Application of Activity Trackers among Nursing Home Residents—A Pilot and Feasibility Study on Physical Activity Behavior, Usage Behavior, Acceptance, Usability and Motivational Impact



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Measures
2.3. Statistical Analysis
3. Results
3.1. Daily PA of Nursing Home Residents
3.1.1. Daily Steps
3.1.2. Daily Sedentary Behavior
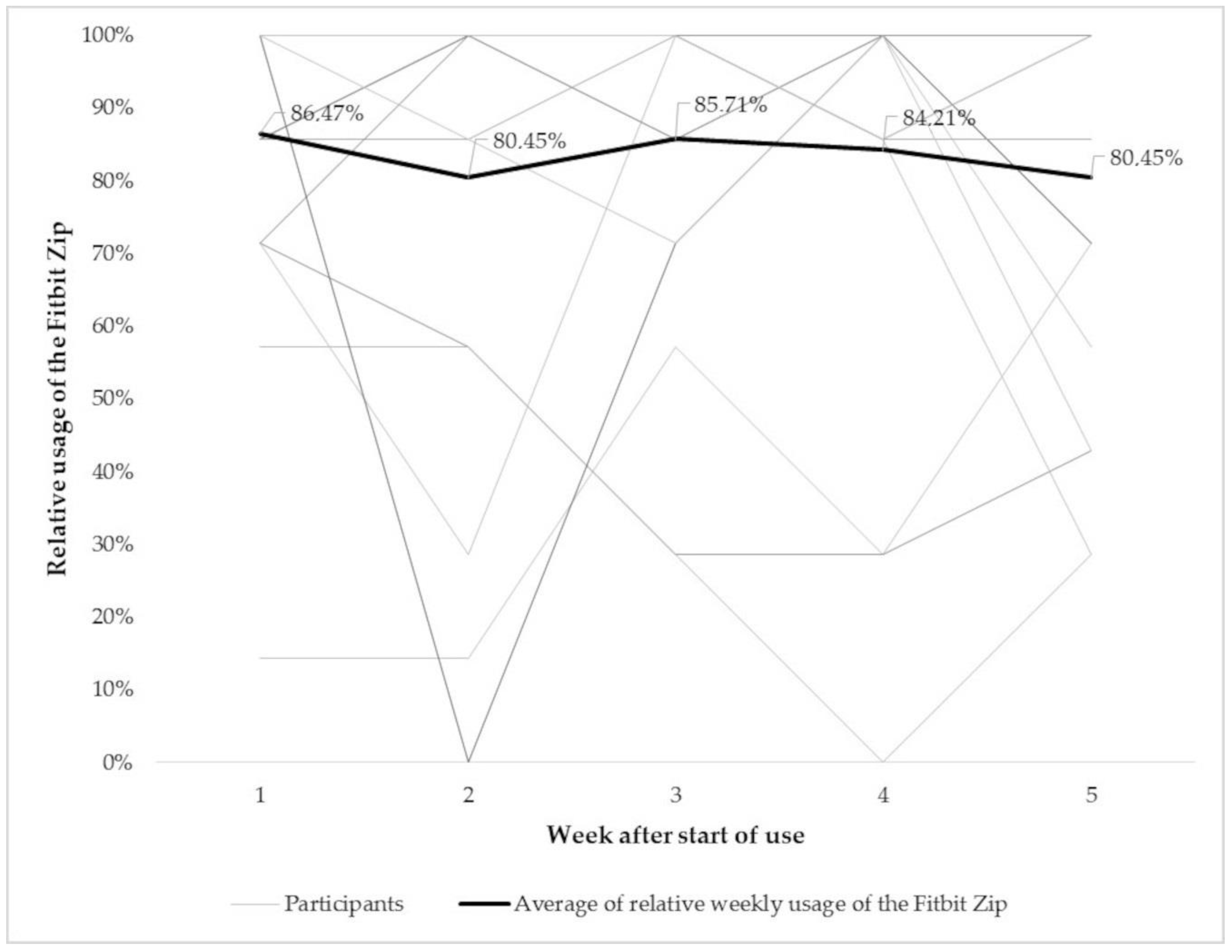
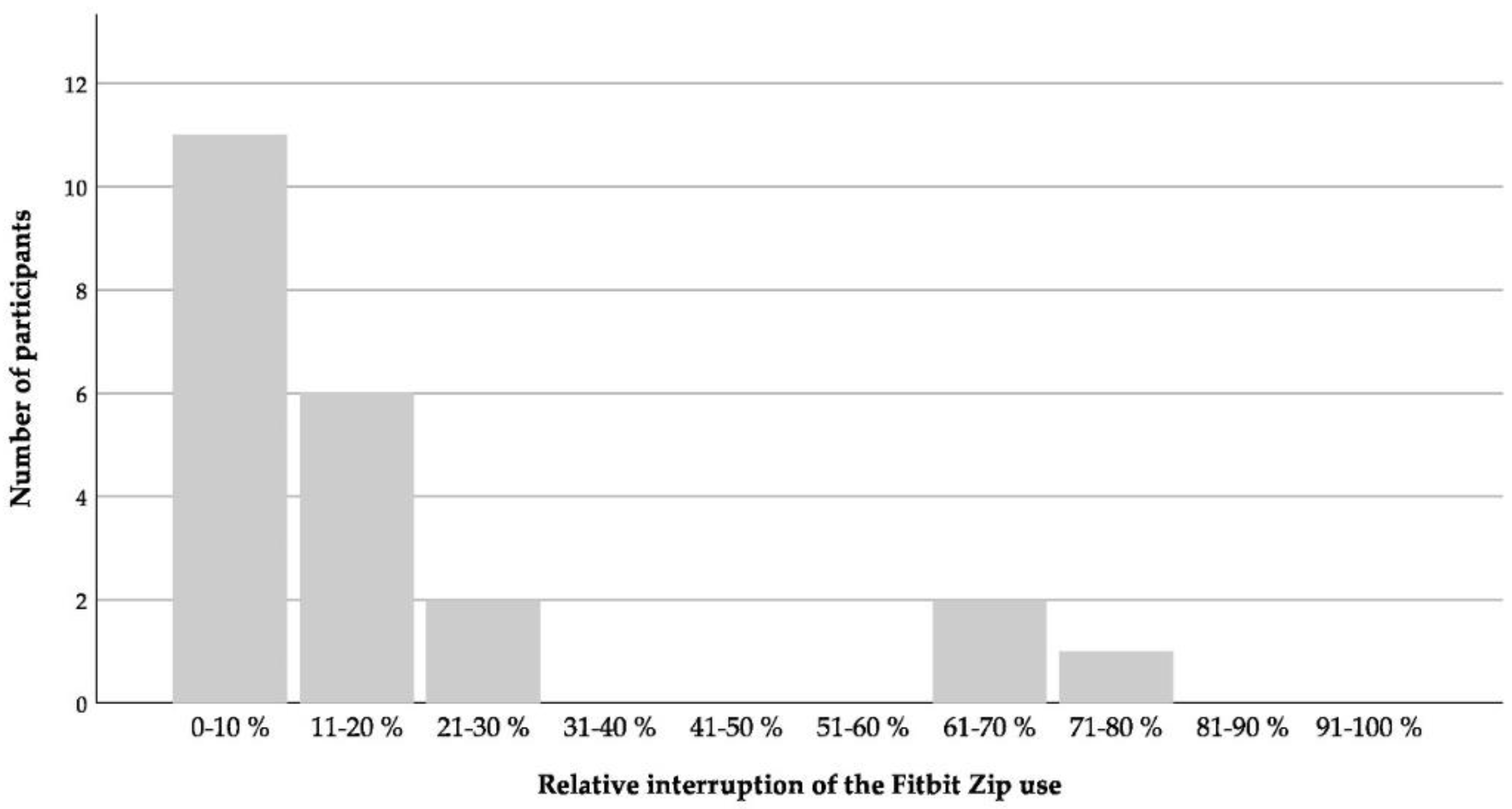
3.2. Usability, Acceptability and Motivational Capacity of Activity Trackers for Nursing Home Residents
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Commission. The 2018 Ageing Report: Economic and Budgetary Projections for the EU Member States (2016–2070). Ageing Rep. Jt. Rep. Prep. By Eur. Comm. Econ. Policy Comm. 2018. [Google Scholar] [CrossRef]
- Rothgang, H.; Müller, R.; Unger, R. Themenreport “Pflege 2030”. Was ist zu erwarten—Was ist zu tun; Bertelsmann Stiftung: Gütersloh, Germany, 2012. [Google Scholar]
- Acree, L.S.; Longfors, J.; Fjeldstad, A.S.; Fjeldstad, C.; Schank, B.; Nickel, K.J.; Montgomery, P.S.; Gardner, A.W. Physical activity is related to quality of life in older adults. Health Qual. Life Out. 2006, 4, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J. Aging Res. 2013, 2013, 657508. [Google Scholar] [CrossRef] [Green Version]
- Blake, H.; Mo, P.; Malik, S.; Thomas, S. How effective are physical activity interventions for alleviating depressive symptoms in older people? A systematic review. Clin. Rehabil. 2009, 23, 873–887. [Google Scholar] [CrossRef] [PubMed]
- Buman, M.P.; Hekler, E.B.; Haskell, W.L.; Pruitt, L.; Conway, T.L.; Cain, K.L.; Sallis, J.F.; Saelens, B.E.; Frank, L.D.; King, A.C. Objective light-intensity physical activity associations with rated health in older adults. Am. J. Epidemiol. 2010, 172, 1155–1165. [Google Scholar] [CrossRef] [Green Version]
- Talbot, L.A.; Gaines, J.M.; Huynh, T.N.; Metter, E.J. A home-based pedometer-driven walking program to increase physical activity in older adults with osteoarthritis of the knee: A preliminary study. J. Am. Geriatr. Soc. 2003, 51, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Voelcker-Rehage, C.; Godde, B.; Staudinger, U.M. Physical and motor fitness are both related to cognition in old age. Eur. J. Neurosci. 2010, 31, 167–176. [Google Scholar] [CrossRef]
- Blodgett, J.; Theou, O.; Kirkland, S.; Andreou, P.; Rockwood, K. The association between sedentary behaviour, moderate-vigorous physical activity and frailty in NHANES cohorts. Maturitas 2015, 80, 187–191. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Lee, I.-M. Sedentary behaviour and life expectancy in the USA: A cause-deleted life table analysis. BMJ Open 2012, 2. [Google Scholar] [CrossRef]
- Klenk, J.; Dallmeier, D.; Denkinger, M.D.; Rapp, K.; Koenig, W.; Rothenbacher, D. Objectively measured walking duration and sedentary behaviour and four-year mortality in older people. PLoS ONE 2016, 11, e0153779. [Google Scholar] [CrossRef]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J.H. Erratum to: Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2013, 56, 942–943. [Google Scholar] [CrossRef] [Green Version]
