Psychosocial Resources for Hedonic Balance, Life Satisfaction and Happiness in the Elderly: A Path Analysis


Abstract
:1. Introduction
Associations between Affect Balance, Life Satisfaction and Happiness with Psychosocial Variables in Older Adults
2. Materials and Methods
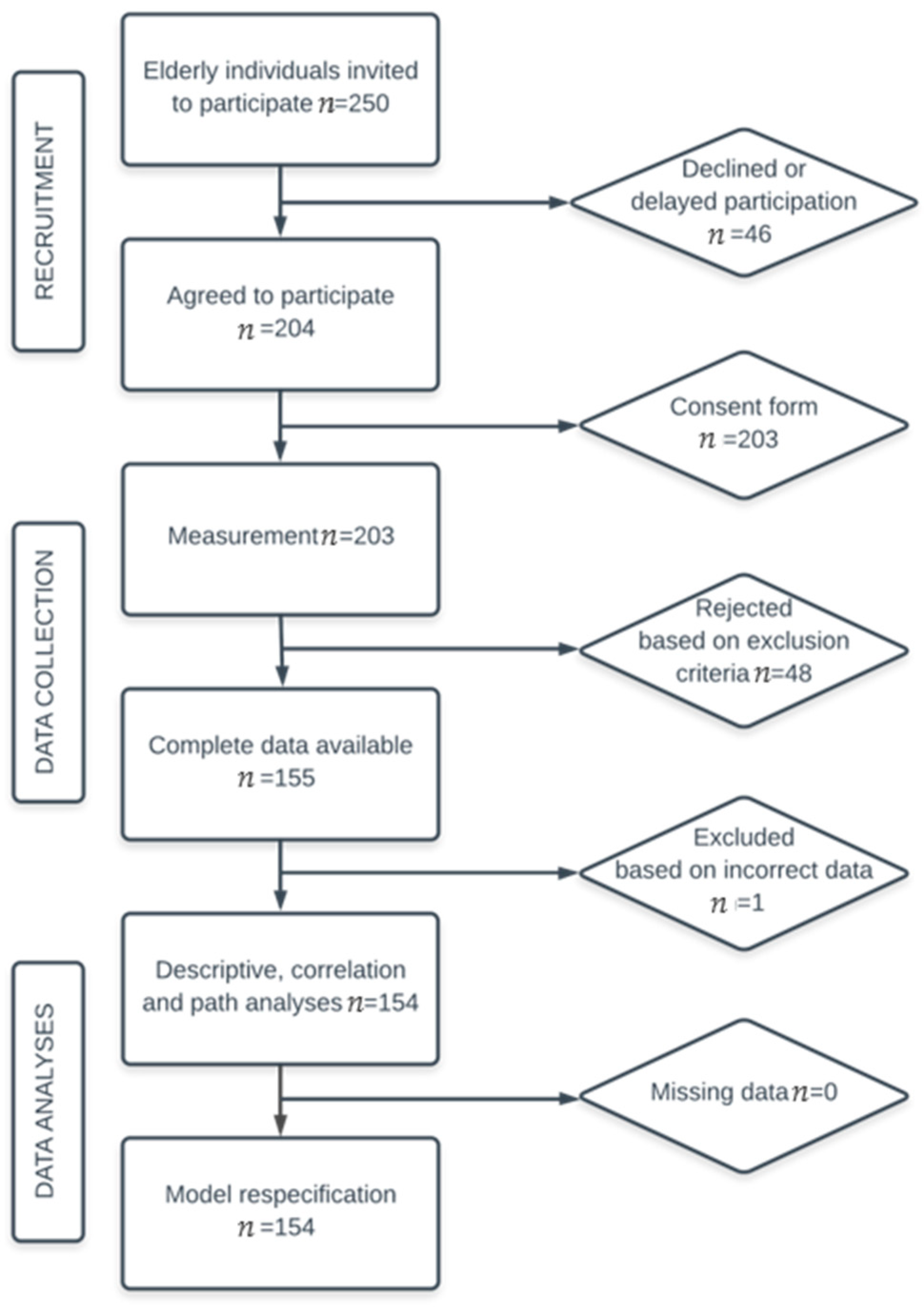
2.1. Participants
2.2. Measures
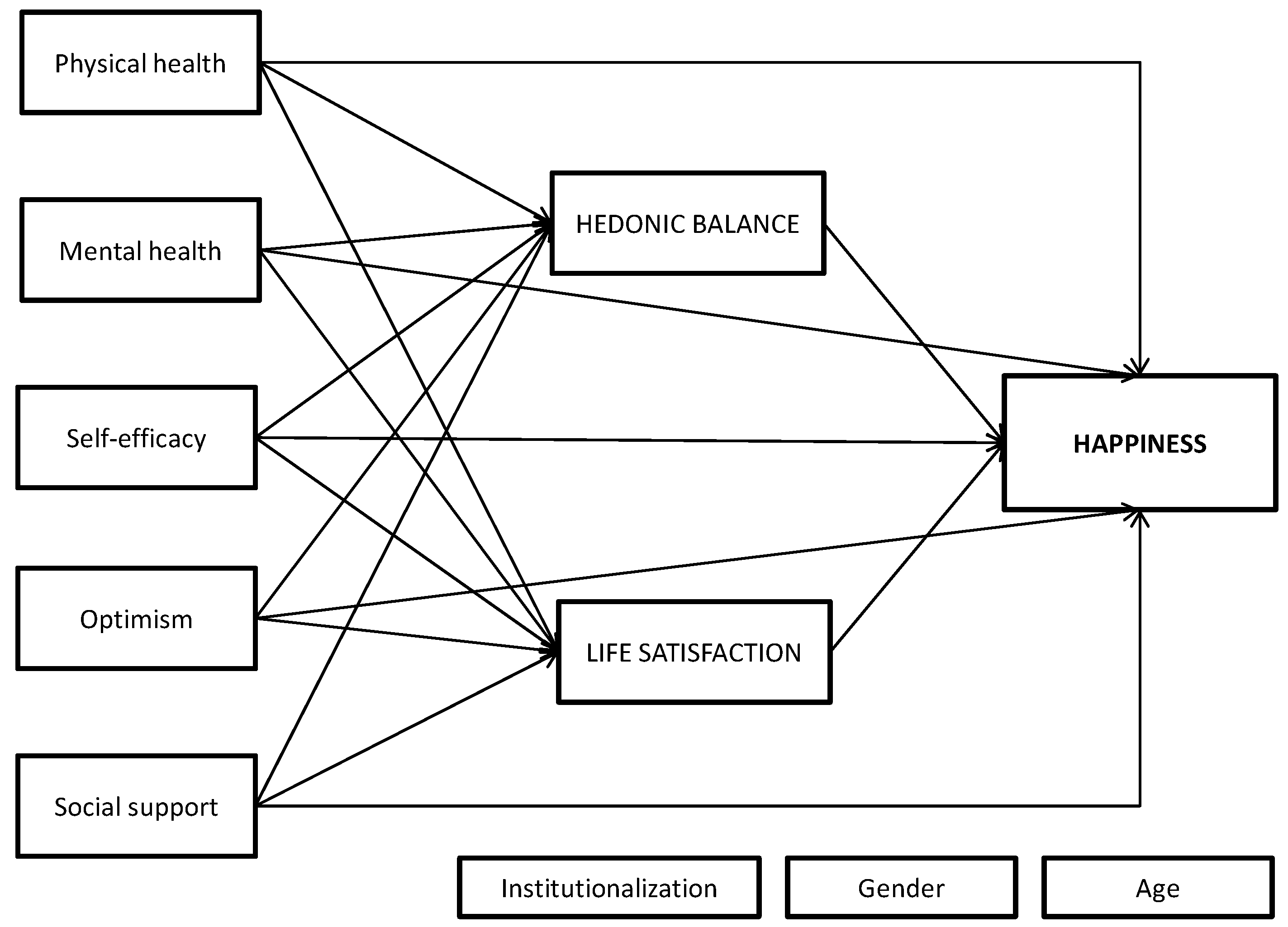
2.3. Study Design, Procedures, and Analytical Plan
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cosco, T.D.; Prina, A.M.; Perales, J.; Stephan, B.C.; Brayne, C. Operational definitions of successful aging: A systematic review. Int. Psychogeriatr. 2014, 26, 373. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Dieppe, P. What is successful ageing and who should define it? Br. Med. J. 2005, 331, 1548–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carver, L.F.; Buchanan, D. Successful aging: Considering non-biomedical constructs. Clinical Interventions in Aging. Clin. Interv. Aging 2016, 11, 1623–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teater, B.; Chonody, J.M. How do older adults define successful aging? A scoping review. Int. J. Aging Hum. Dev. 2019, 0091415019871207. [Google Scholar] [CrossRef] [PubMed]
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health 2013, 13, 119–139. [Google Scholar] [CrossRef] [Green Version]
- Sin, N.L.; Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. J. Clin. Psychol. Sess. 2010, 65, 467–487. [Google Scholar] [CrossRef] [Green Version]
- Ho, H.C.; Yeung, D.Y.; Kwok, S.Y. Development and evaluation of the positive psychology intervention for older adults. J. Posit. Psychol. 2014, 9, 187–197. [Google Scholar] [CrossRef]
- Proyer, R.T.; Gander, F.; Wellenzohn, S.; Ruch, W. Positive psychology interventions in people aged 50–79 years: Long-term effects of placebo-controlled online interventions on well-being and depression. Aging Ment. Health 2014, 18, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Sutipan, P.; Intarakamhang, U.; Macaskill, A. The impact of positive psychological interventions on well-being in healthy elderly people. J. Happiness Stud. 2017, 18, 269–291. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being. Psychol. Bull. 1984, 95, 542–575. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.; Lucas, R.; Smith, H. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Diener, E. Myths in the science of happiness, and directions for future research. In The Science of Subjective Well-Being; Eid, M., Larsen, R.J., Eds.; Guilford: New York, NY, USA, 2008; pp. 493–514. [Google Scholar]
- Bradburn, N.M. The Structure of Psychological Well-Being; Aldine: Chicago, IL, USA, 1969. [Google Scholar]
- Diener, E.; Sandvik, E.; Pavot, W. Happiness is the frequency, not the intensity, of positive versus negative affect. In Assessing Well-being: The Collected Works of Ed Diener; Diener, E., Ed.; Springer: New York, NY, USA, 2009; pp. 213–231. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Veenhoven, R. Healthy happiness: Effects of happiness on physical health and the consequences for preventive health care. J. Happiness Stud. 2008, 9, 449–469. [Google Scholar] [CrossRef] [Green Version]
