Oral Health Inequalities and the Corporate Determinants of Health: A Commentary




{kind=link}
Abstract
:1. Introduction
2. What Are Corporate Determinants of Health?
3. What Is Power?
4. What Are Oral Health Inequalities?
5. Industries That Directly Impact Oral Health Inequalities
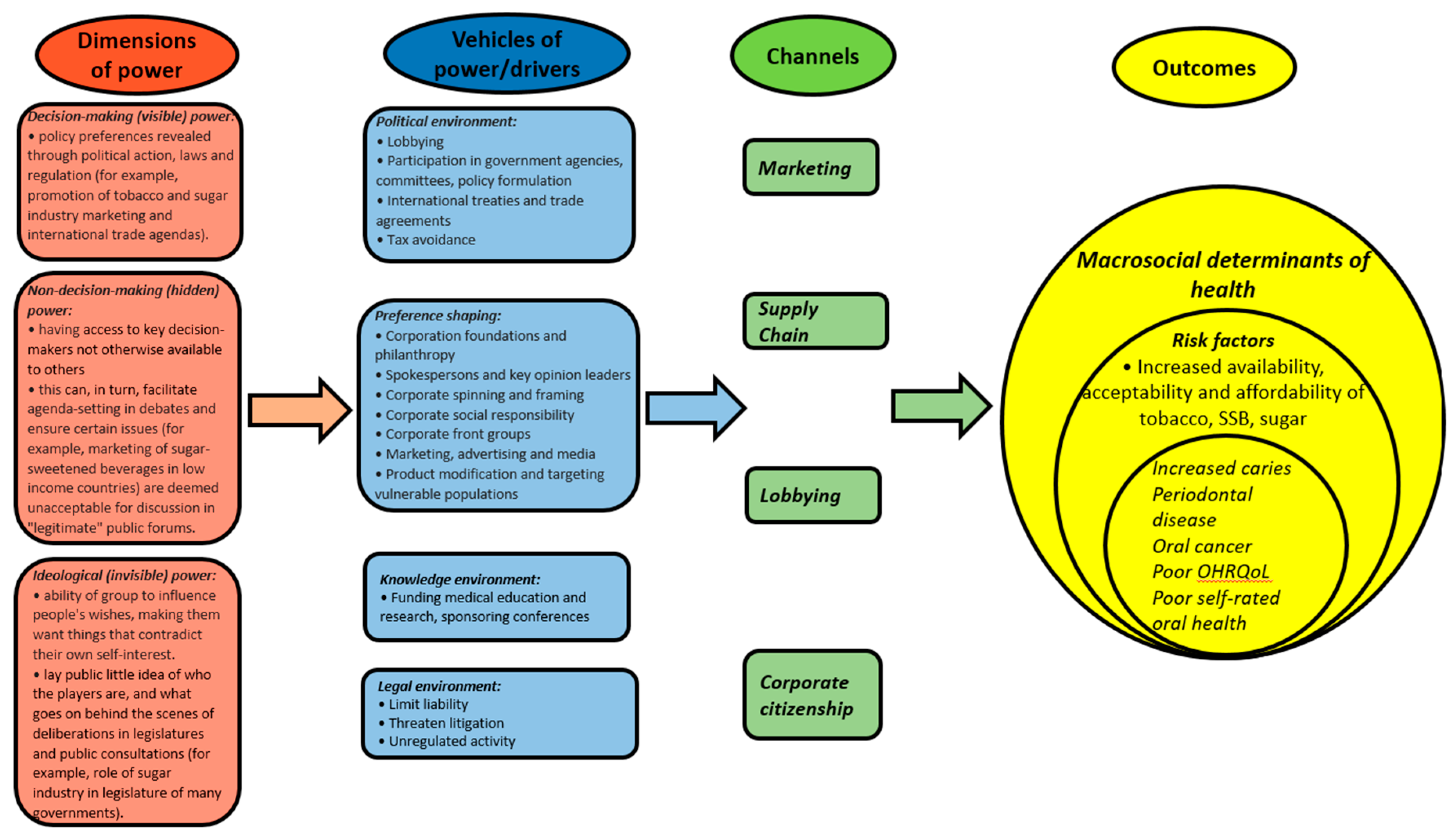
6. A Conceptual Framework of the Corporate Determinants of Health and Oral Health Inequalities
7. How Can the Dental Profession Counter the Corporate Determinants of Oral Health?
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hastings, G. Why corporate power is a public health priority. BMJ 2012, 345, 5124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. Lancet NCD Action Group. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Kenworthy, N.; MacKenzie, R.; Lee, K. Case Studies on Corporations and Global Health Governance: Impacts, Influence and Accountability; Rowman and Littlefield International: London, UK, 2016. [Google Scholar]
- Kickbusch, I.; Allen, L.; Franz, C. The commercial determinants of health. Lancet Glob. Health 2016, 4, e895–e896. [Google Scholar] [CrossRef] [Green Version]
- West, R.; Marteau, T. Commentary on Casswell (2013): The commercial determinants of health. Addiction 2013, 108, 686–687. [Google Scholar] [CrossRef]
- Reid, J.R. A History of Mentholated Cigarettes ‘This Spud’s for You’Philip Morris, 1993. Available online: http://legacy.library.ucsf.edu/tid/nqf32e00 (accessed on 1 August 2020).
- Babor, T.F.; Robaina, K. Public health, academic medicine, and the alcohol industry’s corporate social responsibility activities. Am. J. Public Health 2013, 103, 206–214. [Google Scholar] [CrossRef]
- Taylor, A.J. Conditional Party Government and Campaign Contributions: Insights from the Tobacco and Alcoholic Beverage Industries. Am. J. Political Sci. 2003, 47, 293–304. [Google Scholar] [CrossRef]
- Alvarez, J. Sweetening the US Legislature: The remarkable success of the sugar lobby. Political Q. 2005, 76, 92–99. [Google Scholar] [CrossRef]
- McKee, M.; Stuckler, D. Revisiting the Corporate and Commercial Determinants of Health. Am. J. Public Health 2018, 108, 1167–1170. [Google Scholar] [CrossRef]
- Dahl, R.A. The concept of power. Behav. Sci. 1957, 2, 201–215. [Google Scholar] [CrossRef]
- Lukes, S. Power: A Radical View; Palgrave Macmillan: Basingstoke, UK, 1975. [Google Scholar]
- Hall, O.H. An Analysis of Power and its Role in the Decision-Making Process of the Formal Organization; Louisiana State University: Baton Rouge, LA, USA, 1964. [Google Scholar]