- Woolcott, J.C.; Ashe, M.C.; Miller, W.C.; Shi, P.; Marra, C.A. Does physical activity reduce seniors’ need for healthcare? A study of 24,281 Canadians. Br. J. Sports Med. 2010, 44, 902. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, C.E.; George, S.M.; Moore, S.C.; Bowles, H.R.; Blair, A.; Park, Y.; Troiano, R.P.; Hollenbeck, A.; Schatzkin, A. Amount of time spent in sedentary behaviors and cause-specific mortality in US adults. Am. J. Clin. Nutr. 2012, 95, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- MacRae, P.G.; Schnelle, J.F.; Simmons, S.F.; Ouslander, J.G. Physical activity levels of ambulatory nursing home residents. J. Aging Phys. Act. 1996, 4, 264–278. [Google Scholar] [CrossRef] [Green Version]
- Parry, S.; Chow, M.; Batchelor, F.; Fary, R.E. Physical activity and sedentary behaviour in a residential aged care facility. Australas. J. Ageing 2019, 38, E12–E18. [Google Scholar] [CrossRef] [Green Version]
- Reid, N.; Eakin, E.; Henwood, T.; Keogh, J.W.L.; Senior, H.E.; Gardiner, P.A.; Winkler, E.; Healy, G.N. Objectively measured activity patterns among adults in residential aged care. Int. J. Environ. Res. Public Health 2013, 10, 6783–6798. [Google Scholar] [CrossRef] [Green Version]
- Buckinx, F.; Mouton, A.; Reginster, J.Y.; Croisier, J.L.; Dardenne, N.; Beaudart, C.; Nelis, J.; Lambert, E.; Appelboom, G.; Bruyère, O. Relationship between ambulatory physical activity assessed by activity trackers and physical frailty among nursing home residents. Gait Posture 2017, 54, 56–61. [Google Scholar] [CrossRef]
- Cyarto, E.V.; Myers, A.M.; Tudor-Locke, C. Pedometer accuracy in nursing home and community-dwelling older adults. Med. Sci. Sports Exerc. 2004, 36, 205–209. [Google Scholar] [CrossRef]
- Tudor-Locke, C.E.; Myers, A.M. Challenges and opportunities for measuring physical activity in sedentary adults. Sports Med. 2001, 31, 91–100. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, J.F.; Saelens, B.E. Assessment of physical activity by self-report: Status, limitations, and future directions. Res. Q. Exerc. Sport 2000, 71 (Suppl. 2), 1–14. [Google Scholar] [CrossRef]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R. Using pedometers to increase physical activity and improve health: A systematic review. JAMA 2007, 298, 2296–2304. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, E.D.; Hartmann, A.; Uebelhart, D.; Murer, K.; Zijlstra, W. Wearable systems for monitoring mobility-related activities in older people: A systematic review. Clin. Rehabil. 2008, 22, 878–895. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S.; Stewart, J. Use of consumer wearable devices to promote physical activity: A review of health intervention studies. J. Environ. Health Sci. 2016, 2. [Google Scholar] [CrossRef]
- Bassett, D.R. Validity and reliability issues in objective monitoring of physical activity. Res. Q. Exerc. Sport 2000, 71 (Suppl. 2), 30–36. [Google Scholar] [CrossRef]
- Evenson, K.R.; Goto, M.M.; Furberg, R.D. Systematic review of the validity and reliability of consumer-wearable activity trackers. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 159. [Google Scholar] [CrossRef] [Green Version]
- Cohen-Mansfield, J.; Werner, P.; Culpepper, W.J.; Wolfson, M.; Bickel, E. Assessment of ambulatory behavior in nursing home residents who pace or wander: A comparison of four commercially available devices. Dement. Geriatr. Cogn. Disord. 1997, 8, 359–365. [Google Scholar] [CrossRef]
- Kawagoshi, A.; Kiyokawa, N.; Sugawara, K.; Takahashi, H.; Sakata, S.; Satake, M.; Shioya, T. Effects of low-intensity exercise and home-based pulmonary rehabilitation with pedometer feedback on physical activity in elderly patients with chronic obstructive pulmonary disease. Respir. Med. 2015, 109, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Snyder, A.; Colvin, B.; Gammack, J.K. Pedometer use increases daily steps and functional status in older adults. J. Am. Med. Dir. Assoc. 2011, 12, 590–594. [Google Scholar] [CrossRef]