- Diener, E.; Lucas, R.E.; Oishi, S. Subjective well-being: The science of happiness and life satisfaction. In Handbook of Positive Psychology; Snyder, C., Lopez, S., Eds.; Oxford University Press: New York, NY, USA, 2002; pp. 63–73. [Google Scholar]
- Baird, B.M.; Lucas, R.E.; Donnellan, M.B. Life satisfaction across the lifespan: Findings from two nationally representative panel studies. Soc. Indic. Res. 2010, 99, 183–203. [Google Scholar] [CrossRef] [Green Version]
- Bohórquez, M.R.; Lorenzo, M.; García, A.J. Felicidad y actividad física en personas mayores. Escr. de Psicol. 2013, 6, 6–12. [Google Scholar] [CrossRef]
- Godoy-Izquierdo, D.; Lara, R.; Vázquez, M.L.; Araque, F.; Godoy, J.F. Correlates of happiness among older Spanish institutionalised and non-institutionalised adults. J. Happiness Stud. 2013, 14, 389–414. [Google Scholar] [CrossRef]
- Hellevik, O. The U-shaped age-happiness relationship: Real or methodological artifact? Qual. Quant. 2017, 51, 177–197. [Google Scholar] [CrossRef]
- Holahan, C.K.; Holahan, C.J.; Velasquez, K.E.; North, R.J. Longitudinal change in happiness during aging: The predictive role of positive expectancies. Int. J. Aging Hum. Dev. 2008, 66, 229–241. [Google Scholar] [CrossRef]
- Márquez-González, M.; de Trocóniz, M.I.F.; Cerrato, I.M.; Baltar, A.L. Emotional experience and regulation across the adult lifespan: Comparative analysis in three age groups. Psicothema 2008, 20, 616–622. [Google Scholar]
- Lara, R.; Godoy-Izquierdo, D.; Vázquez-Pérez, M.L.; Padial, A.; Araque-Serrano, F.; Godoy, J.F. Multidimensional psychosocial profiles in the elderly and happiness: A cluster-based identification. Aging Ment. Health 2014, 18, 489–503. [Google Scholar] [CrossRef]
- Rey, L.; Extremera, N.; Sánchez-Álvarez, N. Clarifying the links between perceived emotional intelligence and well-being in older people: Pathways through perceived social support from family and friends. Appl. Res. Qual. Life 2019, 14, 221–235. [Google Scholar] [CrossRef]
- Fancourt, D.; Steptoe, A. Community group membership and multidimensional subjective well-being in older age. J. Epidemiol. Community Health 2018, 72, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco-Molina, M.; Pinazo-Hernandis, S.; Manuel-Tomás, J. Subjective well-being key elements of successful aging: A study with lifelong learners older adults from Costa Rica and Spain. Arch. Gerontol. Geriatr. 2019, 85, 1–8. [Google Scholar] [CrossRef]
- Buz, J.; Perez-Arechaederra, D. Psychometric properties and measurement invariance of the Spanish version of the 11-item De Jong Gierveld loneliness scale. Int. Psychogeriatr. 2014, 26, 1553–1564. [Google Scholar] [CrossRef]
