4. Discussion and Future Directions
In this study, studies in the field of elderly health promotion from 2015 to October 2019 were summarized using a scoping review to investigate the research trends and distribution in the past five years in order to compare the results with studies compiled by Duplaga between 2000 and 2015. In this study, it was found that studies on health promotion in the elderly have increased annually. The topic of health promotion in the elderly is clearly receiving increasing scholarly attention.
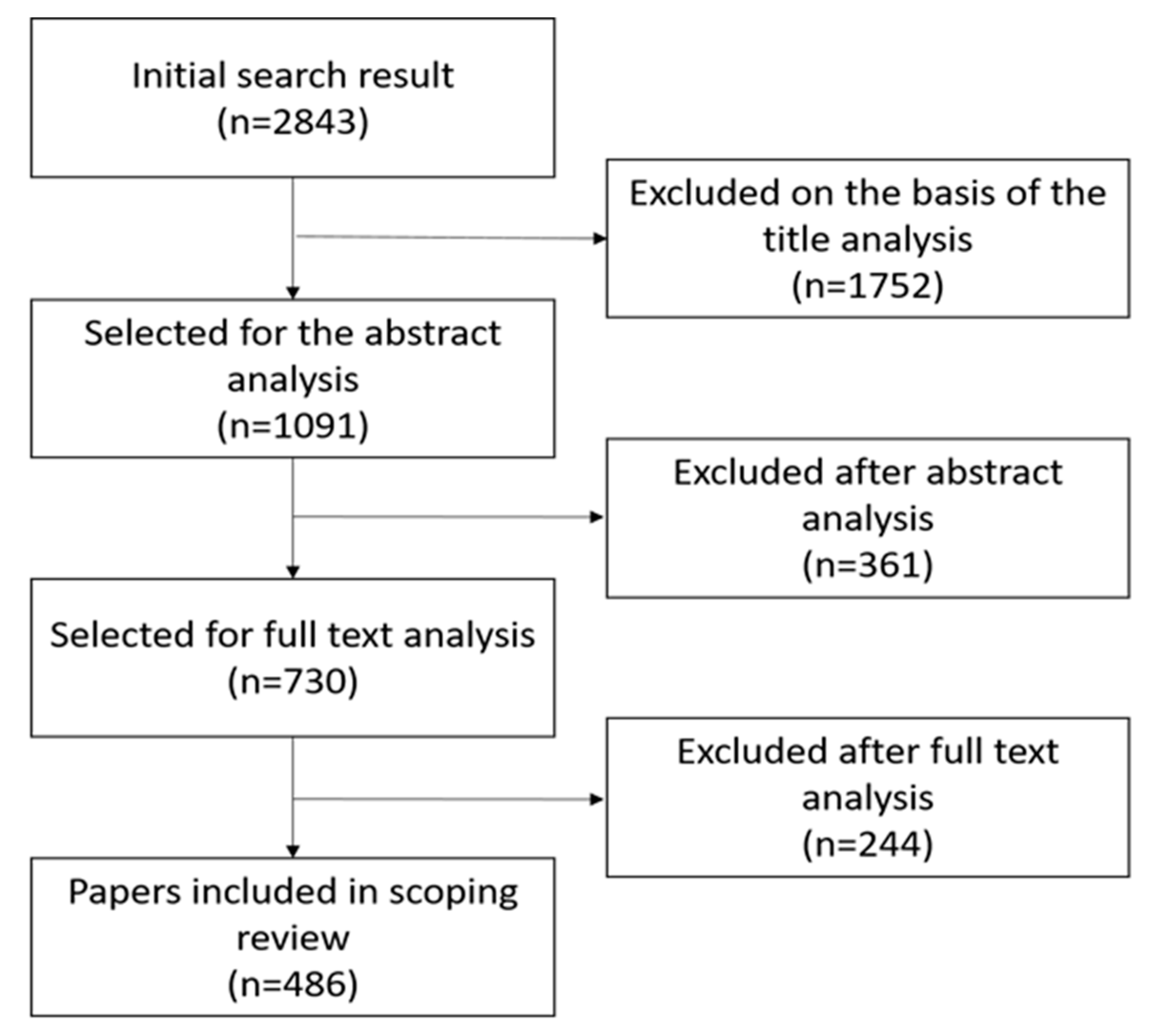
A total of 486 articles from 2015 to 2019 were included in our study, with an average of 97 articles per year, compared with the 334 articles included by Duplaga in the 15 years from 2000 to 2014, with an average of 23 articles per year. From the above statistics, it can be seen that there has been a significant increase in the research on health promotion in the elderly. We did not find any studies specifically targeted at a single gender. Of the 486 studies, only 10 (2.1%) were found on older women, and the proportion of gender-specific studies in Duplaga was also small. Only 33 (9.9%) of the 486 studies were gender-specific. Therefore, it was found that health promotion in the elderly covers all genders at present, which means that in the future, gender effects and effects associated with different groups are worthy of study.