- Steinert, A.; Wegel, S.; Steinhagen-Thiessen, E. Selbst-monitoring der physischen aktivität von senioren. HBScience 2015, 6, 115–120. [Google Scholar] [CrossRef]
- Fausset, C.B.; Mitzner, T.L.; Price, C.E.; Jones, B.D.; Fain, W.B.; Rogers, W.A. Older adults’ use of and attitudes toward activity monitoring technologies. Proc. Hum. Factors Erg. Soc. Annu. Meet. 2013, 57, 1683–1687. [Google Scholar] [CrossRef] [PubMed]
- Lyons, E.J.; Swartz, M.C.; Lewis, Z.H.; Martinez, E.; Jennings, K. Feasibility and acceptability of a wearable technology physical activity intervention with telephone counseling for mid-aged and older adults: A randomized controlled pilot trial. Jmir Mhealth Uhealth 2017, 5, e28. [Google Scholar] [CrossRef]
- Maher, C.; Ryan, J.; Ambrosi, C.; Edney, S. Users’ experiences of wearable activity trackers: A cross-sectional study. BMC Public Health 2017, 17, 880. [Google Scholar] [CrossRef] [Green Version]
- McMahon, S.K.; Lewis, B.; Oakes, M.; Guan, W.; Wyman, J.F.; Rothman, A.J. Older adults’ experiences using a commercially available monitor to self-track their physical activity. JMIR Mhealth Uhealth 2016, 4, e35. [Google Scholar] [CrossRef]
- Mercer, K.; Giangregorio, L.; Schneider, E.; Chilana, P.; Li, M.; Grindrod, K. Acceptance of commercially available wearable activity trackers among adults aged over 50 and with chronic illness: A mixed-methods evaluation. JMIR Mhealth Uhealth 2016, 4, e7. [Google Scholar] [CrossRef]
- Meyer, J.; Schnauber, J.; Heuten, W.; Wienbergen, H.; Hambrecht, R.; Appelrath, H.-J.; Boll, S. Exploring Longitudinal Use of Activity Trackers. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics (ICHI), Chicago, IL, USA, 4–7 October 2016; Fu, W.-T., Ed.; IEEE: Piscataway, NJ, USA, 2016; pp. 198–206. ISBN 978-1-5090-6117-4. [Google Scholar]
- Preusse, K.C.; Mitzner, T.L.; Fausset, C.B.; Rogers, W.A. Older adults’ acceptance of activity trackers. J. Appl. Gerontol. 2017, 36, 127–155. [Google Scholar] [CrossRef] [Green Version]
- Puri, A.; Kim, B.; Nguyen, O.; Stolee, P.; Tung, J.; Lee, J. User acceptance of wrist-worn activity trackers among community-dwelling older adults: Mixed method study. JMIR Mhealth Uhealth 2017, 5, e173. [Google Scholar] [CrossRef] [Green Version]
- Rasche, P.; Wille, M.; Theis, S.; Schaefer, K.; Schlick, C.M.; Mertens, A. Activity Tracker and Elderly. In The 15th IEEE International Conference on Computer and Information Technology (CIT 2015), the 14th IEEE International Conference on Ubiquitous Computing and Communications (IUCC 2015), the 13th IEEE International Conference on Dependable, Autonomic and Secure Computing (DASC 2015), the 13th IEEE International Conference on Pervasive Intelligence and Computing (PICom 2015), CIT/IUCC/DASC/PICom 2015: Proceedings: 26–28 October 2015, Liverpool, UK. 2015 IEEE International Conference on Computer and Information Technology; Ubiquitous Computing and Communications; Dependable, Autonomic and Secure Computing; Pervasive Intelligence and Computing (CIT/IUCC/DASC/PICOM), LIVERPOOL, UK, 26–28 October 2015; Wu, Y., Min, G., Georgalas, N., Eds.; IEEE: Piscataway, NJ, USA, 2015; pp. 1411–1416. ISBN 978-1-5090-0154-5. [Google Scholar]