- Robinson, N. Learning from Lukes? The three Faces of Power and the European Union; European Consortium for Political Research: Nicosia, Cyprus, 2006. [Google Scholar]
- Dowding, K. Three-dimensional power: A discussion of Steven Lukes’ Power: A Radical View. Political Stud. 2006, 4, 136–145. [Google Scholar] [CrossRef]
- Hathaway, T. Lukes reloaded: An actor-centred three-dimensional power framework. Politics 2016, 36, 118–130. [Google Scholar] [CrossRef]
- Lang, T. Reshaping the food system for ecological public health. J. Hunger Environ. Nutr. 2009, 4, 315–335. [Google Scholar] [CrossRef] [PubMed]
- Leichter, H.M. Free to Be Foolish: Politics and Health Promotion in the United States and Great Britain; Princeton University Press: Princeton, NJ, USA, 1991. [Google Scholar]
- Crawford, R. You Are Dangerous to Your Health: The Ideology and Politics of Victim Blaming. Int. J. Health Serv. 1977, 7, 663–680. [Google Scholar] [CrossRef] [PubMed]
- Wigand, J.S. Cigarette testing methods, product design, and labelling: Time to clean up the “negative baggage”. Tob. Control 1998, 7, 336–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilens, M.; Page, B.I. Testing theories of American politics: Elites, interest groups and average citizens. Perspect. Politics 2014, 12, 564–581. [Google Scholar] [CrossRef] [Green Version]
- Kearns, C.E.; Bero, L.A. Conflicts of interest between the sugary food and beverage industry and dental research organisations: Time for reform. Lancet 2019, 394, 194–196. [Google Scholar] [CrossRef]
- Friel, S.; Gleeson, D.; Thow, A.M.; Labonte, R.; Stuckler, D.; Kay, A.; Snowdon, W. A new generation of trade policy: Potential risks to diet-related health from the trans pacific partnership agreement. Glob. Health 2013, 9, 46. [Google Scholar] [CrossRef] [Green Version]
- Mosley, L. Labor Rights and Multinational Production; Cambridge University Press: New York, NY, USA, 2010. [Google Scholar]
- Klasa, S.; Maxwell, W.F.; Ortiz-Molina, H. The strategic use of corporate cash holdings in collective bargaining with labor unions. J. Financ. Econ. 2009, 92, 421–442. [Google Scholar] [CrossRef]
- Whitehead, M.; Dahlgren, G. What can be done about inequalities in health? Lancet 1991, 338, 1059–1063. [Google Scholar] [CrossRef]