According to the research results for intervention methods, the most commonly used research methods for health promotion in the elderly during the period under observation included health promotion (HP), screening (SC), primary prevention (PP) and social support (SS), and many systematic reviews and meta-analyses used two or more types of intervention methods for health promotion in the elderly. When each combination was examined separately, the top five found in this study were “Health promotion,” “Health promotion and Screening,” “Screening,” “Health promotion and Primary prevention,” and “Health promotion and Social support.” Based on these results, it was found that health promotion accounts for a significant proportion of the issues related to health promotion in the elderly, indicating that the issue of health promotion for the elderly is currently under active investigation. Compared with the results of Duplaga’s research, where primary prevention accounted for the majority of the issues, it can be inferred that the current issue of health promotion is not limited to primary prevention, but is being studied in a multi-faceted manner with a more diverse range of topics and interventions. To compare the present study with that conducted by Duplaga et al. [
4], we provide a table (
Supplementary 4) including a comparison of the aims, numbers of studies included, publication years, databases, target areas of interventions, general area of interventions, specific gender target, and classification differences.
Based on the results, purpose-oriented studies can be ranked in the following order: disease-oriented, physical activity, general health, quality of life, general health, frailty, nutrition, mental health, psychosocial functioning, independence, sleep quality, disability, and addiction. The classification results also reveal a trend in multi-purpose-oriented discussions in some of the studies, including: disease-oriented vs. physical activity, physical activity vs. general health, quality of life, cognitive function, disease-oriented vs. nutrition, general health vs. general health, etc. This phenomenon suggests that the issue of health promotion in the elderly needs to be studied from many perspectives, rather than discussed as a single topic. It is also worth noting that the results of the author’s classifications are consistent with Duplaga’s top four results, with the first issue in all studies being treating and preventing disease, followed by physical activity, general health, and quality of life. The following is a discussion of the top five categories.
Among the purpose-oriented classifications, those related to diseases predominated and covered a relatively wide range, such as knee arthritis or sarcopenia of the musculoskeletal system, Alzheimer’s disease, and Parkinson’s disease. Psychological disorders included depression, bipolar disorder, post-traumatic stress disorder, and delirium. Chronic diseases included diabetes, hypertension, and kidney disease. Other illnesses included anorexia and dry mouth. Multiple complications were also the target of some studies. The authors in the literature attempted a variety of interventions, such as medication, physical activity, diet plans, and aromatherapy, to slow or even cure age-related illnesses. Due to the high heterogeneity of health status among the elderly and the significant influence of diseases on health promotion in the elderly, it is necessary to consider the influence of disease during the health promotion of the elderly and to create a health promotion policy based on a multi-dimensional assessment. Therefore, in the future, more in-depth discussion and research on specific diseases would certainly lead to remarkable results in the promotion of health in the elderly.
The physical activity category was the second largest among the purpose-oriented categories. It mainly focuses on sports, such as aerobic exercise, dancing, Tai-Chi, yoga, water aerobics, etc. However, some studies investigated digital behavior interventions, Pilates training, resistance training, physical activity monitoring, etc. In terms of type, most of the studies were related to disease, aging, and cognitive function, so physical activity was used fairly often as an intervention. In addition, Hu et al. conducted a scoping review in 2019 on the involvement of elderly people in physical activities as interventions who did not receive adequate medical services. The results suggest that interventions that are appropriate to the characteristics of older persons with disabilities should be tailored to their race, socioeconomic status, and level of physical disability [
8]. It was observed that the ethnicity, socio-economic status, cultural characteristics, and diseases of the target subjects should be considered as factors in the design of interventional physical activities for the elderly.
