babar, Z.U. Evaluation of prices, availability and affordability of essential medicines in Lahore Division, Pakistan: A cross-sectional survey using WHO/HAI methodology. PLoS ONE 2019, 14, e0216122. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Yang, S.; Yan, K.; Liu, J.; Zhao, J.; Fang, Y. Measuring access to medicines: A survey of prices, availability and affordability in Shaanxi province of China. PLoS ONE 2013, 8, e70836. [Google Scholar] [CrossRef] [PubMed]
- Ball, D.; Tisocki, K. Medicines Price Components in the Philippines. Available online: http://www.haiweb.org/wp-content/uploads/2015/07/Philippines-Report-2008-Price-Components-Pricing-Surveys.pdf (accessed on 18 June 2019).
- Philippines Official Gazette. Executive Order No. 821, s. 2009: Prescribing the Maximum Drug Retail Prices for Selected Drugs and Medicines that Address Diseases that Account for the Leading Causes of Morbidity and Mortality. Available online: https://www.officialgazette.gov.ph/2009/07/27/executive-order-no-821-s-2009/ (accessed on 25 November 2019).
- Reyes, C.; Tabuga, A.; Asis, R.; Datu, M.B. Improving Access to Affordable Medicines: Looking at Prevailing Prices and Distribution of Village Drugstores in the Philippines. Available online: https://pidswebs.pids.gov.ph/CDN/PUBLICATIONS/pidsdps1110_rev.pdf (accessed on 25 November 2019).
- Sarol, J.N., Jr. Effect of Government Mediated Access Pricing on Prices of Targeted Drugs in The Philippines. J. Asian Sci. Res. 2014, 4, 473–489. [Google Scholar]
- You, H.W.; Tajuddin, N.S.A.; Anwar, Y.A.S. Measuring Availability, Prices and Affordability of Ischaemic Heart Disease Medicines in Bangi, Selangor, Malaysia. Malays. J. Med. Sci. 2019, 26, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Feng, Q.; Kabba, J.A.; Yang, C.; Chang, J.; Jiang, M.; Zhao, M.; Yu, J.; Xu, S.; Li, Q.; et al. Prices, availability and affordability of insulin products: A cross-sectional survey in Shaanxi Province, western China. Trop. Med. Int. Health 2019, 24, 43–52. [Google Scholar] [CrossRef] [PubMed]


| Medicine Name | PEML | WHO/HAI LIST | Availability (%) | Median Unit Price (PHP) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OBs | LPGs | OBs | LPGs | |||||||
| PUB | PRV | PUB | PRV | PUB | PRV | PUB | PRV | |||
| acarbose | No | S | 0.0 | 19.0 | 0.0 | 2.4 | - | 13.75 | - | - |
| amlodipine | Yes | W | 0.0 | 57.1 | 91.7 | 85.7 | - | 21.86 | 2.00 | 5.00 |
| atenolol | Yes | W | 0.0 | 14.3 | 11.1 | 69.0 | - | 45.10 | 3.29 | 7.00 |
| atorvastatin | Yes | S | 0.0 | 52.4 | 38.9 | 83.3 | - | 38.25 | 11.00 | 14.00 |
| bisoprolol | Yes | G | 0.0 | 45.2 | 2.8 | 19.0 | - | 26.79 | - | 16.50 |
| candesartan | No | S | 0.0 | 2.4 | 0.0 | 45.2 | - | - | - | 15.00 |