- Kroemeke, A.; Gruszczynska, E. Well-being and institutional care in older adults: Cross-sectional and time effects of provided and received support. PLoS ONE 2016, 11, e0161328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luchesi, B.M.; de Oliveira, N.A.; de Morais, D.; de Paula Pessoa, R.M.; Pavarini, S.C.I.; Chagas, M.H.N. Factors associated with happiness in the elderly persons living in the community. Arch. Gerontol. Geriatr. 2018, 74, 83–87. [Google Scholar] [CrossRef]
- Matud, M.P.; García, M.C.; Fortes, D. Relevance of gender and social support in self-rated health and life satisfaction in elderly Spanish people. Int. J. Environ. Res. Public Health 2019, 16, 2725. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Blázquez, C.; Joao-Forjaz, M.; Prieto-Flores, M.E.; Rojo-Pérez, F.; Fernández-Mayoralas, G.; Martínez-Martín, P. Spanish Research Group Quality Life and Ageing. Health status and well-being of older adults living in the community and in residential care settings: Are differences influenced by age? Aging Ment. Health 2012, 16, 884–891. [Google Scholar] [CrossRef]
- Sancho, P.; Tomás, J.M.; Oliver, A.; Galiana, L.; Gutiérrez, M. Predicting life satisfaction in Spanish adults of advancing age attending university educational programs. J. Happiness Stud. 2020, 21, 271–287. [Google Scholar] [CrossRef]
- Siedlecki, K.L.; Salthouse, T.A.; Oishi, S.; Jeswani, S. The relationship between social support and subjective well-being across age. Soc. Indic. Res. 2014, 117, 561–576. [Google Scholar] [CrossRef] [Green Version]
- Huxhold, O.; Fiori, K.L.; Windsor, T.D. The dynamic interplay of social network characteristics, subjective well-being, and health: The costs and benefits of socio-emotional selectivity. Psychol. Aging 2013, 28, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Huxhold, O.; Miche, M.; Schüz, B. Benefits of having friends in older ages: Differential effects of informal social activities on well-being in middle-aged and older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2013, 69, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Pauly, T.; Lay, J.C.; Scott, S.B.; Hoppmann, C.A. Social relationship quality buffers negative affective correlates of everyday solitude in an adult lifespan and an older adult sample. Psychol. Aging 2018, 33, 728–738. [Google Scholar] [CrossRef] [PubMed]
- da Dias Rocha, L.F.; Oliveira, E.; da Mota, M. Relationship between social support and subjective well-being in older people: Systematic review. Rev. Bras. Em Promoção da Saúde 2017, 30, 1–13. [Google Scholar] [CrossRef]
- Mhaske, R. Happiness and aging. J. Psychosoc. Res. 2017, 12, 71–79. [Google Scholar]
- Freedman, V.A.; Carr, D.; Cornman, J.C.; Lucas, R. Aging, mobility impairments and subjective wellbeing. Disabil. Health J. 2017, 10, 525–531. [Google Scholar] [CrossRef]
- Gana, K.; Bailly, N.; Saada, Y.; Joulain, M.; Trouillet, R.; Hervé, C.; Alaphilippe, D. Relationship between life satisfaction and physical health in older adults: A longitudinal test of cross-lagged and simultaneous effects. Health Psychol. 2013, 32, 896–904. [Google Scholar] [CrossRef]