- Beal, J.F. Inequalities in health—It’s the poor wot gets the blame. Community Dent. Health 1998, 15, 229–230. [Google Scholar]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Whelton, H.P.; Spencer, A.J.; Do, L.G.; Rugg-Gunn, A.J. Fluoride Revolution and Dental Caries: Evolution of Policies for Global Use. J. Dent. Res. 2019, 98, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Jevdjevic, M.; Trescher, A.L.; Rovers, M.; Listl, S. The caries-related cost and effects of a tax on sugar-sweetened beverages. Public Health 2019, 169, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreño, C.C.; Celeste, R.K.; et al. Ending the neglect of global oral health: Time for radical action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Kearns, C.E.; Watt, R.G. Transnational corporations and oral health: Examples from the sugar industry. Community Dent. Health 2019, 36, 157–162. [Google Scholar] [PubMed]
- United Nations. Transforming our World: The 2030 Agenda for Sustainable Development; United Nations: Geneva, Switzerland, 2015. [Google Scholar]
- Kieny, M.P.; Bekedam, H.; Dovlo, D.; Fitzgerald, J.; Habicht, J.; Harrison, G.; Kluge, H.; Lin, V.; Menabde, N.; Mirza, Z.; et al. Strengthening health systems for universal health coverage and sustainable development. Bull. World Health Organ. 2017, 95, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, S.; Schrecker, T. The double burden of neoliberalism? Noncommunicable disease policies and the global political economy of risk. Health Place 2016, 39, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Wiist, W.H. Public health and the anticorporate movement: Rationale and recommendations. Am. J. Public Health 2006, 96, 1370–1375. [Google Scholar] [CrossRef]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamieson, L.; Gibson, B.; Thomson, W.M. Oral Health Inequalities and the Corporate Determinants of Health: A Commentary. Int. J. Environ. Res. Public Health 2020, 17, 6529. https://doi.org/10.3390/ijerph17186529
Jamieson L, Gibson B, Thomson WM. Oral Health Inequalities and the Corporate Determinants of Health: A Commentary. International Journal of Environmental Research and Public Health. 2020; 17(18):6529. https://doi.org/10.3390/ijerph17186529
Chicago/Turabian StyleJamieson, Lisa, Barry Gibson, and W. Murray Thomson. 2020. "Oral Health Inequalities and the Corporate Determinants of Health: A Commentary" International Journal of Environmental Research and Public Health 17, no. 18: 6529. https://doi.org/10.3390/ijerph17186529
APA StyleJamieson, L., Gibson, B., & Thomson, W. M. (2020). Oral Health Inequalities and the Corporate Determinants of Health: A Commentary. International Journal of Environmental Research and Public Health, 17(18), 6529. https://doi.org/10.3390/ijerph17186529