| captopril | Yes | G | 0.0 | 4.8 | 77.8 | 83.3 | - | - | 3.00 | 8.00 |
| carvedilol | Yes | W | 0.0 | 0.0 | 36.1 | 73.8 | - | - | 13.00 | 9.75 |
| clonidine | Yes | S | 11.1 | 59.5 | 61.1 | 54.8 | 27.13 | 32.25 | 18.67 | 19.05 |
| dapagliflozin | No | S | 2.8 | 38.1 | 0.0 | 0.0 | - | 52.00 | - | - |
| empagliflozin | No | S | 0.0 | 45.2 | 0.0 | 0.0 | - | 59.00 | - | - |
| enalapril | Yes | S | 0.0 | 14.3 | 5.6 | 54.8 | - | 43.75 | - | 14.00 |
| enalapril + HCTZ | Yes | S | 0.0 | 7.1 | 0.0 | 9.5 | - | 42.56 | - | 13.35 |
| felodipine | Yes | S | 0.0 | 35.7 | 16.7 | 33.3 | - | 38.50 | 12.50 | 13.30 |
| fenofibrate | Yes | S | 0.0 | 26.2 | 13.9 | 31.0 | - | 95.00 | 31.00 | 31.25 |
| furosemide | Yes | W | 0.0 | 64.3 | 55.6 | 52.4 | - | 21.00 | 2.00 | 4.13 |
| glibenclamide | No | S | 0.0 | 26.2 | 19.4 | 42.9 | - | 8.00 | 5.50 | 3.75 |
| gliclazide | Yes | W | 0.0 | 47.6 | 55.6 | 57.1 | - | 9.65 | 5.00 | 6.70 |
| glimepiride | No | S | / | / | 0.0 | 66.7 | / | / | - | 10.00 |
| glipizide | No | S | 0.0 | 19.0 | 2.8 | 14.3 | - | 27.38 | - | 12.68 |
| hydralazine | Yes | W | / | / | 0.0 | 0.0 | / | / | - | - |
| hydrochloro-thiazide | Yes | W | / | / | 0.0 | 21.4 | / | / | - | 6.45 |
| indapamide | Yes | S | 0.0 | 21.4 | 0.0 | 2.4 | - | 40.25 | - | - |
| insulin glargine | No | S | 2.8 | 23.8 | 2.8 | 7.1 | - | 2907.50 | - | 1068.66 |
| insulin human isophane | Yes | W | 0.0 | 31.0 | 38.9 | 19.0 | - | 1431.00 | 158.57 | 759.00 |
| insulin human mixed * | Yes | S | 0.0 | 28.6 | 30.6 | 19.0 | - | 1440.50 | 252.00 | 822.50 |
| insulin human regular | Yes | W | 2.8 | 33.3 | 38.9 | 21.4 | - | 1425.00 | 127.00 | 850.00 |
| irbesartan | Yes | S | 0.0 | 52.4 | 30.6 | 57.1 | - | 24.25 | 9.00 | 15.75 |
| irbesartan + HCTZ | Yes | S | 0.0 | 47.6 | 11.1 | 16.7 | - | 31.50 | 21.88 | 19.50 |
| linagliptin | No | S | 0.0 | 54.8 | 0.0 | 0.0 | - | 60.75 | - | - |
| lisinopril | No | S | 0.0 | 11.9 | 0.0 | 2.4 | - | 67.50 | - | - |
| losartan | Yes | W | 0.0 | 42.9 | 86.1 | 92.9 | - | 19.35 | 1.15 | 9.50 |
| losartan + HCTZ | Yes | S | 0.0 | 28.6 | 30.6 | 69.0 | - | 22.63 | 6.00 | 12.50 |
| metformin | Yes | G | 0.0 | 45.2 | 86.1 | 90.5 | - | 14.25 | 1.34 | 3.25 |
| methyldopa | Yes | W | 8.3 | 54.8 | 52.8 | 26.2 | 24.00 | 22.75 | 14.29 | 9.00 |
| metoprolol | Yes | W | / | / | 58.3 | 78.6 | / | / | 2.00 | 3.25 |
| nifedipine | Yes | S | 0.0 | 19.0 | 16.7 | 11.9 | - | 44.40 | 18.48 | 12.42 |
| nimodipine | Yes | S | 0.0 | 26.2 | 5.6 | 2.4 | - | 45.75 | - | - |
| pioglitazone | No | S | 0.0 | 7.1 | 0.0 | 40.5 | - | 67.00 | - | 12.70 |
| pravastatin | No | S | / | / | 0.0 | 23.8 | / | / | - | 25.78 |
| propranolol | Yes | W | 0.0 | 47.6 | 30.6 | 40.5 | - | 25.50 | 13.97 | 4.00 |
| rosuvastatin | Yes | S | 0.0 | 42.9 | 27.8 | 64.3 | - | 85.93 | 20.50 | 20.50 |