The general health category was the third largest among the purpose-oriented categories and covered a wide range of areas, typically including physical functioning, role functioning, social functioning, mental health, health perception, and pain [
9]. Therefore, if the intervention method discussed in each study contained three or more of the above conditions, it was included in this classification. From the classification results, it was found that there were more studies focusing on multi-field comprehensive analyses, while the analysis of a single factor tended to decrease over the period under consideration. For example, in this category, some studies discussed the effect of exercise on the overall health of the elderly and further discussed the impact on cognitive function. There were also some studies on intervention and general health in specific groups (e.g., elderly people in prison, veterans, women during menopause, elderly volunteers/workers, etc.). This classification involves a variety of targets and is comprehensive, and is therefore likely to be one of the research focuses of health promotion in the elderly in the future.
The fourth largest category was quality of life, which comprises health status, social contacts, and other elements [
10] and is also related to the impact of declines in function [
11]. In the screening results for this project, in addition to some of the studies sharing common research themes with other interventions such as physical activity, mental health, psychosocial functioning, sleep quality, etc., there were also studies focusing on independent topics. For example, there were many papers on prevention of abuse and neglect of older adults, and some other papers on the prevention of suicidal behavior and reduction in suicidal ideation, reminiscence therapy interventions, environmental and behavioral modifications, preventive house visits, lifelong learning, etc. The research themes in the relevant studies were quite diverse and will contribute to the formulation of future health and social services policies for the elderly [
10].
The fifth largest category in the purpose-oriented categories was cognitive function, which was compared to “frailty” based on Duplaga’s screening results (2016), which was the only difference among the top five indices. According to the current study, cognitive decline is one of the symptoms of dementia and is not directly related to aging, physical health status, and pre-morbid activity patterns [
12]. This discourse fits the results of the present screening. There was an overwhelming majority of the studies related to dementia. The results of the screening also reveal a wide range of interventions, including non-pharmacological interventions such as physical activity, structural brain plasticity-induced training, video games, electronic-assistive devices, etc. In the face of dementia, which has a longer course of disease and high incidence rates [
13], it is necessary to specify multiple interventions as a research topic to find more effective treatments intended to slow cognitive decline.
In addition to focusing on the distribution of the studies under consideration in this study, studies on the application of eHealth technology were also examined. According to the findings, eHealth technology has been used in recent years as an intervention tool for health promotion. These tools include virtual reality (n = 3), smart homes and home health monitoring technologies (n = 1), socially assistive robots (n = 5), and electronic assistive technology (n = 3).
Some studies explored whether the use of virtual reality technology can improve problems that lead to debilitation in the elderly and prevent them from falling. The results show that virtual reality games are better than traditional interventions for improving balance and preventing falls in the elderly and can strengthen the awareness of the harm caused by falls in the elderly [
14]. Scoglio and Abdi et al. investigated whether socially assistive robots can help the mental health and well-being of the elderly, and their findings suggested that there is positive potential for companionship, cognition, and mental health improvements associated with their use. However, due to the limited number of people involved in the related research and some methodological problems, the helpfulness and value of socially assistive robots in the health promotion of elderly people still requires further research. [
15,
16]. Elderly people have both positive and negative views of socially assistive robots in geriatric care. A further understanding of experience with and willingness toward use is needed to consider the use of socially assistive robots in this area [
17]. Brims and Oliver suggested that the effectiveness of assistive technology in reducing hospital admission rates is inconclusive. However, assistive technology has been tested to reduce the risk of falls, accidents, and other risky behavior, as well as to improve home safety for people with dementia [
18]. Nevertheless, Roest’s study indicated that it is not clear whether AT can actually help resolve dementia-related memory problems [
19]. Tangcharoensathien’s research pointed out that the promotion of assistive technologies requires the establishment of a policy framework and the encouragement of assistive technology product development through the training of professionals and support and promotion programs [
20]. Liu et al. reviewed the impact of smart homes and health monitoring technologies on the health of the elderly, and their results show that eHealth technology could be used to monitor daily life, cognitive decline, mental health, and heart conditions in elderly individuals with complex needs. However, smart homes and home health monitoring technologies are not yet mature [
21].