- Lee, S. An exploration of antecedents of positive affect among the elderly: A cross-sectional study. Eur. J. Public Health 2016, 26, 187–191. [Google Scholar] [CrossRef] [Green Version]
- Meléndez, J.C.; Tomás, J.M.; Oliver, A.; Navarro, E. Psychological and physical dimensions explaining life satisfaction among the elderly: A structural model examination. Archives Gerontol. Geriatr. 2009, 48, 291–295. [Google Scholar] [CrossRef]
- Olson, E.A.; Fanning, J.T.; Awick, E.A.; Chung, H.D.; McAuley, E. Differential trajectories of well-being in older adult women: The role of optimism. Appl. Psychol. Health Well-Being 2014, 6, 362–380. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Fernández, E.; Ortega-Martínez, A.R.; Calero-García, M.J. Optimism as a mediator between resilience and affective states in older adults. Estud. Psicol. 2018, 39, 267–285. [Google Scholar] [CrossRef]
- Parra-Rizo, M.A.; Sanchís-Soler, G. Satisfaction with life, subjective well-being and functional skills in active older adults based on their level of physical activity practice. Int. J. Environ. Res. Public Health 2020, 17, 1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliot, A.J.; Mooney, C.J.; Infurna, F.J.; Chapman, B.P. Perceived control and frailty: The role of affect and perceived health. Psychol. Aging 2018, 33, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Eryilmaz, A.; Atak, H. A model of happiness for older adults living with their families. Noropsikiyatri Ars. Arch. Neuropsychiatry 2011, 48, 227–233. [Google Scholar] [CrossRef]
- Finkenzeller, T.; Pötzelsberger, B.; Kösters, A.; Würth, S.; Amesberger, G.; Dela, F.; Müller, E. Aging in high functioning elderly persons: Study design and analyses of behavioral and psychological factors. Scand. J. Med. Sci. Sports 2019, 29, 7–16. [Google Scholar] [CrossRef] [Green Version]
- de Quadros-Wander, S.; McGillivray, J.; Broadbent, J. The influence of perceived control on subjective wellbeing in later life. Soc. Indic. Res. 2014, 115, 999–1010. [Google Scholar] [CrossRef]
- Gana, K.; Klein, V.; Saada, Y.; Trouillet, R. Relationship between time perspective and life satisfaction among older adults: Test of mediating effect of self-efficacy. Eur. Rev. Appl. Psychol. Rev. Eur. de Psychol. Appl. 2013, 63, 49–57. [Google Scholar] [CrossRef]
- Jafari, A.; Hesampour, F. Predicting life satisfaction based on spiritual intelligence and psychological capital in older people. Salmand Iran. J. Ageing 2017, 12, 90–103. [Google Scholar] [CrossRef] [Green Version]
- Wiesmann, U.; Hannich, H.J. A salutogenic analysis of the well-being paradox in older age. J. Happiness Stud. 2014, 15, 339–355. [Google Scholar] [CrossRef]
- Ferguson, S.J.; Goodwin, A.D. Optimism and well-being in older adults: The mediating role of social support and perceived control. Int. J. Aging Hum. Dev. 2010, 71, 43–68. [Google Scholar] [CrossRef]
