Modelling the Effectiveness of Epidemic Control Measures in Preventing the Transmission of COVID-19 in Malaysia

 , , , ,
, , , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Data Analysis
2.3. Model Formulation
- (1)
- We assumed that international travel had introduced transmission into the local setting but then played no further role in local transmissions, assuming a closed population. This was mitigated by travel restrictions and entry/exit point screening, which were enforced on 25 January 2020, limiting importation of cases.
- (2)
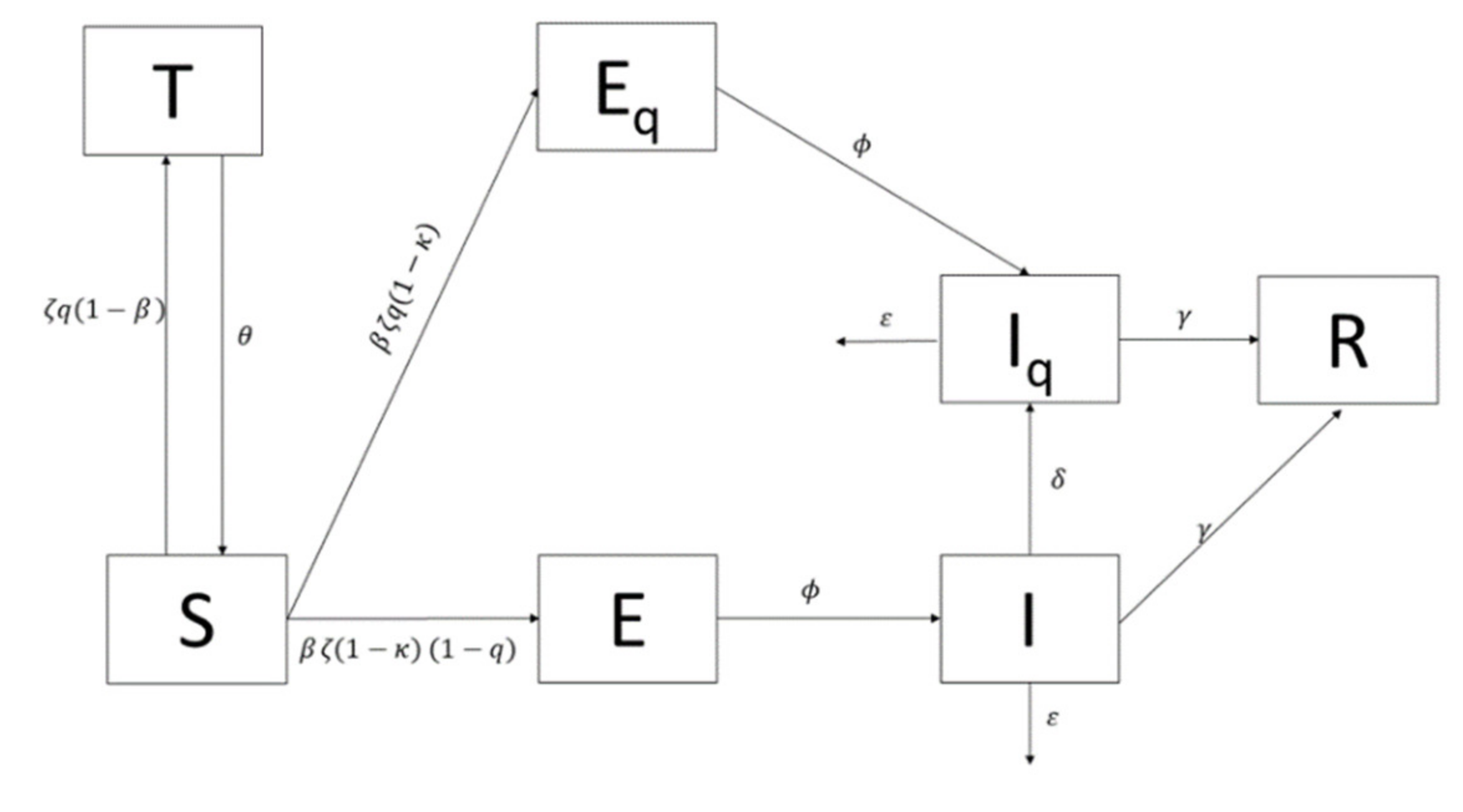
- Malaysia’s total population, denoted as N, was divided into an extended SEIR compartmental model, distinguishing between the traced and untraced populations and incorporating the current control measures and precautions taken. Apart from the basic compartments of SEIR (Susceptible (S), Exposed (E), Infected (I), and Recovered (R)), this model had additional three compartments, namely traced close-contact and a negative test result population (T), traced exposed close-contact and positive test result population (Eq), and the infected isolated (Iq). It was assumed that, initially, the entire Malaysian population was susceptible, hence S0 = N.
