The Effects of Exclusively Resistance Training-Based Supervised Programs in People with Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search
2.3. Study Selection
2.4. Data Collection Process
2.5. Data Items
2.6. Risk of Bias in Individual Studies and Across Studies
2.7. Summary Measures, Synthesis of Results and Risk of Bias across Studies
3. Results
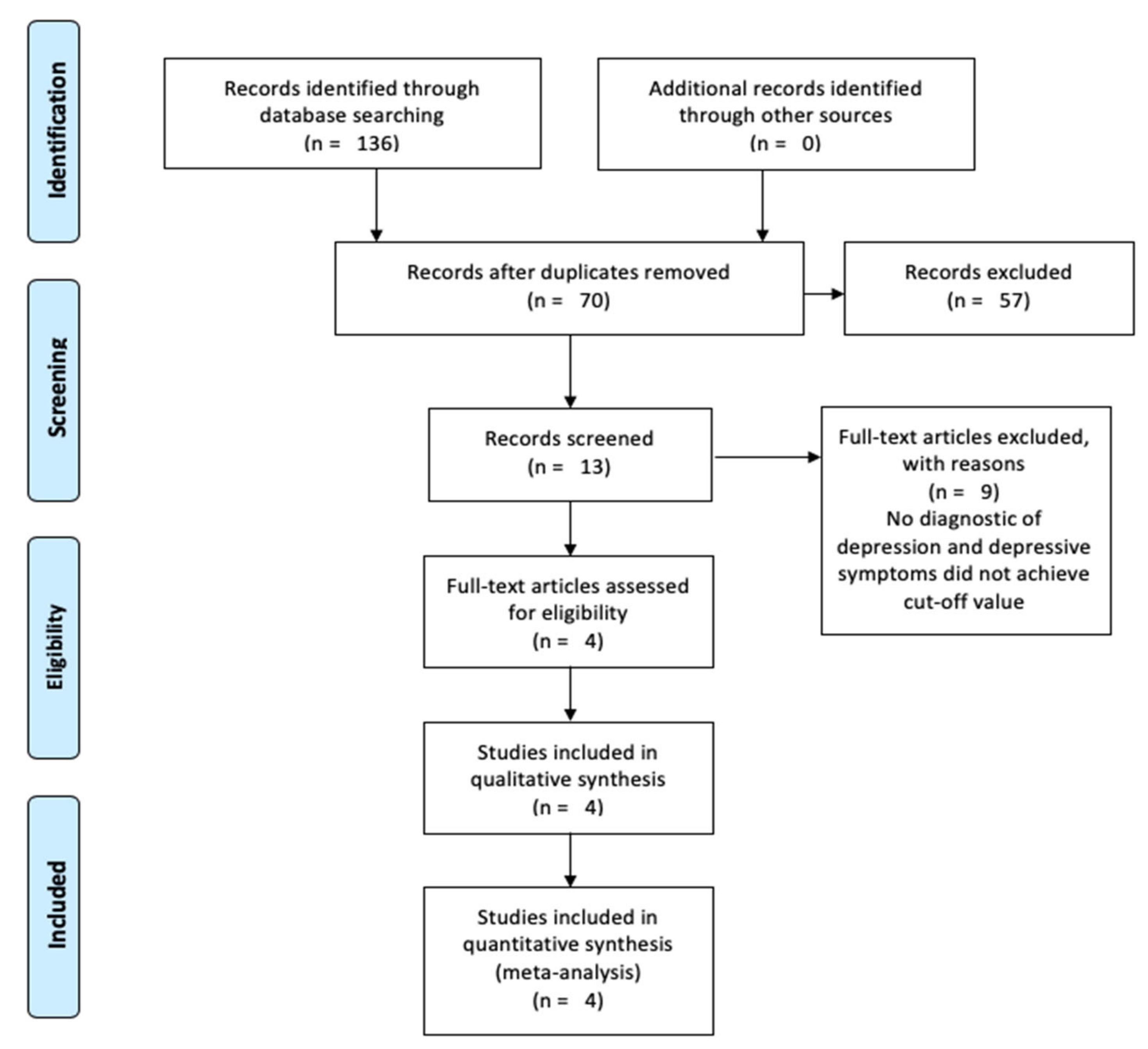
3.1. Study Selection
3.2. Characteristics and Results of Individual Studies
3.3. Risk of Bias within Studies and across Studies
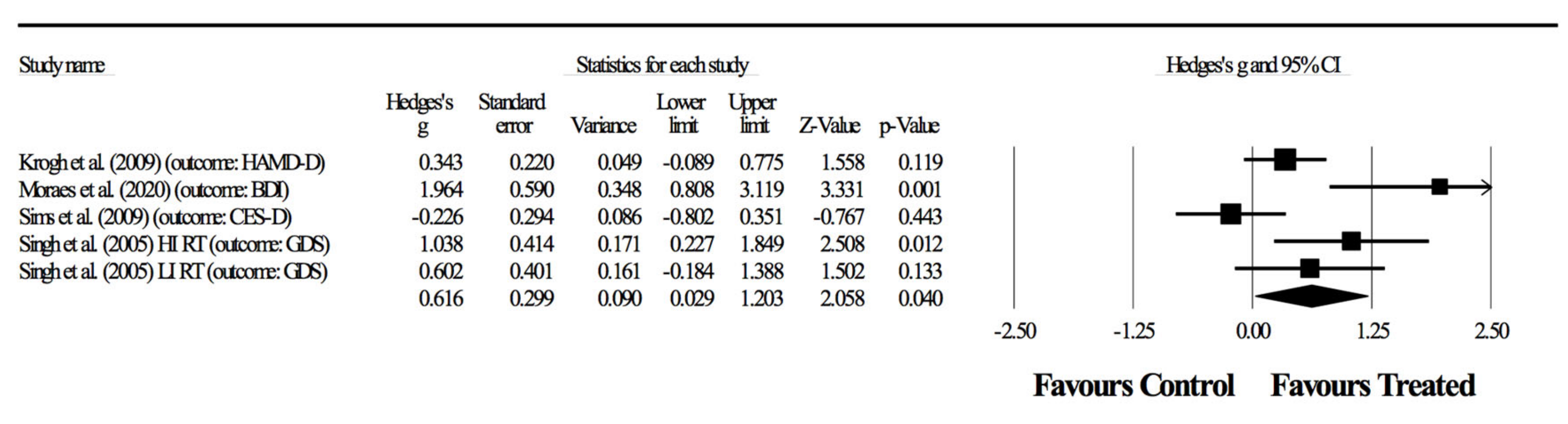
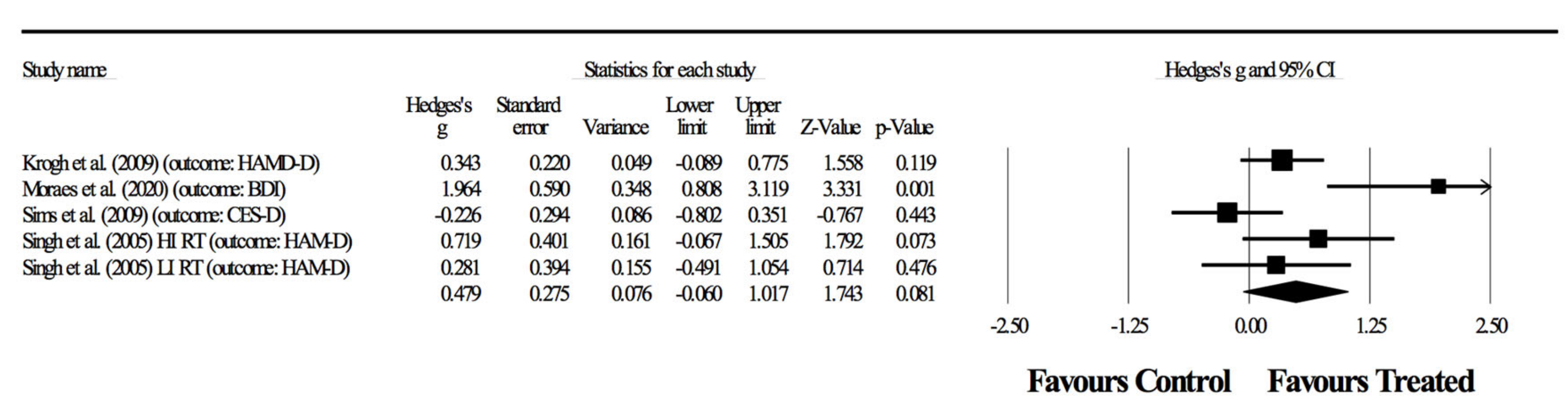
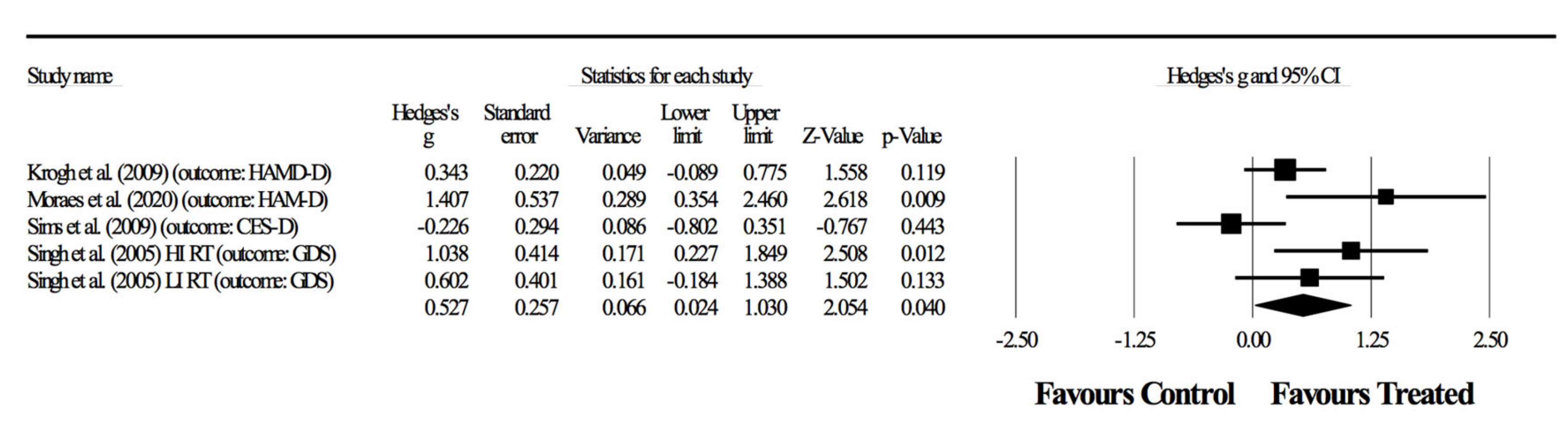
3.4. Meta-Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Patel, V.; Chisholm, D.; Parikh, R.; Charlson, F.J.; Degenhardt, L.; Dua, T.; Ferrari, A.J.; Hyman, S.; Laxminarayan, R.; Levin, C.; et al. Addressing the burden of mental, neurological, and substance use disorders: Key messages from Disease Control Priorities. Lancet 2016, 387, 1672–1685. [Google Scholar] [CrossRef] [Green Version]
- Arshad Ali, S.; Baloch, M.; Ahmed, N.; Arshad Ali, A.; Iqbal, A. The outbreak of Coronavirus Disease 2019 (COVID-19)—An emerging global health threat. J. Infect. Public Health 2020, 13, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yang, Z.; Qiu, H.; Wang, Y.; Jian, L.; Ji, J.; Li, K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry 2020, 19, 249–250. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.S.; Chee, C.Y.; Ho, R.C. Mental Health Strategies to Combat the Psychological Impact of COVID-19 Beyond Paranoia and Panic. Ann. Acad. Med. Singap. 2020, 49, 155–160. [Google Scholar] [PubMed]
- Netz, Y. Is the Comparison between Exercise and Pharmacologic Treatment of Depression in the Clinical Practice Guideline of the American College of Physicians Evidence-Based? Front. Pharmacol. 2017, 8, 257. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Vancampfort, D.; Hallgren, M.; Firth, J.; Veronese, N.; Solmi, M.; Brand, S.; Cordes, J.; Malchow, B.; Gerber, M.; et al. EPA guidance on physical activity as a treatment for severe mental illness: A meta-review of the evidence and Position Statement from the European Psychiatric Association (EPA), supported by the International Organization of Physical Therapists in Mental Health (IOPTMH). Eur. Psychiatry 2018, 54, 124–144. [Google Scholar] [CrossRef] [Green Version]