- González, V.; Extremera, N. Daily life activities as mediators of the relationship between personality variables and subjective well-being among older adults. Personal. Individ. Differ. 2010, 49, 124–129. [Google Scholar] [CrossRef]
- Busseri, M.A. Examining the structure of subjective well-being through meta-analysis of the associations among positive affect, negative affect, and life satisfaction. Personal. Individ. Differ. 2018, 122, 68–71. [Google Scholar] [CrossRef]
- Schimmack, U. The structure of subjective well-being. In The Science of Subjective Well-Being; Eid, M., Larsen, R.J., Eds.; Guilford: New York, NY, USA, 2008; pp. 97–123. [Google Scholar]
- Bujang, M.A.; Baharum, N. Sample size guideline for correlation analysis. World J. Soc. Sci. Res. 2016, 3, 37–46. [Google Scholar] [CrossRef]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.; Newman, T.B. Designing Clinical Research: An Epidemiologic Approach, 4th ed.; Lippincott Williams Wilkins: Philadelphia, PA, USA, 2013; p. 73. [Google Scholar]
- Warr, P.; Barter, J.; Brownbridge, G. On the independence of positive and negative affect. J. Personal. Soc. Psychol. 1983, 44, 644–651. [Google Scholar] [CrossRef]
- Godoy-Izquierdo, D.; Martínez, A. La “Escala de Balance Afectivo”: Propiedades psicométricas de un instrumento para la medida del afecto positivo y negativo en población española. Clínica y Salud 2008, 19, 157–189. [Google Scholar]
- Stock, W.A.; Okun, M.A.; Benito, J.A.G. Subjective well-being measures: Reliability and validity among Spanish elders. Int. J. Aging Hum. Dev. 1994, 38, 221–235. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E. Review of the Satisfaction with Life Scale. Psychol. Assess. 1993, 5, 164–172. [Google Scholar] [CrossRef]
- Vázquez, C.; Duque, A.; Hervás, G. Satisfaction with life scale in a representative sample of Spanish adults: Validation and normative data. Span. J. Psychol. 2013, 16, e82. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Alonso, J.; Regidor, E.; Barrio, G.; Prieto, L.; Rodríguez, C.; de la Fuente, L. Valores poblacionales de referencia de la versión española del Cuestionario de Salud SF-36. Med. Clínica Barc. 1998, 111, 410–416. [Google Scholar] [CrossRef]
- Vilagut, G.; Valderas, J.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretation of SF-36 and SF-12 questionnaires in Spain: Physical and mental components. Med. Clínica 2008, 130, 726–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunillera, O.; Tresserras, R.; Rajmil, L.; Vilagut, G.; Brugulat, P.; Herdman, M.; Mompart, A.; Medina, A.; Pardo, Y.; Alonso, J.; et al. Discriminative capacity of the EQ-5D, SF-6D, and SF-12 as measures of health status in population health survey. Qual. Life Res. 2010, 19, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Gandek, B.; Ware, J.; Aaronson, N.; Apolone, G.; Bjorner, J.; Brazier, J.; Bullinger, M.; Kaasa, S.; Leplège, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health survey in nine countries: Results from the IQOLA Project. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- Sherer, M.; Adams, C.H. Construct validation of the Self-Efficacy Scale. Psychol. Rep. 1983, 53, 899–902. [Google Scholar] [CrossRef]