- (3)
- All Malaysian residents were assumed to be of equal measure in their likelihood to contract and transmit the virus, assuming there was homogenous mixing within the population; however, we assumed that only 67% of the population would be susceptible based on the concept of herd immunity [24]. Current literature on transmission of COVID-19 has suggested that there is no strong evidence to support asymptomatic transmission and therefore our model only accounted for symptomatic transmission [24].
- (4)
- A constant population was assumed due to the short time period for the model development and projection, wherein changes of birth and death rates would be negligible.
- (5)
- Some of the parameters used were developed based on the outbreak data in China. As such, we assumed homogeneity of the disease dynamics between China and Malaysia.
2.4. Model Simulation
3. Results
3.1. Outbreak Simulation With No MCO Measures
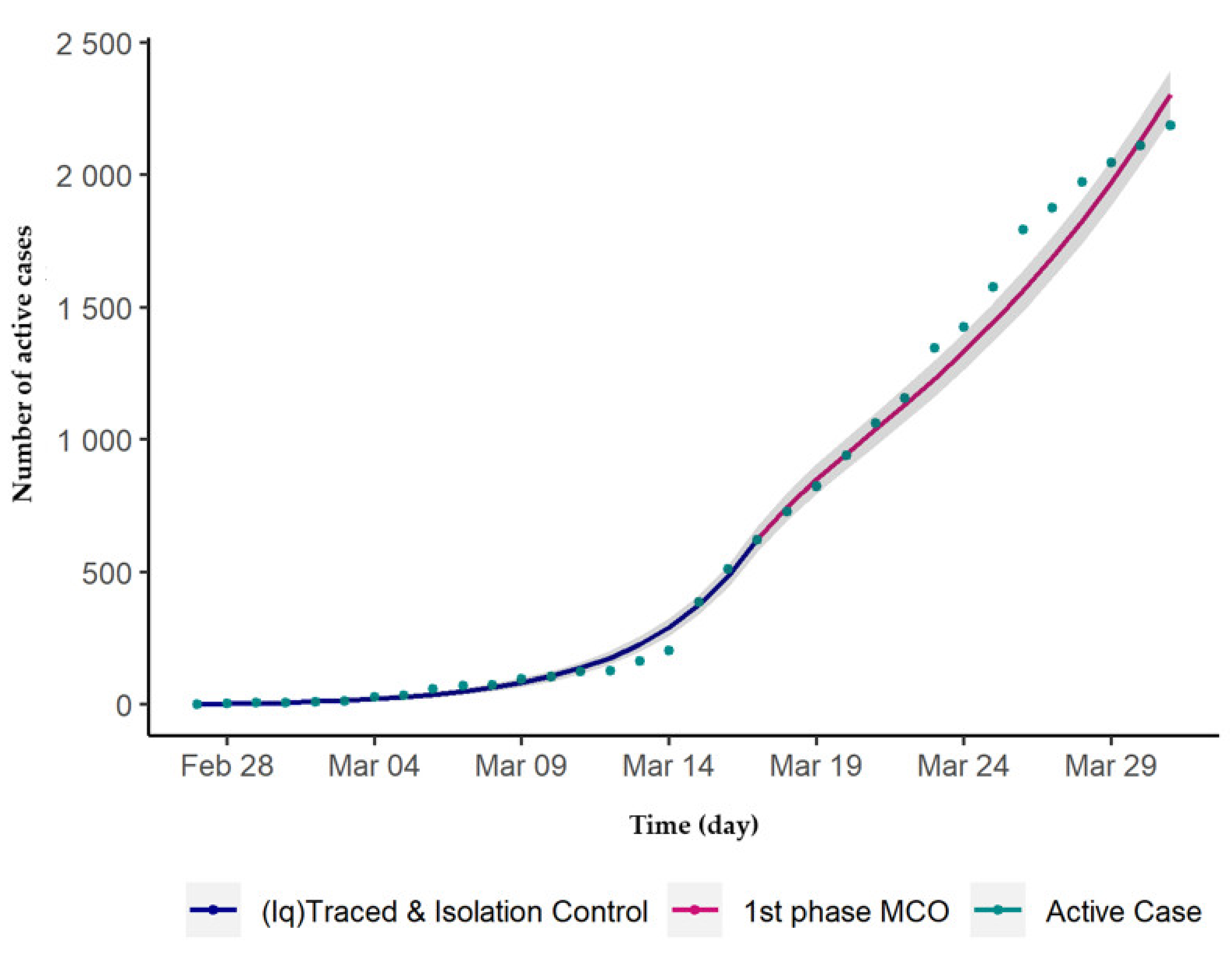
3.2. Outbreak Simulation with MCO Measures
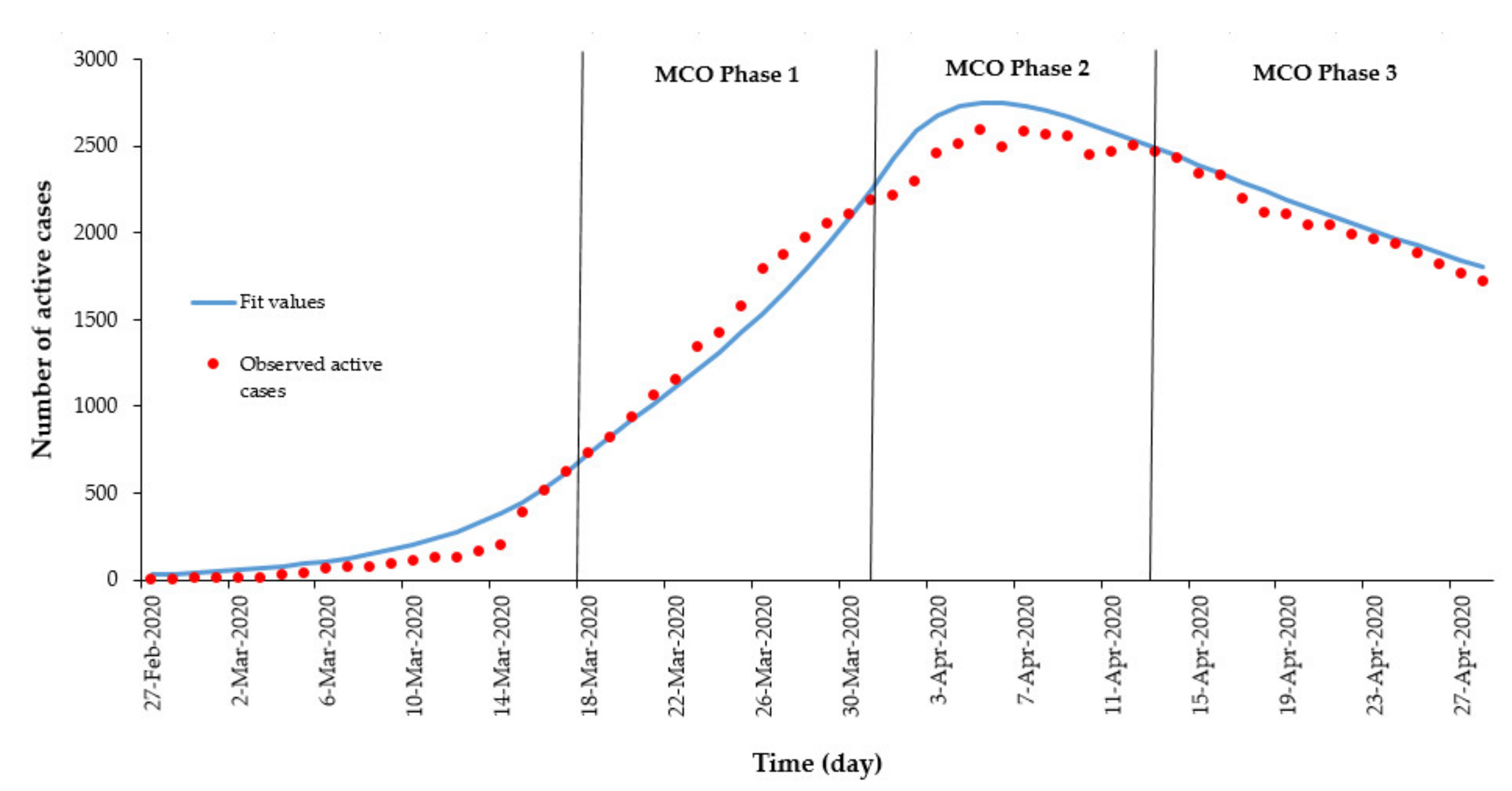
3.3. Comparison of Outbreak Simulation With and Without MCO Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 (accessed on 15 March 2020).