- Cordes, T.; Bischoff, L.L.; Schoene, D.; Schott, N.; Voelcker-Rehage, C.; Meixner, C.; Appelles, L.-M.; Bebenek, M.; Berwinkel, A.; Hildebrand, C.; et al. A multicomponent exercise intervention to improve physical functioning, cognition and psychosocial well-being in elderly nursing home residents: A study protocol of a randomized controlled trial in the PROCARE (prevention and occupational health in long-term care) project. BMC Geriatr. 2019, 19, 369. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Farina, N.; Lowry, R.G. The validity of consumer-level activity monitors in healthy older adults in free-living conditions. J. Aging Phys. Act. 2018, 26, 128–135. [Google Scholar] [CrossRef]
- Ferguson, T.; Rowlands, A.V.; Olds, T.; Maher, C. The validity of consumer-level, activity monitors in healthy adults worn in free-living conditions: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, S.S.; Tiedemann, A.; Hassett, L.M.; Ramsay, E.; Kirkham, C.; Chagpar, S.; Sherrington, C. Validity of the fitbit activity tracker for measuring steps in community-dwelling older adults. BMJ Open Sport Exerc. Med. 2015, 1, e000013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alharbi, M.; Bauman, A.; Neubeck, L.; Gallagher, R. Validation of Fitbit-Flex as a measure of free-living physical activity in a community-based phase III cardiac rehabilitation population. Eur. J. Prev. Cardiol. 2016, 23, 1476–1485. [Google Scholar] [CrossRef]
- van Blarigan, E.L.; Kenfield, S.A.; Tantum, L.; Cadmus-Bertram, L.A.; Carroll, P.R.; Chan, J.M. The fitbit one physical activity tracker in men with prostate cancer: Validation study. JMIR Cancer 2017, 3, e5. [Google Scholar] [CrossRef]
- Meyer, J.; von Holdt, K.; Beck, E.; Brandes, M.; Pischke, C.; Voelcker-Rehage, C. Toy or tool? Activity trackers for the assessment of physical activity in the wild. In 2019 IEEE International Conference on Healthcare Informatics (ICHI), 10–13 June 2019, Xi’an, China; IEEE: Piscataway, NJ, USA, 2019; pp. 1–9. ISBN 978-1-5386-9138-0. [Google Scholar]
- Meyer, J.; Wasmann, M.; Heuten, W.; El Ali, A.; Boll, S.C.J. Identification and Classification of Usage Patterns in Long-Term Activity Tracking. In Explore, Innovate, Inspire, CHI ’17, Proceedings of the CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; Mark, G., Fussell, S., Lampe, C., Schraefel, M.C., Hourcade, J.P., Appert, C., Wigdor, D., Eds.; Association for Computing Machinery Inc. (ACM): New York, NY, USA, 2017; pp. 667–678. ISBN 9781450346559. [Google Scholar]
- Alessi, C.A.; Martin, J.L.; Webber, A.P.; Cynthia Kim, E.; Harker, J.O.; Josephson, K.R. Randomized, controlled trial of a nonpharmacological intervention to improve abnormal sleep/wake patterns in nursing home residents. J. Am. Geriatr. Soc. 2005, 53, 803–810. [Google Scholar] [CrossRef]
- Minge, M.; Riedel, L. meCUE-Ein modularer fragebogen zur erfassung des nutzungserlebens. In Mensch Computer 2013: Interaktive Vielfalt; Oldenburg Verlag: Munich, Germany, 2013. [Google Scholar]
- Meyer, J.; von Holdt, K.; Bragina, I.; Voelcker-Rehage, C. Using Activity Tracker Data for the Assessment of Physical Activity in Public Health Studies. In 2018 IEEE International Conference on Healthcare Informatics, 4–7 June 2018, New York, NY, USA; IEEE: Piscataway, NJ, USA, 2018; pp. 396–397. ISBN 978-1-5386-5377-7. [Google Scholar]