- Montorio, I.; Izal, M.; Sánchez, M.; Losada, A. Dependencia y autonomía funcional en la vejez. La profecía se autocumple. Rev. Multidiscip. de Gerontol. 2002, 12, 61–71. [Google Scholar]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J. Personal. Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef]
- Ferrando, P.; Chico, E.; Tous, J. Propiedades psicométricas del test de optimismo Life Orientation Test. Psicothema 2002, 14, 673–680. [Google Scholar]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Remor, E. Fiabilidad y validez de la versión española del cuestionario MOS y SF-30 para evaluar la calidad de vida de personas infectadas por el VIH. Rev. de Atención Primaria 2003, 32, 15–22. [Google Scholar] [CrossRef]
- Revilla, L.; Luna del Castillo, J.; Bailon-Muñoz, E.; Medina-Moruno, I. Validación del cuestionario MOS de apoyo social en Atención Primaria. Med. de Fam. 2005, 6, 10–18. [Google Scholar] [CrossRef]
- Arbuckle, J.L. Computer Program. In Amos (Version 22.0); IBM-SPSS: Chicago, IL, USA, 2013. [Google Scholar]
- Diener, E.; Fujita, F. Resources, personal strivings, and subjective well-being: A nomothetic and idiographic approach. J. Personal. Soc. Psychol. 1995, 68, 926–935. [Google Scholar] [CrossRef]
- Lucas, R.E.; Diener, E.; Suh, E. Discriminant validity of well-being measures. J. Personal. Soc. Psychol. 1996, 71, 616–628. [Google Scholar] [CrossRef]
- Diener, E.; Larsen, R.J. The subjective experience of emotional well-being. In Handbook of Emotions; Lewis, M., Haviland, J.M., Eds.; Guilford Press: New York, NY, USA, 1993; pp. 405–415. [Google Scholar]
- Busseri, M.A. Toward a resolution of the tripartite structure of subjective well-being. J. Personal. 2015, 83, 413–428. [Google Scholar] [CrossRef] [PubMed]
- Metler, S.; Busseri, M.A. Further evaluation of the tripartite structure of subjective well-being: Evidence from longitudinal and experimental studies. J. Personal. 2017, 85, 192–206. [Google Scholar] [CrossRef]
- Kline, R. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Salces-Cubero, M.I.; Ramírez-Fernández, E.R.; Ortega-Martínez, A. Strengths in older adults: Differential effect of savoring, gratitude and optimism on well-being. Aging Ment. Health 2019, 23, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P.; Krull, J.L.; Lockwood, C.W. Equivalence of the mediation, confounding and suppression effect. Prev. Sci. 2000, 1, 173–181. [Google Scholar] [CrossRef]
- Brooke, M.; Alice, E.; Musikanski, L. Life satisfaction, affect, and belonging in older adults. Appl. Res. Qual. Life 2020. [Google Scholar] [CrossRef]
- United Nations. World Population Ageing. Available online: www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2017_Highlights.pdf (accessed on 3 February 2020).
- World Health Organization. Ageing and health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 3 February 2020).