- Brinsley, J.; Schuch, F.; Lederman, O.; Girard, D.; Smout, M.; Immink, M.A.; Stubbs, B.; Firth, J.; Davison, K.; Rosenbaum, S. Effects of yoga on depressive symptoms in people with mental disorders: A systematic review and meta-analysis. Br. J. Sports Med. 2020. [Google Scholar] [CrossRef]
- Cooney, G.M.; Dwan, K.; Greig, C.A.; Lawlor, D.A.; Rimer, J.; Waugh, F.R.; McMurdo, M.; Mead, G.E. Exercise for depression. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Heissel, A.; Zech, P.; Rapp, M.A.; Schuch, F.B.; Lawrence, J.B.; Kangas, M.; Heinzel, S. Effects of exercise on depression and anxiety in persons living with HIV: A meta-analysis. J. Psychosom. Res. 2019, 126, 109823. [Google Scholar] [CrossRef]
- Moura, A.M.C.; Lamegro, M.K.; Paes, F.; Rocha, N.B.F.; Simões-Silva, V.; Rocha, S.A.; Filho, A.S.S.; Rimes, R.; Manochio, J.; Budde, H.; et al. Comparison Among Aerobic Exercise and Other Types of Interventions to Treat Depression: A Systematic Review. CNS Neurol. Disord. Drug Targets 2015, 14, 1171–1183. [Google Scholar] [CrossRef] [Green Version]
- Perraton, L.G.; Kumar, S.; Machotka, Z. Exercise parameters in the treatment of clinical depression: A systematic review of randomized controlled trials. J. Eval. Clin. Pract. 2010, 16, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Silveira, H.; Moraes, H.; Oliveira, N.; Coutinho, E.S.F.; Laks, J.; Deslandes, A. Physical Exercise and Clinically Depressed Patients: A Systematic Review and Meta-Analysis. Neuropsychobiology 2013, 67, 61–68. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Schuch, F.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.; Reichert, T.; Bagatini, N.C.; Bgeginski, R.; Stubbs, B. Physical activity and sedentary behavior in people with major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2017, 210, 139–150. [Google Scholar] [CrossRef] [Green Version]
- Dunn, A.L.; Trivedi, M.H.; Kampert, J.B.; Clark, C.G.; Chambliss, H.O. Exercise treatment for depression: Efficacy and dose response. Am. J. Prev. Med. 2005, 28, 1–8. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Rosenbaum, S.; Ward, P.B.; Richards, J.; Soundy, A.; Veronese, N.; Solmi, M.; Schuch, F.B. Dropout from exercise randomized controlled trials among people with depression: A meta-analysis and meta regression. J. Affect. Disord. 2016, 190, 457–466. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; Risi Ambrogioni, L.; Lo Presti, D.; Carnevale, A.; Candela, V.; Stelitano, G.; Schena, E.; Nazarian, A.; Denaro, V. Cost-Effectiveness of Supervised versus Unsupervised Rehabilitation for Rotator-Cuff Repair: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2852. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Babyak, M.A.; Doraiswamy, P.M.; Watkins, L.; Hoffman, B.M.; Barbour, K.A.; Herman, S.; Craighead, W.E.; Brosse, A.L.; Waugh, R.; et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom. Med. 2007, 69, 587–596. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Rosenbaum, S.; Vancampfort, D.; Ward, P.B.; Schuch, F.B. Exercise improves cardiorespiratory fitness in people with depression: A meta-analysis of randomized control trials. J. Affect. Disord. 2016, 190, 249–253. [Google Scholar] [CrossRef]
- Kim, Y.S.; O’Sullivan, D.M.; Shin, S.K. Can 24 weeks strength training reduce feelings of depression and increase neurotransmitter in elderly females? Exp. Gerontol. 2019, 115, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.R.; McDowell, C.P.; Hallgren, M.; Meyer, J.D.; Lyons, M.; Herring, M.P. Association of Efficacy of Resistance Exercise Training With Depressive Symptoms: Meta-analysis and Meta-regression Analysis of Randomized Clinical Trials. JAMA Psychiatry 2018, 75, 566–576. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- WHO. International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M. Rating depressive patients. J. Clin. Psychiatry 1980, 41, 21–24. [Google Scholar]
- Yesavage, J.A. Geriatric Depression Scale. Psychopharmacol. Bull. 1988, 24, 709–711. [Google Scholar]
- Pereira, D.S.; de Queiroz, B.Z.; Miranda, A.S.; Rocha, N.P.; Felício, D.C.; Mateo, E.C.; Favero, M.; Coelho, F.M.; Jesus-Moraleida, F.; Gomes Pereira, D.A.; et al. Effects of physical exercise on plasma levels of brain-derived neurotrophic factor and depressive symptoms in elderly women—A randomized clinical trial. Arch. Phys. Med. Rehabil. 2013, 94, 1443–1450. [Google Scholar] [CrossRef]
- Sims, J.; Hill, K.; Davidson, S.; Gunn, J.; Huang, N. Exploring the feasibility of a community-based strength training program for older people with depressive symptoms and its impact on depressive symptoms. BMC Geriatr. 2006, 6, 18. [Google Scholar] [CrossRef] [Green Version]
- Teychenne, M.; Lamb, K.E.; Main, L.; Miller, C.; Hahne, A.; Ford, J.; Rosenbaum, S.; Belavy, D. General strength and conditioning versus motor control with manual therapy for improving depressive symptoms in chronic low back pain: A randomised feasibility trial. PLoS ONE 2019, 14, e0220442. [Google Scholar] [CrossRef]