- Muellmann, S.; Buck, C.; Voelcker-Rehage, C.; Bragina, I.; Lippke, S.; Meyer, J.; Peters, M.; Pischke, C.R. Effects of two web-based interventions promoting physical activity among older adults compared to a delayed intervention control group in Northwestern Germany: Results of the PROMOTE community-based intervention trial. Prev. Med. Rep. 2019, 15, 100958. [Google Scholar] [CrossRef]
- Choi, B.C.K.; Pak, A.W.P.; Choi, J.C.L.; Choi, E.C.L. Daily step goal of 10,000 steps: A literature review. Clin. Invest. Med. 2007, 30, E146–E151. [Google Scholar] [CrossRef] [Green Version]
- Tudor-Locke, C.; Craig, C.L.; Aoyagi, Y.; Bell, R.C.; Croteau, K.A.; de Bourdeaudhuij, I.; Ewald, B.; Gardner, A.W.; Hatano, Y.; Lutes, L.D.; et al. How many steps/day are enough? For older adults and special populations. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 80. [Google Scholar] [CrossRef] [Green Version]
- Ogilvie, D.; Foster, C.E.; Rothnie, H.; Cavill, N.; Hamilton, V.; Fitzsimons, C.F.; Mutrie, N. Interventions to promote walking: Systematic review. BMJ 2007, 334, 1204. [Google Scholar] [CrossRef] [Green Version]
- Arnardottir, N.Y.; Koster, A.; van Domelen, D.R.; Brychta, R.J.; Caserotti, P.; Eiriksdottir, G.; Sverrisdottir, J.E.; Launer, L.J.; Gudnason, V.; Johannsson, E.; et al. Objective measurements of daily physical activity patterns and sedentary behaviour in older adults: Age, Gene/Environment Susceptibility-Reykjavik study. Age Ageing 2013, 42, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.G.; Fox, K.R.; Hillsdon, M.; Sharp, D.J.; Coulson, J.C.; Thompson, J.L. Objectively measured physical activity in a diverse sample of older urban UK adults. Med. Sci. Sports Exerc. 2011, 43, 647–654. [Google Scholar] [CrossRef]
- Harris, T.J.; Owen, C.G.; Victor, C.R.; Adams, R.; Cook, D.G. What factors are associated with physical activity in older people, assessed objectively by accelerometry? Br. J. Sports Med. 2009, 43, 442. [Google Scholar] [CrossRef]
- Koolhaas, C.M.; van Rooij, F.J.A.; Schoufour, J.D.; Cepeda, M.; Tiemeier, H.; Brage, S.; Franco, O.H. Objective measures of activity in the elderly: Distribution and associations with demographic and health factors. J. Am. Med. Dir. Assoc. 2017, 18, 838–847. [Google Scholar] [CrossRef]
- Lohne-Seiler, H.; Hansen, B.H.; Kolle, E.; Anderssen, S.A. Accelerometer-determined physical activity and self-reported health in a population of older adults (65–85 years): A cross-sectional study. BMC Public Health 2014, 14, 284. [Google Scholar] [CrossRef] [Green Version]
- van Ballegooijen, A.J.; van der Ploeg, H.P.; Visser, M. Daily sedentary time and physical activity as assessed by accelerometry and their correlates in older adults. Eur. Rev. Aging Phys. Act. 2019, 16, 3. [Google Scholar] [CrossRef] [Green Version]
- Barber, S.E.; Forster, A.; Birch, K.M. Levels and patterns of daily physical activity and sedentary behavior measured objectively in older care home residents in the United Kingdom. J. Aging Phys. Act. 2015, 23, 133–143. [Google Scholar] [CrossRef]
- Chau, J.Y.; Grunseit, A.C.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.E.; Bauman, A.E.; van der Ploeg, H.P. Daily sitting time and all-cause mortality: A meta-analysis. PLoS ONE 2013, 8, e80000. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Davis, M.; Stathi, A.; Hamer, M. Associations between multiple indicators of objectively-measured and self-reported sedentary behaviour and cardiometabolic risk in older adults. Prev. Med. 2012, 54, 82–87. [Google Scholar] [CrossRef]