- Ministry of Health (MOH) Malaysia. COVID-19 (Maklumat Terkini). 2020. Available online: http://www.moh.gov.my/index.php/pages/view/2019-ncov-wuhan (accessed on 15 March 2020).
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). 2020. Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 15 March 2020).
- Read, J.M.; Bridgen, J.R.; Cummings, D.A.; Ho, A.; Jewell, C.P. Novel coronavirus 2019-nCoV: Early estimation of epidemiological parameters and epidemic forecasts. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Imai, N.; Dorigatti, I.; Cori, A.; Riley, S.; Ferguson, N.M. Estimating the potential total number of novel Coronavirus cases in Wuhan City, China. Imp. Coll. Lon. 2020, 1–4. [Google Scholar] [CrossRef]
- Riou, J.; Althaus, C.L. Pattern of early human-to-human transmission of Wuhan 2019-nCoV. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Hu, J.; Kang, M.; Lin, L.; Zhong, H.; Xiao, J.; He, G.; Song, T.; Huang, Q.; Rong, Z.; et al. Transmission dynamics of 2019 novel coronavirus (2019-nCoV). SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Zhao, S.; Musa, S.S.; Lin, Q.; Ran, J.; Yang, G.; Wang, W.; Lou, Y.; Yang, L.; Gao, D.; He, D.; et al. Estimating the Unreported Number of Novel Coronavirus (2019-nCoV) Cases in China in the First Half of January 2020: A Data-Driven Modelling Analysis of the Early Outbreak. J. Clin. Med. 2020, 9, 388. [Google Scholar] [CrossRef] [Green Version]
- Shen, M.; Peng, Z.; Xiao, Y.; Zhang, L. Modelling the epidemic trend of the 2019 novel coronavirus outbreak in China. bioRxiv 2020. [Google Scholar] [CrossRef]
- Kermack, W.O.; McKendrick, A.G. Contributions to the mathematical theory of epidemics-II. The problem of endemicity. Bull. Math Biol. 1991, 138, 55–83. [Google Scholar]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Hao, X.; Lau, E.H.Y.; Wong, J.Y.; Leung, K.S.M.; Wu, J.T.; Cowling, B.J.; Leung, G.M. Real-time tentative assessment of the epidemiological characteristics of novel coronavirus infections in Wuhan, China, as at 22 January 2020. Eurosurveillance 2020, 25, 2000044. [Google Scholar] [CrossRef]
- Kucharski, A.J.; Russell, T.W.; Diamond, C.; Liu, Y.; Edmunds, J.; Funk, S.; Eggo, R.M.; Sun, F.; Jit, M.; Munday, J.D.; et al. Early dynamics of transmission and control of COVID-19: A mathematical modelling study. Lancet Inf. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Tang, B.; Wang, X.; Li, Q.; Luigi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the Transmission Risk of the 2019-nCoV and Its Implication for Public Health Interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Wang, Z.; Dong, Y.; Chang, R.; Xu, C.; Yu, X.; Zhang, S.; Tsamlag, L.; Shang, M.; Huang, J.; et al. Phase-adjusted estimation of the number of Coronavirus Disease 2019 cases in Wuhan, China. Cell Discov. 2020, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. The incubation period of 2019-nCoV infections among travellers from Wuhan, China. Eurosurveillance 2020, 25, 2000062. [Google Scholar]
- Linton, N.M.; Kobayashi, T.; Yang, Y.; Hayashi, K.; Akhmetzhanov, A.R.; Jung, S.-M.; Yuan, B.; Kinoshita, R.; Nishiura, H. Epidemiological characteristics of novel coronavirus infection: A statistical analysis of publicly available case data. medRxiv 2020. [Google Scholar] [CrossRef]
- Chen, J. Pathogenicity and transmissibility of 2019-nCoV—A quick overview and comparison with other emerging viruses. Microbes Infect. 2020, 22, 69–71. [Google Scholar] [CrossRef] [PubMed]
- The Star. Coronavirus: New Study Finds Incubation Period of up to 24 Days. 2020. Available online: https://www.thestar.com.my/news/regional/2020/02/11/coronavirus-new-study-finds-incubation-period-of-up-to-24-days (accessed on 16 March 2016).