The authors found that most of the studies on eHealth technology interventions were focused on treatment rather than prevention. Seven out of 12 studies using eHealth technology focused more on treatment. For example, Roest et al. [
19] focused on how to make use of assistive technology (AT) to help dementia patients and their caregivers manage their daily lives and enhance their safety [
17]. Abdi et al. [
15] suggested five roles for social assistive technology (SAR), which included affective therapy, cognitive training, social facilitation, companionship, and physiological therapy. Four of the studies focused more on prevention. Neri et al. studied improvements in balance and mobility in the elderly [
17]. Liu et al. investigated the interaction between smart homes and home health monitoring technologies and life functioning, cognitive ability, mental health, and cardiac status among older adults [
17]. There was also one study that focused on both treatment and prevention, Afsaneh et al. [
22] found that self-care ATs can efficiently reduce care hours and also help to increase levels of independence. In this study, only 2.5% (
n = 12) of the studies were on the use of eHealth technologies among the searchable reviews. However, with the rapid development of technology (e.g., where robots may gradually replace people, and 5G technology will be mature), older people are becoming increasingly more receptive to technology. It is expected that the use of eHealth technology as an intervention tool for health promotion in the elderly will become a trend, and in the future, more in-depth research can be conducted on the use of eHealth technology as an intervention tool for health promotion in the elderly. Therefore, before using eHealth technology in this way, it is important to know how receptive older people are to eHealth technology in order to develop strategies for its use among different groups, such as women, aborigines, and people with dementia. In this study, the results of these studies also show that eHealth technology as a means of health promotion for the elderly is not yet mature and requires larger samples and more rigorous research designs.
The present study has the following limitations: First, there were different research standards for each paper. Through the comparison, it was found that in fact, there are different types of studies, such as meta-analyses and systematic reviews, different types of participants, including different health conditions and ages, different types of interventions, and various outcome measures and analysis technologies used for research statistics and analysis purposes. This may have led to errors in the literature comparison. Secondly, not all of the studies under review had specific results due to such things as time limitation, outcomes being both positive and negative, and a lack of maturity of the technologies leading to adequate experience and data to analyze, etc. Muellmann et al.’s study noted that due to a lack of research time, it was impossible to confirm whether long-term health interventions increase physical activity in 55 year-old individuals [
17]. Vandemeulebroucke’s research mentioned that there were both positive and negative results found for the use of socially assistive robots in the area of elderly care. They demonstrated that technology intervention in the area of elderly care is not yet mature, and it is necessary to learn more about the past life experiences of the elderly and to use more rigorous research designs in more groups [
17]. In addition, some studies mentioned that before using technology as an intervention for health promotion in the elderly, it is important to determine how receptive older people are to this technology in order to develop strategies suitable for different groups, such as women, aborigines, and people with dementia. It was also mentioned in many studies that more study is needed for corroboration due to the shortage of existing research on this topic. Therefore, there is also no definitive conclusion as to whether technology promotes behavioral change [
23]. Another limitation is language restrictions. This study includes reviews written in English. Further studies are suggested to include works written in other languages.
It was found in this study that the presence of diseases and co-morbidities is an important direction of concern for health promotion in the elderly. Health promotion in the elderly typically has three purposes: maintaining and increasing function, maintaining or improving self-managed health, and creating active social networks. However, all of these aims are intended to contribute to independence and a better quality of life. Older people struggle to stay healthy, not only because of the challenges of aging, but also because they are more likely to be ostracized and socially isolated than younger people. However, subjective or psychosocial factors are often neglected in the implementation or formulation of advanced age health promotion programs. Therefore, it is important to go beyond the physical to further explore the psychosocial components of a strategy and how these factors affect overall happiness. Self-reported survey data can be used to measure psychosocial factors (e.g., loneliness, self-efficacy) so as to provide a clearer picture of the real needs of this population.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}