| simvastatin | Yes | G | 0.0 | 23.8 | 61.1 | 81.0 | - | 33.88 | 4.49 | 9.83 |
| sitagliptin | No | S | 0.0 | 40.5 | 0.0 | 0.0 | - | 60.00 | - | - |
| spironolactone | Yes | W | 5.6 | 52.4 | 25.0 | 26.2 | - | 18.50 | 16.83 | 12.00 |
| telmisartan | Yes | S | 13.9 | 73.8 | 16.7 | 7.1 | 24.50 | 25.00 | 21.62 | 14.25 |
| telmisartan + HCTZ | Yes | S | 2.8 | 59.5 | 0.0 | 4.8 | - | 24.85 | - | - |
| valsartan | Yes | S | 0.0 | 47.6 | 13.9 | 38.1 | - | 25.25 | 22.14 | 19.24 |
| valsartan + HCTZ | Yes | S | 0.0 | 33.3 | 0.0 | 14.3 | - | 26.80 | - | 23.48 |
| verapamil | Yes | S | 0.0 | 31.0 | 0.0 | 14.3 | - | 93.50 | - | 42.46 |
| Medicine Name | Public Sector | Private Sector | Comparison between Public and Private Sectors | ||
|---|---|---|---|---|---|
| LPGs | OBs | LPGs | OBs/LPG | p-Value for LPGs * | |
| amlodipine | 2.00 | 21.86 | 5.00 | 4.36 | 0.000 |
| atenolol | 3.29 | 45.10 | 7.00 | 6.44 | 0.290 |
| atorvastatin | 11.00 | 38.25 | 14.00 | 2.73 | 0.417 |
| clonidine | 18.67 | 32.25 | 19.05 | 1.69 | 0.339 |
| felodipine | 12.50 | 38.50 | 13.30 | 2.89 | 0.741 |
| fenofibrate | 31.00 | 95.00 | 31.25 | 3.04 | 0.758 |
| furosemide | 2.00 | 21.00 | 4.13 | 5.08 | 0.006 |
| glibenclamide | 5.50 | 8.00 | 3.75 | 2.13 | 0.671 |
| gliclazide | 5.00 | 9.65 | 6.70 | 1.44 | 0.106 |
| insulin human isophane | 158.57 | 1431.00 | 759.00 | 1.89 | 0.000 |
| insulin human mixed % | 252.00 | 1440.50 | 822.50 | 1.75 | 0.004 |
| insulin human regular | 127.00 | 1425.00 | 850.00 | 1.68 | 0.001 |
| irbesartan | 9.00 | 24.25 | 15.75 | 1.54 | 0.194 |
| irbesartan + HCTZ | 21.88 | 31.50 | 19.50 | 1.62 | 0.850 |
| losartan | 1.15 | 19.35 | 9.50 | 2.04 | 0.000 |
| losartan + HCTZ | 6.00 | 22.63 | 12.50 | 1.81 | 0.009 |
| metformin | 1.34 | 14.25 | 3.25 | 4.38 | 0.000 |
| methyldopa | 14.29 | 22.75 | 9.00 | 2.53 | 0.219 |
| nifedipine | 18.48 | 44.40 | 12.42 | 3.57 | 0.715 |
| propranolol | 13.97 | 25.50 | 4.00 | 6.38 | 0.221 |
| rosuvastatin | 20.50 | 85.93 | 20.50 | 4.19 | 0.600 |
| simvastatin | 4.49 | 33.88 | 9.83 | 3.45 | 0.000 |
| spironolactone | 16.83 | 18.50 | 12.00 | 1.54 | 0.380 |
| telmisartan | 21.62 | 25.00 | 14.25 | 1.75 | 0.236 |
| valsartan | 22.14 | 25.25 | 19.24 | 1.31 | 0.943 |
| Medicine Name | Strength | Dosage Form | No. of Units Per Day | Total No. of Units Per Month | Day’s Wages to Pay for Treatment | |||
|---|---|---|---|---|---|---|---|---|
| Public Sector | Private Sector | |||||||
| OBs | LPGs | OBs | LPGs | |||||
| Antidiabetics | ||||||||
| gliclazide | 80 mg | cap/tab | 1 | 30 | - | 0.4 | 0.8 | 0.5 |
| insulin glargine | 100 IU/mL | 10 mL vial | - | 10 mL | - | - | 7.9 | 2.9 |
| insulin isophane | 100 IU/mL | 10 mL vial | - | 10 mL | - | 0.4 | 3.9 | 2.1 |