- Kucharski, A.J.; Althaus, C.L. The role of superspreading in middle east respiratory syndrome coronavirus (Mers-CoV) transmission. Eurosurveill. 2015, 20, 14–18. [Google Scholar] [CrossRef]
- Wang, W.; Ruan, S. Simulating the SARS outbreak in Beijing with limited data. J. Theor. Biol. 2004, 227, 369–379. [Google Scholar] [CrossRef]
- Dénes, A.; Gumel, A.B. Modeling the impact of quarantine during an outbreak of Ebola virus disease. Infect. Dis. Model. 2019, 4, 12–27. [Google Scholar] [CrossRef]
- Ng, T.W.; Turinici, G.; Danchin, A.; Ng, W.T.; Turinici, G.; Danchin, A. A double epidemic model for the SARS propagation. Biomed. Cent. Infect. Dis. 2003, 3, 1–16. [Google Scholar] [CrossRef]
- Nishiura, H.; Patanarapelert, K.; Sriprom, M.; Sarakorn, W.; Sriyab, S.; Ming Tang, I. Modelling potential responses to severe acute respiratory syndrome in Japan: The role of initial attack size, precaution, and quarantine. J. Epidemiol. Commun. Health 2004, 58, 186–191. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 7 February 2020).
- Soetaert, K.; Petzoldt, T.; Setzer, R.W. Solving differential equations in R: Package deSolve. J. Stat. Softw. 2010, 33, 1–25. [Google Scholar] [CrossRef]
- Wickham, H. Ggplot2 Elegant Graphics for Data Analysis; Journal of the Royal Statistical Society: Series A (Statistics in Society); Springer: Berlin, Germany, 2016. [Google Scholar]
- Team. BB and RDC. Bbmle: Tools for General Maximum Likelihood Estimation. R Package Version 1.0.23.1. 2020. Available online: https://cran.r-project.org/package=bbmle (accessed on 7 February 2020).
- Labadin, J.; Hong, B.H. Transmission Dynamics of 2019-nCoV in Malaysia. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Kocijan, J. Modelling and Control of Dynamic Systems Using Gaussian Process Models; Springer: New York, NY, USA, 2016; p. 121. [Google Scholar]
- Ng, Y.; Li, Z.; Chua, Y. Evaluation of the Effectiveness of Surveillance and Containment Measures for the First 100 Patients with COVID-19 in Singapore—January 2–February 29, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, J. Feasibility of controlling 2019-nCoV outbreaks by isolation of cases and contacts. Lancet 2020. [Google Scholar] [CrossRef]
- Fraser, C.; Riley, S.; Anderson, R.M.; Ferguson, N.M. Factors that make an infectious disease outbreak controllable. Proc. Natl. Acad. Sci. USA 2004, 101, 6146–6151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majumder, M.; Mandl, K.D. Early Transmissibility Assessment of a Novel Coronavirus in Wuhan, China. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.; Yiting, N.; Marshare, P. Transmission dynamics of the COVID-19 outbreak and effectiveness of government interventions: A data-driven analysis. J. Med. Virol. 2020, 92, 1–15. [Google Scholar] [CrossRef] [Green Version]
- O’Hagan, J.J.; Lipsitch, M.; Hernán, M.A. Estimating the per-exposure effect of infectious disease interventions. Epidemiology 2014, 25, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Tang, B.; Xia, F.; Tang, S.; Bragazzi, N.L.; Li, Q.; Sun, X.; Liang, J.; Xiao, Y.; Wu, J. The effectiveness of quarantine and isolation determine the trend of the COVID-19 epidemics in the final phase of the current outbreak in China. Int. J. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- The Guardian. The Coronavirus Pandemic: Visualising the Global Crisis. 2020. Available online: https://www.theguardian.com/world/2020/mar/13/coronavirus-pandemic-visualising-the-global-crisis (accessed on 15 March 2020).
- Brennan, D.; China Claims Peak of Coronavirus Epidemic Has Passed as New Cases Decline and More than 60,000 Have Recovered. Newsweek. 2020. Available online: https://www.newsweek.com/china-says-passed-peak-coronavirus-epidemic-covid-19-1491863 (accessed on 15 March 2020).