- Ansai, J.H.; Rebelatto, J.R. Effect of two physical exercise protocols on cognition and depressive symptoms in oldest-old people: A randomized controlled trial. Geriatr. Gerontol. Int. 2015, 15, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Chin, A.P.M.J.; van Poppel, M.N.; Twisk, J.W.; van Mechelen, W. Effects of resistance and all-round, functional training on quality of life, vitality and depression of older adults living in long-term care facilities: A ‘randomized’ controlled trial [ISRCTN87177281]. BMC Geriatr. 2004, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Kekäläinen, T.; Kokko, K.; Sipilä, S.; Walker, S. Effects of a 9-month resistance training intervention on quality of life, sense of coherence, and depressive symptoms in older adults: Randomized controlled trial. Qual. Life Res. 2018, 27, 455–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeCheminant, J.D.; Hinman, T.; Pratt, K.B.; Earl, N.; Bailey, B.W.; Thackeray, R.; Tucker, L.A. Effect of resistance training on body composition, self-efficacy, depression, and activity in postpartum women. Scand. J. Med. Sci. Sports 2014, 24, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Levinger, I.; Selig, S.; Goodman, C.; Jerums, G.; Stewart, A.; Hare, D.L. Resistance training improves depressive symptoms in individuals at high risk for type 2 diabetes. J. Strength Cond. Res. 2011, 25, 2328–2333. [Google Scholar] [CrossRef] [PubMed]
- Krogh, J.; Saltin, B.; Gluud, C.; Nordentoft, M. The DEMO trial: A randomized, parallel-group, observer-blinded clinical trial of strength versus aerobic versus relaxation training for patients with mild to moderate depression. J. Clin. Psychiatry 2009, 70, 790–800. [Google Scholar] [CrossRef]
- Moraes, H.S.; Silveira, H.S.; Oliveira, N.A.; Matta Mello Portugal, E.; Araújo, N.B.; Vasques, P.E.; Bergland, A.; Santos, T.M.; Engedal, K.; Coutinho, E.S.; et al. Is Strength Training as Effective as Aerobic Training for Depression in Older Adults? A Randomized Controlled Trial. Neuropsychobiology 2020, 79, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Sims, J.; Galea, M.; Taylor, N.; Dodd, K.; Jespersen, S.; Joubert, L.; Joubert, J. Regenerate: Assessing the feasibility of a strength-training program to enhance the physical and mental health of chronic post stroke patients with depression. Int. J. Geriatr. Psychiatry 2009, 24, 76–83. [Google Scholar] [CrossRef]