- Luger, T.; Cotter, K.A.; Sherman, A.M. It’s all in how you view it: Pessimism, social relations, and life satisfaction in older adults with osteoarthritis. Aging Ment. Health 2009, 13, 635–647. [Google Scholar] [CrossRef] [Green Version]
- Carver, C.S.; Scheier, M.F.; Segerstrom, S.C. Optimism. Clin. Psychol. Rev. 2010, 30, 879–889. [Google Scholar] [CrossRef] [Green Version]
- Klassen, R.M. Optimism and realism: A review of self-efficacy from a cross-cultural perspective. Int. J. Psychol. 2004, 39, 205–230. [Google Scholar] [CrossRef]
- Burleson, B.R. The experience and effects of emotional support: What the study of cultural and gender differences can tell us about close relationships, emotion, and interpersonal communication. Pers. Relatsh. 2003, 10, 1–23. [Google Scholar] [CrossRef]
- Diener, E.; Oishi, S.; Lucas, R.E. Personality, culture, and subjective well-being: Emotional and cognitive evaluations of life. Annu. Rev. Psychol. 2003, 54, 403–425. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Biswas-Diener, R. The happiest places on earth: Culture and well-being. In Happiness: Unlocking the Mysteries of Psychological Wealth; Blackwell: Malden, MA, USA, 2008; pp. 127–144. [Google Scholar]
- Diener, E.; Ryan, K. Subjective well-being: A general overview. S. Afr. J. Psychol. 2009, 39, 391–406. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Condition | % | |
|---|---|---|
| Marital Status | Single with no history of a regular partner | 1.9 |
| Married or in a stable relationship | 56.5 | |
| No current partner but a history of a stable or marital relationship | 41.6 | |
| Education Level | No education | 20.8 |
| Primary | 46.1 | |
| Secondary | 16.9 | |
| Vocational training | 7.1 | |
| University | 9.1 | |
| Employment Status | Working | 1.9 |
| Unemployed | 2.6 | |
| Housework | 20.8 | |
| Retired | 74.7 | |
| Monthly Family Income | <1000 € | 47.6 |
| 1000–2000 € | 46.2 | |
| 2000–3000 € | 4.2 | |
| >3000 € | 2.1 | |
| Number of Children | 0 | 10.4 |
| 1 | 3.2 | |
| 2 | 23.4 | |
| 3 | 31.8 | |
| ≥4 | 31.1 | |
| Chronic Disease (Perceived health on a 0–10 points scale: M = 6.25, SD = 1.89) | Yes, of which (more frequent) | 74.7 |
| Cardiovascular diseases including coronary and vascular diseases, hypertension and high cholesterol | 47.9 | |
| Bone and rheumatic diseases including osteoporosis, osteoarthritis, and rheumatoid arthritis | 27.1 | |
| Diabetes | 6.9 | |
| Hyperthyroidism | 4.2 | |
| Neurologic diseases including multiple sclerosis, Parkinson, and limb paralysis | 3.5 | |
| Respiratory diseases including asthma and chronic bronchitis | 2.8 | |
| Limb amputation | 2.8 | |
| Cancer, including prostate diseases | 2.8 | |
| Sensorial deficit | 2.1 | |
| Any Kind of Therapy | Yes, of which (more frequent) | 76.6 |
| Cardiovascular treatments | 26.5 | |
| Non-steroidal anti-inflammatory drugs | 19.7 | |
| Calcium and vitamins supplements | 6.8 | |
| Diabetes treatments | 5.1 | |
| Hyperthyroidism treatments | 4.3 | |
| Anxiolytics | 3.4 | |
| Min | Max | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. SF12PCS | 16.66 | 60.30 | 39.08 | 10.86 | - | 0.11 | 0.43 ** | 0.06 | 0.18 * | 0.35 ** | −0.46 ** | 0.48 ** | 0.24 ** | 0.29 ** |
| 2. SF12MCS | 20.73 | 64.11 | 46.59 | 9.93 | - | 0.26 ** | 0.05 | 0.14 † | 0.36 ** | −0.58 ** | 0.55 ** | 0.33 ** | 0.36 ** | |
| 3. Self-efficacy | 46 | 99 | 78.67 | 11.32 | - | 0.17 * | 0.29 ** | 0.44 ** | −0.39 ** | 0.49 ** | 0.17 * | 0.23 ** | ||