- Kupferschmidt, K.; Cohen, J.; China’s Aggressive Measures Have Slowed the Coronavirus. They May Not Work in Other Countries. American Association for the Advancement of Science. 2020. Available online: https://www.sciencemag.org/news/2020/03/china-s-aggressive-measures-have-slowed-coronavirus-they-may-not-work-other-countries (accessed on 19 March 2020).
- Rapoza, K. China and South Korea Models Seem Like Only Way to Contain COVID-19. Fobes. 2020. Available online: https://www.forbes.com/sites/kenrapoza/2020/03/12/china-and-south-korea-models-seem-like-only-way-to-contain-covid-19/#1a35db1447d3 (accessed on 19 March 2020).
- Ferguson, M.; Laydon, D.; Gilani, G.; Imai, N.; Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand. Imperial College COVID-19 Response Team. 2020, pp. 1–20. Available online: https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf (accessed on 22 March 2020).
- Randolph, H.; Barreiro, L. Herd Immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.J.; Li, L.M. Advances on presymptomatic or asymptomatic carrier transmission of COVID-19. Eur. PMC 2020, 41, 485–488. [Google Scholar]
- Ngonghala, C.N.; Iboi, E.; Eikenberry, S.; Scotch, M.; MacIntyre, C.R.; Bonds, M.H.; Gumel, A.B. Mathematical assessment of the impact of non-pharmaceutical interventions on curtailing the 2019 novel Coronavirus. Math. Biosci. 2020, 108364. [Google Scholar] [CrossRef]
- Venkatarao, E.; Patil, R.R.; Prasad, D.; Anasuya, A.; Samuel, R. Monitoring data quality in syndromic. surveillance: Learnings from a resource limited setting. J. Glob. Infect. Dis. 2012, 4, 120–127. [Google Scholar]
- Laws of Malaysia. Prevention and Control Of Infectious Diseases Act 1988. Available online: https://www.moh.gov.my/index.php/database_stores/attach_download/317/19 (accessed on 13 June 2020).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Description | Value | Source |
|---|---|---|---|
| N | Total human population in Malaysia | 32,600,000 | (DOSM 2019) |
| Incubation Period | 6.5 | [16] | |
| β | Probability of susceptible become infectious per contact | 0.052 | Calibrated using data (27 February to 17 March 2020) |
| Infectious period | 3.6 | [4] | |
| ε | Death rate due to COVID-19 | 0 | MOH (as per 16 March 2020) |
| ζ | The average number of contacts per day per case | 25 | Calibrated using data (27 February to 17 March 2020) |
| q | The proportion of close contact traced per day | 0.23 | Calibrated using data (27 February to 17 March 2020) |
| The duration of quarantine | 14 | MOH | |
| κ | The proportion of exposed persons who performed effective precautions | 0.05 | [24] |
| δ | The mean daily rate at which infectious cases are isolated | 0.03 | [24] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gill, B.S.; Jayaraj, V.J.; Singh, S.; Mohd Ghazali, S.; Cheong, Y.L.; Md Iderus, N.H.; Sundram, B.M.; Aris, T.B.; Mohd Ibrahim, H.; Hong, B.H.; et al. Modelling the Effectiveness of Epidemic Control Measures in Preventing the Transmission of COVID-19 in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 5509. https://doi.org/10.3390/ijerph17155509
Gill BS, Jayaraj VJ, Singh S, Mohd Ghazali S, Cheong YL, Md Iderus NH, Sundram BM, Aris TB, Mohd Ibrahim H, Hong BH, et al. Modelling the Effectiveness of Epidemic Control Measures in Preventing the Transmission of COVID-19 in Malaysia. International Journal of Environmental Research and Public Health. 2020; 17(15):5509. https://doi.org/10.3390/ijerph17155509
Chicago/Turabian StyleGill, Balvinder Singh, Vivek Jason Jayaraj, Sarbhan Singh, Sumarni Mohd Ghazali, Yoon Ling Cheong, Nuur Hafizah Md Iderus, Bala Murali Sundram, Tahir Bin Aris, Hishamshah Mohd Ibrahim, Boon Hao Hong, and et al. 2020. "Modelling the Effectiveness of Epidemic Control Measures in Preventing the Transmission of COVID-19 in Malaysia" International Journal of Environmental Research and Public Health 17, no. 15: 5509. https://doi.org/10.3390/ijerph17155509