- Singh, N.A.; Stavrinos, T.A.; Scarbek, Y.; Galambos, G.; Liber, C.; Singh, M.A.F. A randomized controlled trial of high versus low intensity weight training versus general practitioner care for clinical depression in older adults. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2005, 60, 768–776. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2008; pp. 243–296. [Google Scholar]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A re-analysis of the Cochrane Library data: The dangers of unobserved heterogeneity in meta-analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Rush, A.J.; Trivedi, M.H.; Ibrahim, H.M.; Carmody, T.J.; Arnow, B.; Klein, D.N.; Markowitz, J.C.; Ninan, P.T.; Kornstein, S.; Manber, R.; et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): A psychometric evaluation in patients with chronic major depression. Biol. Psychiatry 2003, 54, 573–583. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Hamilton, M. Development of a Rating Scale for Primary Depressive Illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Reijnders, M.; Kishimoto, S.; Sakata, M.; DeRubeis, R.J.; Dimidjian, S.; Dozois, D.J.A.; Hegerl, U.; Hollon, S.D.; Jarrett, R.B.; et al. Translating the BDI and BDI-II into the HAMD and vice versa with equipercentile linking. Epidemiol. Psychiatr. Sci. 2020, 29, e24. [Google Scholar] [CrossRef] [Green Version]
- Isacsson, G.; Adler, M. Randomized clinical trials underestimate the efficacy of antidepressants in less severe depression. Acta Psychiatr. Scand. 2012, 125, 453–459. [Google Scholar] [CrossRef]
- Schuch, F.B.; Morres, I.D.; Ekkekakis, P.; Rosenbaum, S.; Stubbs, B. A critical review of exercise as a treatment for clinically depressed adults: Time to get pragmatic. Acta Neuropsychiatr. 2017, 29, 65–71. [Google Scholar] [CrossRef]
- Cooper, A.A.; Conklin, L.R. Dropout from individual psychotherapy for major depression: A meta-analysis of randomized clinical trials. Clin. Psychol. Rev. 2015, 40, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Moens, H.; Madou, T.; De Backer, T.; Vallons, V.; Bruyninx, P.; Vanheuverzwijn, S.; Mota, C.T.; Soundy, A.; Probst, M. Autonomous motivation is associated with the maintenance stage of behaviour change in people with affective disorders. Psychiatry Res. 2016, 240, 267–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancampfort, D.; Stubbs, B.; Ward, P.B.; Teasdale, S.; Rosenbaum, S. Integrating physical activity as medicine in the care of people with severe mental illness. Aust. N. Z. J. Psychiatry 2015, 49, 681–682. [Google Scholar] [CrossRef] [PubMed]