| insulin regular | 100 IU/mL | 10 mL vial | - | 10 mL | - | 0.3 | 3.9 | 2.3 |
| metformin | 500 mg | cap/tab | 2 | 60 | - | 0.2 | 2.3 | 0.5 |
| Lipid-lowering Agents | ||||||||
| atorvastatin | 20 mg | cap/tab | 1 | 30 | - | 0.9 | 3.1 | 1.1 |
| fenofibrate | 160 mg | cap/tab | 1 | 30 | - | 2.5 | 7.7 | 2.5 |
| simvastatin | 20 mg | cap/tab | 1 | 30 | - | 0.4 | 2.8 | 0.8 |
| Antihypertensives | ||||||||
| amlodipine | 5 mg | cap/tab | 1 | 30 | - | 0.2 | 1.8 | 0.4 |
| atenolol | 50 mg | cap/tab | 1 | 30 | - | 0.3 | 3.7 | 0.6 |
| bisoprolol | 5 mg | cap/tab | 1 | 30 | - | - | 2.2 | 1.3 |
| captopril | 25 mg | cap/tab | 2 | 60 | - | 0.5 | - | 1.3 |
| clonidine | 75 mcg | cap/tab | 2 | 60 | 4.4 | 3.0 | 5.2 | 3.1 |
| furosemide | 40 mg | cap/tab | 1 | 30 | - | 0.2 | 1.7 | 0.3 |
| losartan | 50 mg | cap/tab | 1 | 30 | - | 0.1 | 1.6 | 0.8 |
| methyldopa | 250 mg | cap/tab | 2 | 60 | 3.9 | 2.3 | 3.7 | 1.5 |
| nifedipine | 30 mg | SR cap/tab | 1 | 30 | - | 1.5 | 3.6 | 1.0 |
| propranolol | 40 mg | cap/tab | 2 | 60 | - | 2.3 | 4.2 | 0.7 |
| spironolactone | 25 mg | cap/tab | 1 | 30 | - | 1.4 | 1.5 | 0.9 |
| telmisartan | 40 mg | cap/tab | 1 | 30 | 2.0 | 1.8 | 2.0 | 1.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambojon, K.; Chang, J.; Saeed, A.; Hayat, K.; Li, P.; Jiang, M.; Atif, N.; Desalegn, G.K.; Khan, F.U.; Fang, Y. Prices, Availability and Affordability of Medicines with Value-Added Tax Exemption: A Cross-Sectional Survey in the Philippines. Int. J. Environ. Res. Public Health 2020, 17, 5242. https://doi.org/10.3390/ijerph17145242
Lambojon K, Chang J, Saeed A, Hayat K, Li P, Jiang M, Atif N, Desalegn GK, Khan FU, Fang Y. Prices, Availability and Affordability of Medicines with Value-Added Tax Exemption: A Cross-Sectional Survey in the Philippines. International Journal of Environmental Research and Public Health. 2020; 17(14):5242. https://doi.org/10.3390/ijerph17145242
Chicago/Turabian StyleLambojon, Krizzia, Jie Chang, Amna Saeed, Khezar Hayat, Pengchao Li, Minghuan Jiang, Naveel Atif, Gebrehaweria Kassa Desalegn, Faiz Ullah Khan, and Yu Fang. 2020. "Prices, Availability and Affordability of Medicines with Value-Added Tax Exemption: A Cross-Sectional Survey in the Philippines" International Journal of Environmental Research and Public Health 17, no. 14: 5242. https://doi.org/10.3390/ijerph17145242
APA StyleLambojon, K., Chang, J., Saeed, A., Hayat, K., Li, P., Jiang, M., Atif, N., Desalegn, G. K., Khan, F. U., & Fang, Y. (2020). Prices, Availability and Affordability of Medicines with Value-Added Tax Exemption: A Cross-Sectional Survey in the Philippines. International Journal of Environmental Research and Public Health, 17(14), 5242. https://doi.org/10.3390/ijerph17145242