- Thibaud, M.; Bloch, F.; Tournoux-Facon, C.; Brèque, C.; Rigaud, A.S.; Dugué, B.; Kemoun, G. Impact of physical activity and sedentary behaviour on fall risks in older people: A systematic review and meta-analysis of observational studies. Eur. Rev. Aging Phys. Act. 2012, 9, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef] [Green Version]
- Sardinha, L.B.; Santos, D.A.; Silva, A.M.; Baptista, F.; Owen, N. Breaking-up sedentary time is associated with physical function in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonsick, E.M.; Guralnik, J.M.; Volpato, S.; Balfour, J.; Fried, L.P. Just get out the door! Importance of walking outside the home for maintaining mobility: Findings from the women’s health and aging study. J. Am. Geriatr. Soc. 2005, 53, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazar, A.; Koehler, C.; Tanenbaum, J.; Nguyen, D.H. Why We Use and Abandon Smart Devices. In Proceedings of the 2015 ACM International Joint Conference, Osaka, Japan, 7–11 September 2015; Mase, K., Ed.; ACM: Osaka, Japan, 2015; pp. 635–646. ISBN 9781450335744. [Google Scholar]
- Lee, H.; Lee, Y. A Look at Wearable Abandonment. In Proceedings of the 2017 18th IEEE International Conference on Mobile Data Management (MDM), Daejeon, South Korea, 29 May–1 June 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 392–393. ISBN 978-1-5386-3932-0. [Google Scholar]
- Shin, G.; Jarrahi, M.H.; Fei, Y.; Karami, A.; Gafinowitz, N.; Byun, A.; Lu, X. Wearable activity trackers, accuracy, adoption, acceptance and health impact: A systematic literature review. J. Biomed. Inf. 2019, 93, 103153. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, D.; Kadokura, E.A.; Bouldin, E.D.; Miyawaki, C.E.; Higano, C.S.; Hartzler, A.L. Acceptability of Fitbit for physical activity tracking within clinical care among men with prostate cancer. Amia Annu. Symp. Proc. 2016, 2016, 1050–1059. [Google Scholar]
- Kolt, G.S.; Schofield, G.M.; Kerse, N.; Garrett, N.; Ashton, T.; Patel, A. Healthy steps trial: Pedometer-based advice and physical activity for low-active older adults. Ann. Fam. Med. 2012, 10, 206–212. [Google Scholar] [CrossRef]
- Lauritzen, J.; Muñoz, A.; Sevillano Ramos, J.L.; Civit Balcells, A. The usefulness of activity trackers in elderly with reduced mobility: A case study. Stud. Health Technol. Inform. 2013, 192, 759–762. [Google Scholar]
- Fokkema, T.; Kooiman, T.J.; Krijnen, W.P.; van der Schans, C.P.; de Groot, M. Reliability and validity of ten consumer activity trackers depend on walking speed. Med. Sci. Sports Exerc. 2017, 49, 793–800. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean ± SD OR Number (%) | ||||
|---|---|---|---|---|---|
| Whole Group (n = 22) | <85 (n = 10) | ≥85 (n = 12) | Men (n = 6) | Women (n = 16) | |
| Age (years) | 86.4 ± 9.3 | 78.4 ± 6.6 | 93.1 ± 4.9 | 79.3 ± 8.5 | 89.1 ± 8.4 |
| Gender (women) | 16 (72.7) | 5 | 11 | 6 | 16 |
| Cognitive status | |||||
| No dementia (MoCA >23 OR staff survey = “no dementia”) | 8 (36.4) | 3 | 5 | 2 | 6 |
| Mild dementia (MoCA = 18–23 OR staff survey = “mild dementia” | 8 (36.4) | 4 | 4 | 3 | 5 |
| Moderate dementia (MoCA 10–17 OR staff survey = “moderate dementia”) | 4 (18.2) | 2 | 2 | 1 | 3 |
| Missing | 2 (9.1) | 1 | 1 | - | 2 |
| Height (cm) | 162.3 ± 9.6 | 165.2 ± 9.5 | 159.7 ± 9.4 | 170.2 ± 12.2 | 159.2 ± 6.4 |
| Weight (kg) | 69.0 ± 17.4 | 75.7 ± 14.7 | 63.5 ± 18.1 | 76.3 ± 15.8 | 66.3 ± 17.7 |
| BMI (kg/m²) | 26.4 ± 6.0 | 27.7 ± 4.7 | 25.2 ± 7.0 | 26.4 ± 5.0 | 26.4 ± 6.5 |