| 4. Optimism | 10 | 29 | 19.83 | 2.76 | - | –0.10 | 0.13 | −0.03 | 0.10 | 0.13 | 0.01 | |||
| 5. Social support | 37 | 95 | 72.56 | 16.81 | - | 0.48 ** | −0.34 ** | 0.49 ** | 0.32 ** | 0.34 ** | ||||
| 6. Positive affect | 9 | 27 | 16.87 | 3.92 | - | −0.43 ** | 0.85 ** | 0.29 ** | 0.40 ** | |||||
| 7. Negative affect | 9 | 26 | 15.88 | 3.80 | - | −0.84 ** | −0.51 ** | −0.40 ** | ||||||
| 8. Hedonic balance | −13 | 17 | 0.99 | 6.53 | - | 0.47 ** | 0.47 ** | |||||||
| 9. Life satisfaction | 8 | 35 | 25.88 | 5.61 | - | 0.45 ** | ||||||||
| 10. Current happiness | 0 | 10 | 6.59 | 1.90 | - |
| Path | Stand. Estimate | S.E. | C.R. | p | ||
|---|---|---|---|---|---|---|
| SF12PCS | - | Hedonic balance | 0.32 | 0.040 | 2.176 | 0.000 ** |
| SF12MCS | - | Hedonic balance | 0.46 | 0.042 | 4.296 | 0.000 ** |
| Self-efficacy | - | Hedonic balance | 0.13 | 0.042 | −1.107 | 0.025 * |
| Optimism | - | Hedonic balance | 0.10 | 0.145 | 2.378 | 0.068 † |
| Social support | - | Hedonic balance | 0.33 | 0.025 | 3.792 | 0.000 ** |
| SF12PCS | - | Life satisfaction | 0.17 | 0.033 | 5.758 | 0.030 * |
| SF12MCS | - | Life satisfaction | 0.32 | 0.034 | 8.643 | 0.000 ** |
| Self-efficacy | - | Life satisfaction | −0.09 | 0.034 | 2.240 | 0.268 |
| Optimism | - | Life satisfaction | 0.17 | 0.119 | 1.822 | 0.017 * |
| Social support | - | Life satisfaction | 0.28 | 0.020 | 6.238 | 0.000 ** |
| Hedonic balance | - | Happiness | 0.33 | 0.023 | 4.220 | 0.000 ** |
| Life satisfaction | - | Happiness | 0.29 | 0.026 | 3.815 | 0.000 ** |
| Self-efficacy | - | SF12PCS | 0.39 | 9.791 | 4.716 | 0.000 ** |
| Self-efficacy | - | SF12MCS | 0.24 | 8.334 | 3.130 | 0.002 ** |
| Self-efficacy | - | Optimism | 0.16 | 2.174 | 2.289 | 0.022 * |
| Self-efficacy | - | Social support | 0.26 | 14.185 | 3.384 | 0.000 ** |
| Social support | - | SF12MCS | 0.19 | 13.651 | 2.305 | 0.021 * |
| e1 | - | e2 | 0.21 | 1.605 | 2.514 | 0.012 * |
| Predictor | Stand. Estimate | 95% CI Lower Bound | 95% CI Upper Bound | p |
|---|---|---|---|---|
| SF12PCS | 0.16 | 0.088 | 0.229 | 0.004 ** |
| SF12MCS | 0.24 | 0.157 | 0.326 | 0.002 ** |
| Self-efficacy | 0.02 | −0.079 | 0.080 | 0.770 |
| Optimism | 0.08 | 0.024 | 0.153 | 0.007 ** |
| Social support | 0.19 | 0.109 | 0.269 | 0.003 ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lara, R.; Vázquez, M.L.; Ogallar, A.; Godoy-Izquierdo, D. Psychosocial Resources for Hedonic Balance, Life Satisfaction and Happiness in the Elderly: A Path Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5684. https://doi.org/10.3390/ijerph17165684
Lara R, Vázquez ML, Ogallar A, Godoy-Izquierdo D. Psychosocial Resources for Hedonic Balance, Life Satisfaction and Happiness in the Elderly: A Path Analysis. International Journal of Environmental Research and Public Health. 2020; 17(16):5684. https://doi.org/10.3390/ijerph17165684
Chicago/Turabian StyleLara, Raquel, Mᵃ Luisa Vázquez, Adelaida Ogallar, and Débora Godoy-Izquierdo. 2020. "Psychosocial Resources for Hedonic Balance, Life Satisfaction and Happiness in the Elderly: A Path Analysis" International Journal of Environmental Research and Public Health 17, no. 16: 5684. https://doi.org/10.3390/ijerph17165684
APA StyleLara, R., Vázquez, M. L., Ogallar, A., & Godoy-Izquierdo, D. (2020). Psychosocial Resources for Hedonic Balance, Life Satisfaction and Happiness in the Elderly: A Path Analysis. International Journal of Environmental Research and Public Health, 17(16), 5684. https://doi.org/10.3390/ijerph17165684