| Current level of activity | |||||
| never | 3 (13.6) | 2 | 1 | 1 | 2 |
| rarely | 3 (13.6) | 0 | 3 | 1 | 2 |
| frequently | 7 (31.8) | 2 | 5 | 1 | 6 |
| daily | 9 (40.9) | 6 | 3 | 3 | 6 |
| Past level of activity | |||||
| never | 4 (18.2) | 1 | 3 | 1 | 3 |
| rarely | 6 (27.3) | 4 | 2 | 2 | 4 |
| occasionally | 5 (22.7) | 2 | 3 | 1 | 4 |
| regularly | 7 (31.8) | 3 | 4 | 2 | 5 |
| n | Mean (SD) | Min | Max | |
|---|---|---|---|---|
| Steps entire period | 22 | 1007.0 (860) | 70.0 | 2770.0 |
| Steps summer | 20 | 1055.0 (933) | 61.0 | 2930.0 |
| Steps first seven days | 22 | 974.0 (877) | 53.0 | 2821.0 |
| Sedentary minutes entire period | 17 | 561.7 (86.3) | 444.6 | 824.7 |
| Sedentary minutes summer | 17 | 568.1 (42.5) | 501.2 | 632.2 |
| Sedentary minutes first seven days | 16 | 541.0 (113.9) | 352.2 | 810.9 |
| Longest zero entire period | 17 | 154.6 (37.4) | 94.3 | 247.6 |
| Longest zero summer | 17 | 156.4 (31.8) | 116.4 | 274.2 |
| Longest zero first seven days | 16 | 152.3 (37.7) | 79.2 | 225.0 |
| Wearing Week | First Wearing Week Mean (SD) | Fifth Wearing Week Mean (SD) | Wilcoxon-Test z-Value; p-Value |
|---|---|---|---|
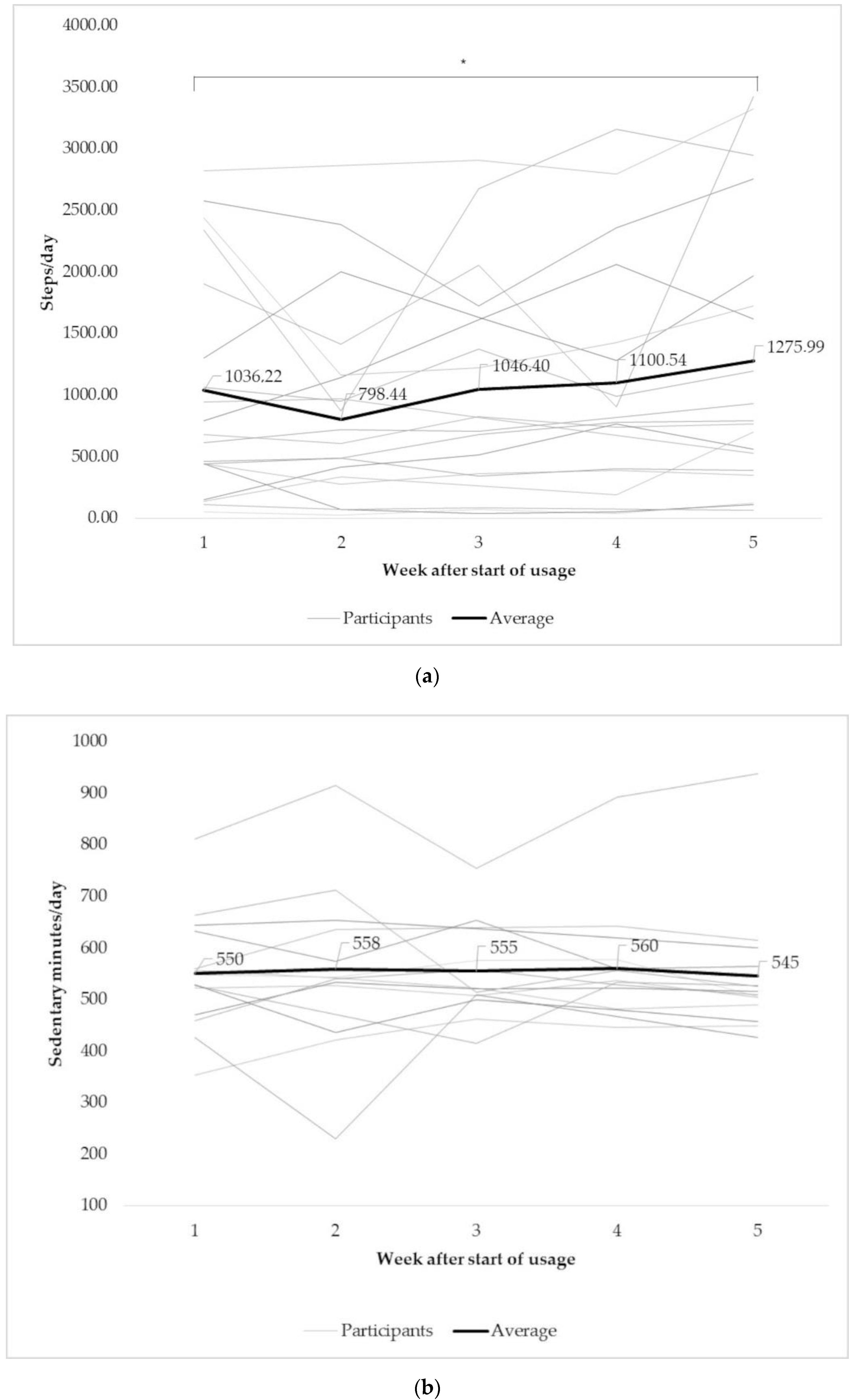
| Steps (n = 19) | 1020 (973) | 1276 (1115) | −2,1; 0.04 * |
| Sedentary minutes (n = 14) | 550.9 (122.5) | 549.9 (113.5) | −0.31; 0.98 |
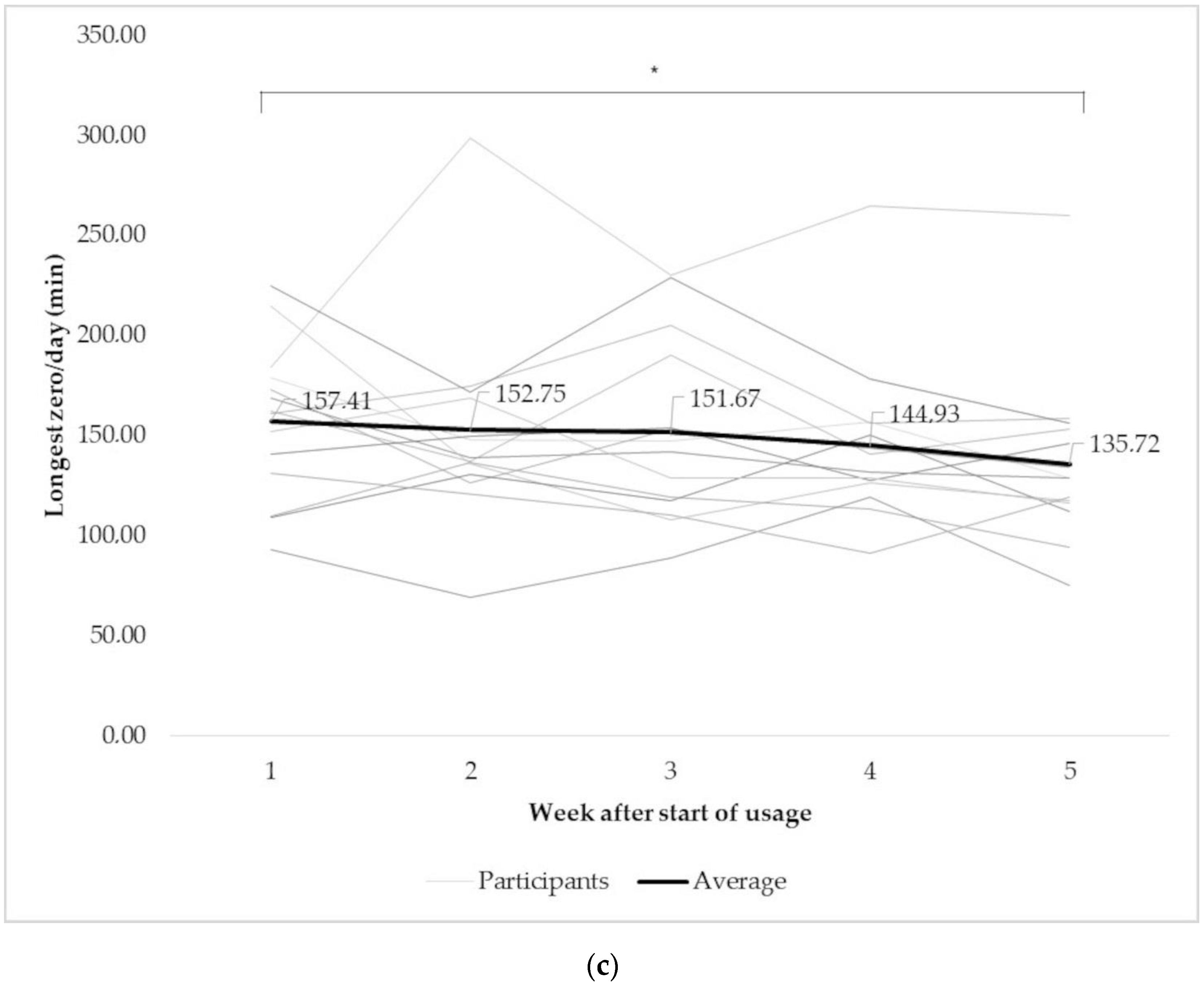
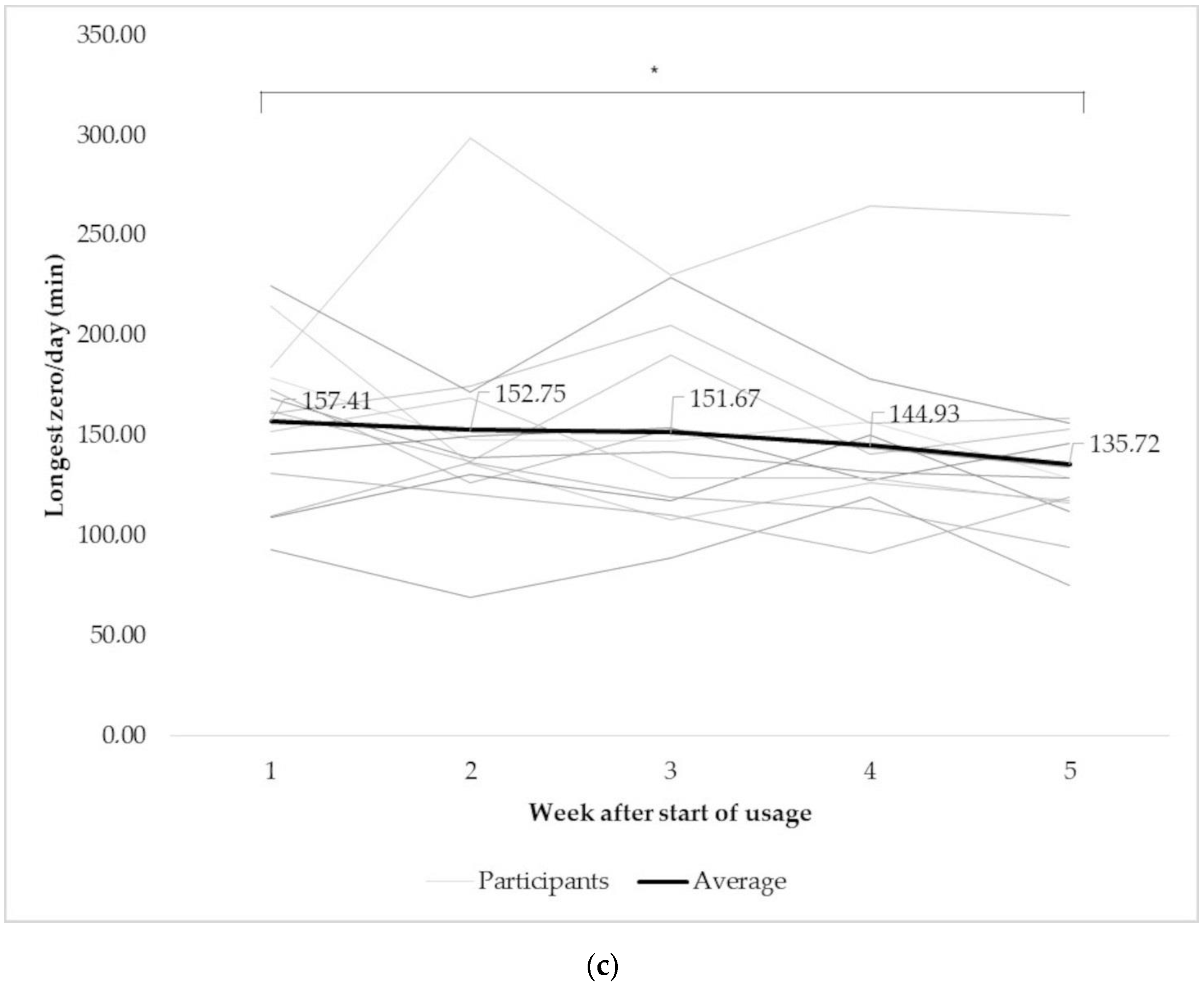
| Longest zero (n = 14) | 157.4 (38.4) | 135.7 (42.7) | −2.1; 0.03 * |
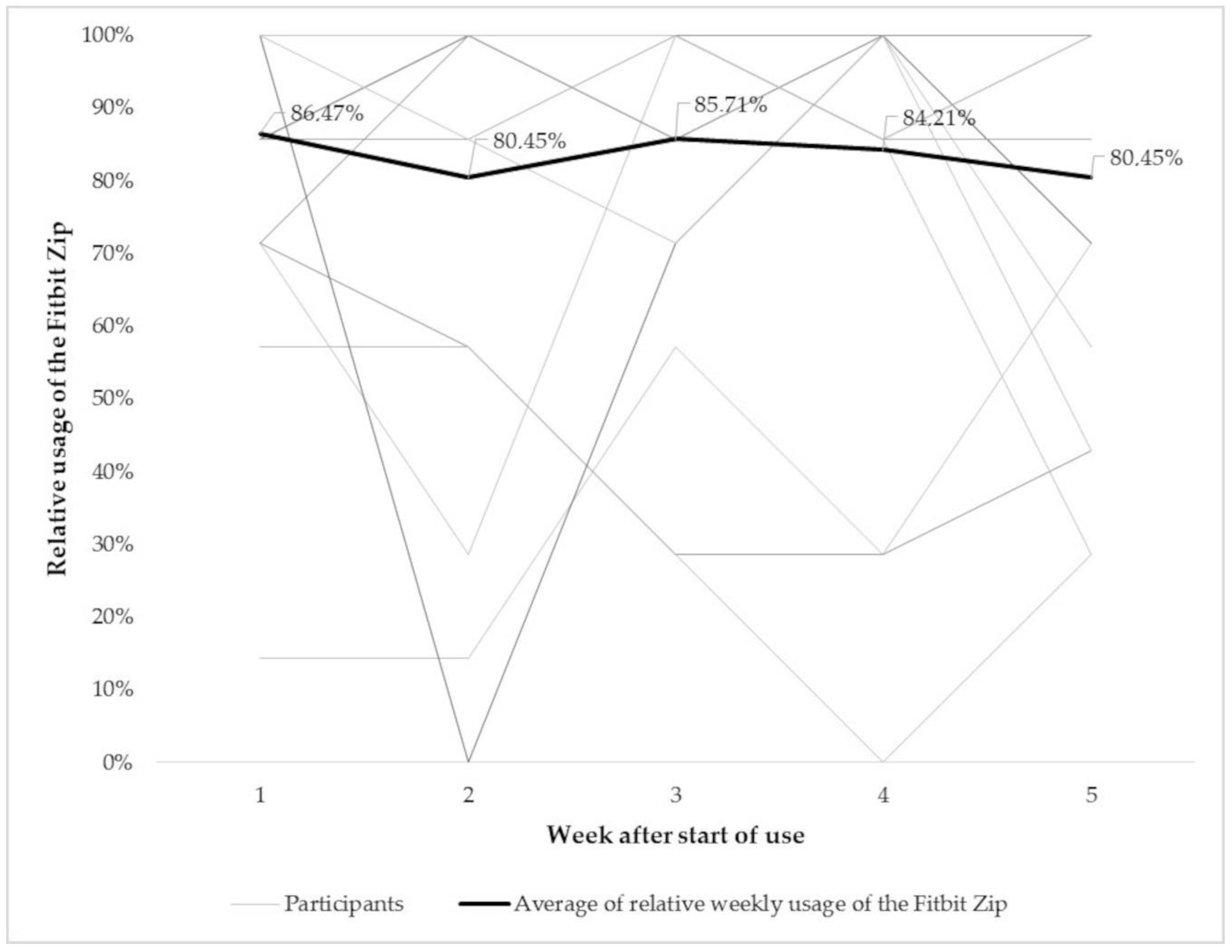
| Usage time (%; n = 19) | 85.1 (24.4) | 80.5 (27.0) | −0.9; 0.37 |
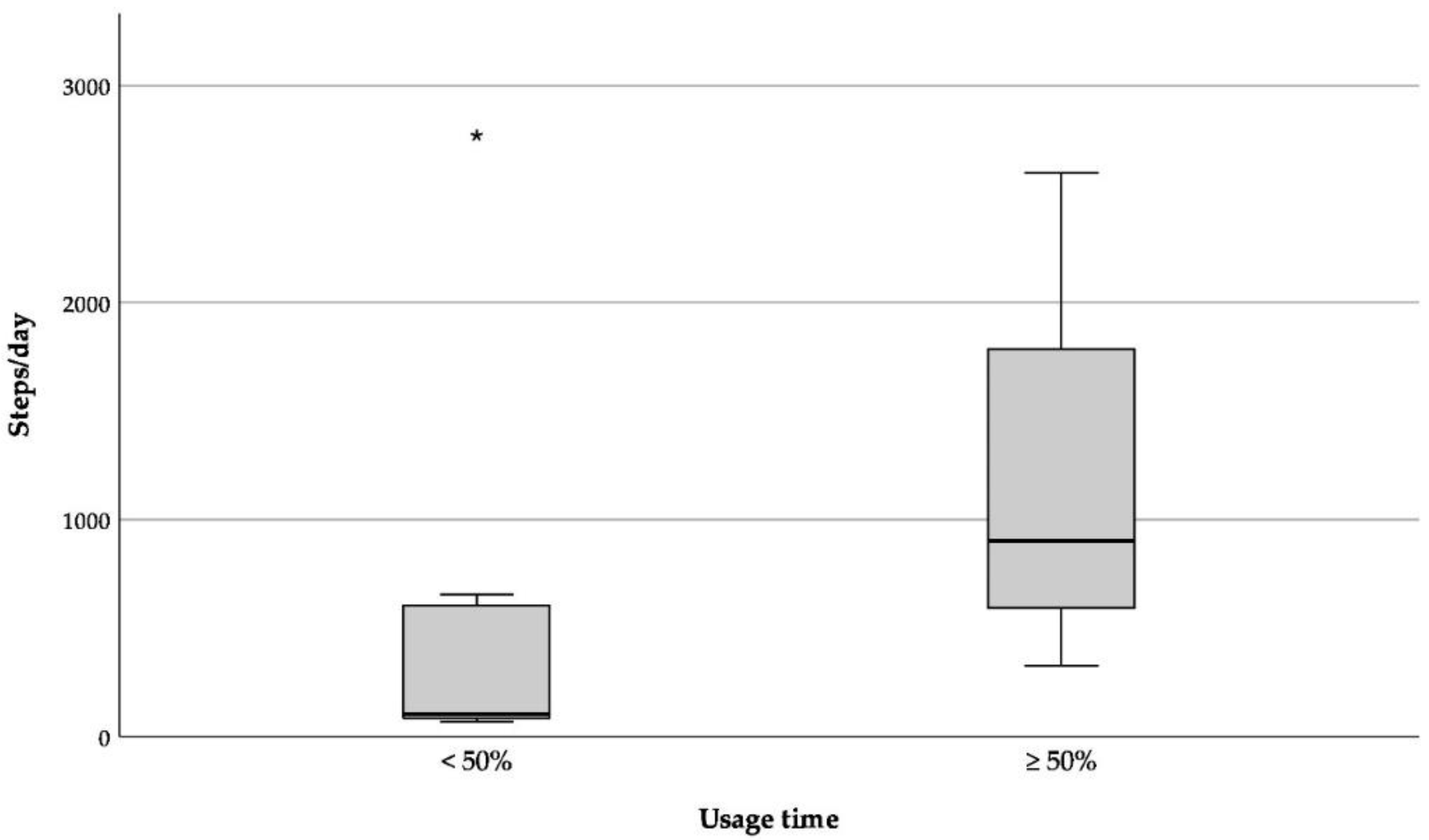
| Relative Usage Time of the Fitbit Zip | <50% | ≥50% | Mann-Whitney U-Test z-Value; p-Value |
| Steps | 617.7 (980.4) | 1188.1 (766.4) | −2.1; 0.04 * |
| Age | <85 Years Mean (SD) | ≥85 Years Mean (SD) | Mann-Whitney U-Test z-Value; p-Value |
|---|---|---|---|
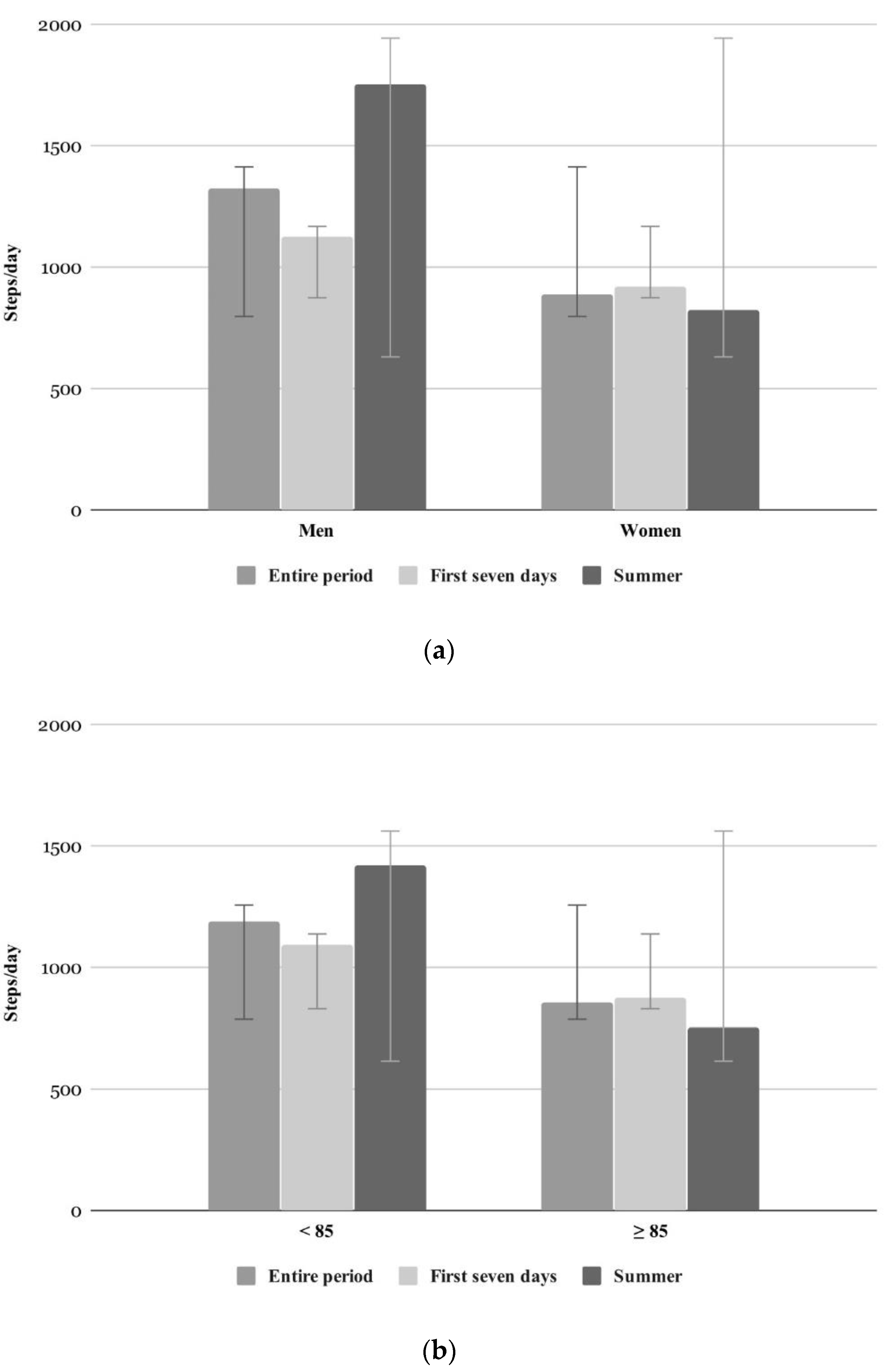
| Steps entire period | 1188.0 (905) | 856.0 (829) | −0.7; 0.54 |
| Steps summer | 1423.0 (1069) | 754.0 (720) | −1.1; 0.30 |
| Steps first seven days | 1093.0 (870) | 875.0 (908) | −0.8; 0.46 |
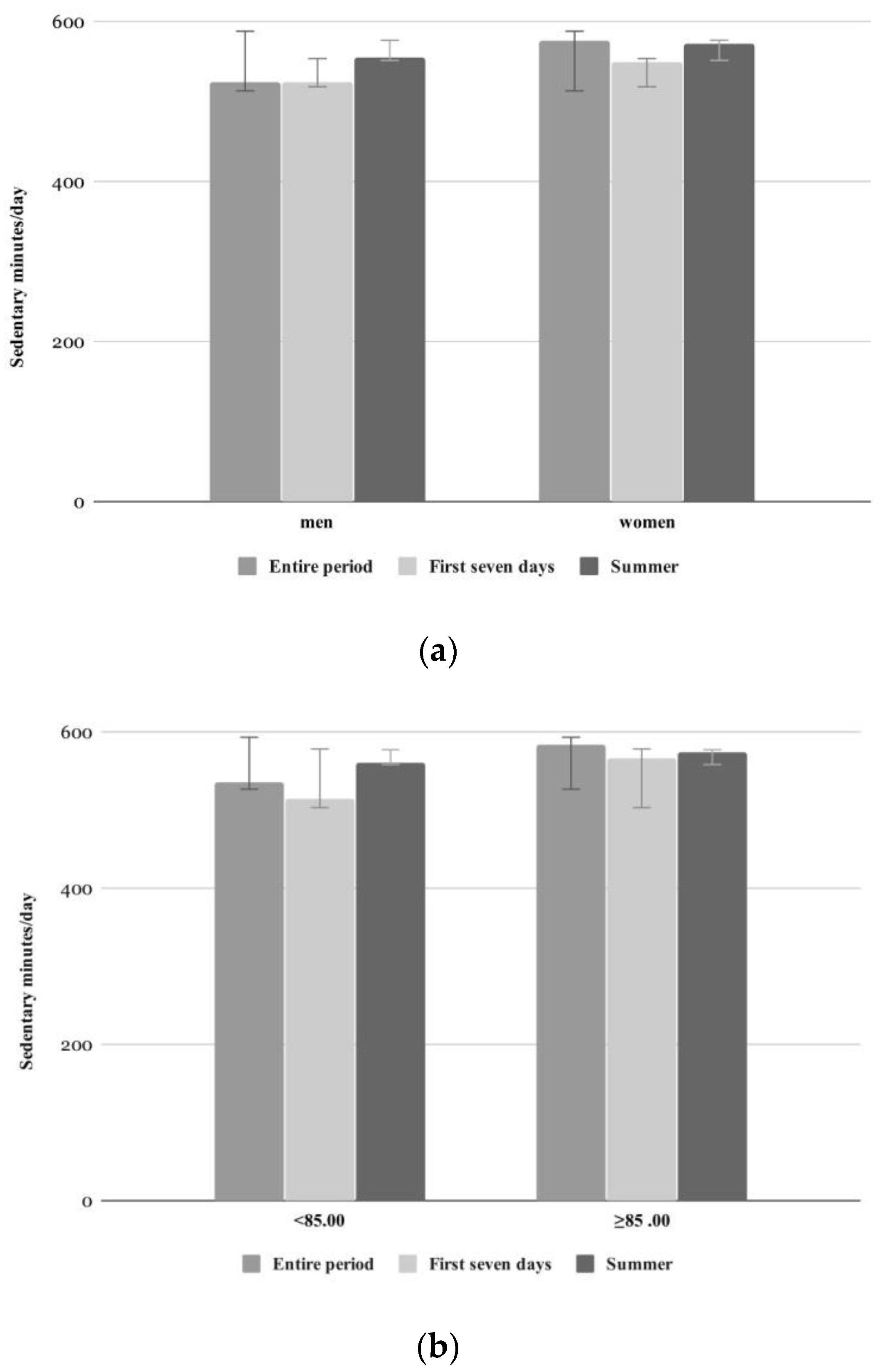
| Sedentary minutes entire period | 536.8 (51.7) | 583.8 (106.7) | −1.0; 0.34 |
| Sedentary minutes summer | 561.4 (40.5) | 574.8 (46.5) | −0.7; 0.48 |
| Sedentary minutes first seven days | 514.5 (93.2) | 567.5 (132.0) | −0.6; 0.53 |
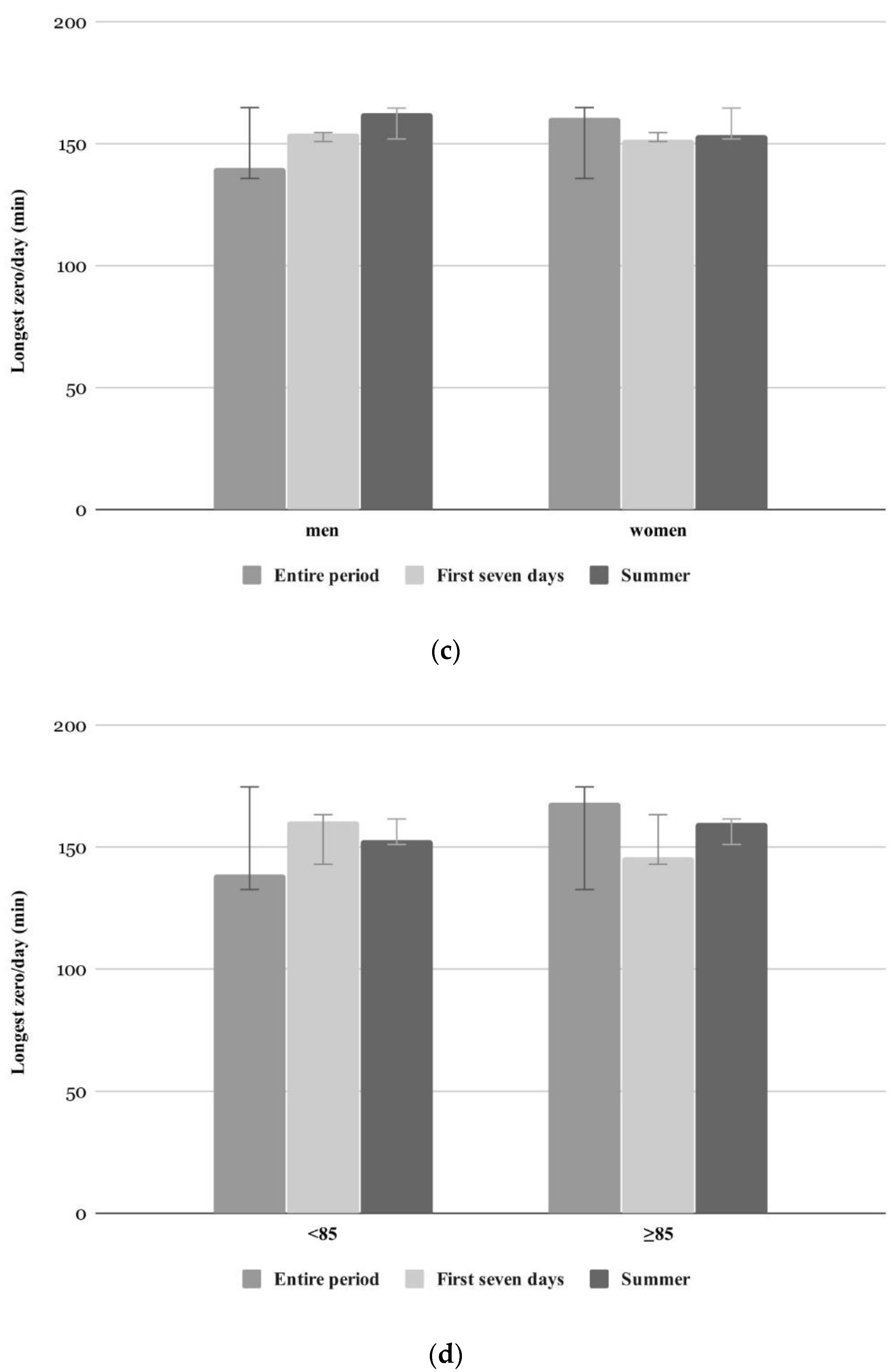
| Longest zero entire period | 138.8 (23.6) | 168.6 (42.9) | −1.6; 0.29 |
| Longest zero summer | 152.7 (23.7) | 160.1 (40.0) | −0.3; 0.75 |
| Longest zero first seven days | 160.4 (29.3) | 146.0 (43.8) | −0.7; 0.49 |
| Gender | Men Mean (SD) | Women Mean (SD) | Mann-Whitney U-Test z-Value; p-Value |
| Steps entire period | 1323.0 (1009) | 888.0 (801) | −1.0; 0.33 |
| Steps summer | 1752.0 (1140) | 823.0 (761) | −1.8; 0.08 |
| Steps first seven days | 1126.0 (833) | 918.0 (912) | −0.7; 0.54 |
| Sedentary minutes entire period | 524.5 (56.7) | 577.2 (93.6) | −1.2; 0.25 |
| Sedentary minutes summer | 555.3 (39.6) | 573.2 (44.5) | −0.7; 0.48 |
| Sedentary minutes first seven days | 523.9 (125.3) | 548.8 (113.8) | −0.1; 1.00 |
| Longest zero entire period | 140.1 (28.3) | 160.6 (40.1) | −0.4; 0.67 |
| Longest zero summer | 162.8 (23.3) | 153.8 (35.4) | −1.3; 0.20 |
| Longest zero first seven days | 154.1 (34.8) | 151.5 (40.5) | −0.1; 0.96 |
| Reason for Temporary Interruption or Premature Abortion n = 20 | Number (%) |
|---|---|
| Forgot to apply | 11 (55) |
| Hospitalization | 1 (5) |
| Lost Interest | 4 (20) |
| Lost Fitbit Zip (temporarily) | 4 (20) |
| Item | Mean (SD) | ||||
|---|---|---|---|---|---|
| Whole Group (n = 18) | <85 (n = 9) | ≥85 (n = 9) | Men (n = 5) | Women (n = 13) | |
| Acceptability (1–5 *) | |||||
| Activity tracker is annoying | 1.27 (0.75) | 1.11 (0.33) | 1.44 (1.01) | 1.00 (0.00) | 1.38 (0.87) |
| Usability (1–5 *) | |||||
| Activity tracker is easy to use (e.g., attaching on clothes) | 3.39 (1.20) | 3.67 (1.22) | 3.11 (1.17) | 3.40 (1.14) | 3.38 (1.26) |
| Personal handling of the activity tracker without problems | 3.06 (0.94) | 3.00 (1.00) | 3.11 (0.93) | 3.00 (1.00) | 3.08 (0.95) |
| Current motivation (1–5 *) | |||||
| Activity tracker motivates me to do more physical activity | 1.78 (0.81) | 1.67 (0.87) | 1.89 (0.78) | 2.00 (1.00) | 1.69 (0.75) |
| Potential Motivation (1–5 *) | |||||
| Activity tracker with feedback would motivate me to do more physical activity | 3.45 (1.15) | 3.00 (1.00) | 3.89 (1.17) | 3.40 (1.14) | 3.46 (1.20) |
| Overall experience (0–10 °) | |||||
| Overall experience of the activity tracker | 6.95 (1.55) | 7.00 (1.58) | 6.89 (1.62) | 6.80 (1.10) | 7.00 (1.73) |
| Item | Strongly Disagree/Disagree N (%) | Neither Agree Nor Disagree N (%) | Strongly Agree/Agree N (%) |
|---|---|---|---|
| Acceptability | |||
| Activity tracker is annoying | 17 (94.4) | 0 (0) | 1 (5.6) |
| Usability | |||
| Activity tracker is easy to use (e.g., attaching on clothes) | 6 (33.3) | 3 (16.7) | 9 (50.0) |
| Personal handling of the activity tracker without problems | 7 (38.9) | 3 (16.7) | 8 (44.4) |
| Current motivation | |||
| Activity tracker motivates me to do more physical activity | 14 (77.8) | 4 (22.2) | 0 (0.0) |
| Potential Motivation | |||
| Activity tracker with feedback would motivate me to do more physical activity | 4 (22.2) | 7 (38.9) | 7 (38.9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auerswald, T.; Meyer, J.; von Holdt, K.; Voelcker-Rehage, C. Application of Activity Trackers among Nursing Home Residents—A Pilot and Feasibility Study on Physical Activity Behavior, Usage Behavior, Acceptance, Usability and Motivational Impact. Int. J. Environ. Res. Public Health 2020, 17, 6683. https://doi.org/10.3390/ijerph17186683
Auerswald T, Meyer J, von Holdt K, Voelcker-Rehage C. Application of Activity Trackers among Nursing Home Residents—A Pilot and Feasibility Study on Physical Activity Behavior, Usage Behavior, Acceptance, Usability and Motivational Impact. International Journal of Environmental Research and Public Health. 2020; 17(18):6683. https://doi.org/10.3390/ijerph17186683
Chicago/Turabian StyleAuerswald, Tina, Jochen Meyer, Kai von Holdt, and Claudia Voelcker-Rehage. 2020. "Application of Activity Trackers among Nursing Home Residents—A Pilot and Feasibility Study on Physical Activity Behavior, Usage Behavior, Acceptance, Usability and Motivational Impact" International Journal of Environmental Research and Public Health 17, no. 18: 6683. https://doi.org/10.3390/ijerph17186683
APA StyleAuerswald, T., Meyer, J., von Holdt, K., & Voelcker-Rehage, C. (2020). Application of Activity Trackers among Nursing Home Residents—A Pilot and Feasibility Study on Physical Activity Behavior, Usage Behavior, Acceptance, Usability and Motivational Impact. International Journal of Environmental Research and Public Health, 17(18), 6683. https://doi.org/10.3390/ijerph17186683