- De Hert, M.; Correll, C.U.; Bobes, J.; Cetkovich-Bakmas, M.; Cohen, D.; Asai, I.; Detraux, J.; Gautam, S.; Möller, H.-J.; Ndetei, D.M.; et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2011, 10, 52–77. [Google Scholar] [CrossRef] [Green Version]
- Vancampfort, D.; Correll, C.U.; Wampers, M.; Sienaert, P.; Mitchell, A.J.; De Herdt, A.; Probst, M.; Scheewe, T.W.; De Hert, M. Metabolic syndrome and metabolic abnormalities in patients with major depressive disorder: A meta-analysis of prevalences and moderating variables. Psychol. Med. 2014, 44, 2017–2028. [Google Scholar] [CrossRef]
- Vancampfort, D.; Correll, C.U.; Galling, B.; Probst, M.; De Hert, M.; Ward, P.B.; Rosenbaum, S.; Gaughran, F.; Lally, J.; Stubbs, B. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: A systematic review and large scale meta-analysis. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2016, 15, 166–174. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, S.; Tiedemann, A.; Sherrington, C.; Curtis, J.; Ward, P.B. Physical activity interventions for people with mental illness: A systematic review and meta-analysis. J. Clin. Psychiatry 2014, 75, 964–974. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Rosenbaum, S.; Richards, J.; Ward, P.B.; Stubbs, B. Exercise improves physical and psychological quality of life in people with depression: A meta-analysis including the evaluation of control group response. Psychiatry Res. 2016, 241, 47–54. [Google Scholar] [CrossRef] [Green Version]
- de Salles, B.F.; Simão, R.; Miranda, F.; da Silva Novaes, J.; Lemos, A.; Willardson, J.M. Rest Interval between Sets in Strength Training. Sports Med. 2009, 39, 765–777. [Google Scholar] [CrossRef]
- Meyer, J.; Schuch, F.B. Chapter 1—Exercise for the Prevention and Treatment of Depression. In Exercise-Based Interventions for Mental Illness; Stubbs, B., Rosenbaum, S., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 1–18. [Google Scholar] [CrossRef]
- Carneiro, L.S.F.; Mota, M.P.; Vieira-Coelho, M.A.; Rosenbaum, S.; Fonseca, A.M.; Vasconcelos-Raposo, J. Exercise for adults with depressive symptoms: Beyond the weight loss paradigm. Psychiatry Res. 2016, 246, 364–365. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Ward, P.B.; Teasdale, S.; Rosenbaum, S. Why moving more should be promoted for severe mental illness. Lancet Psychiatry 2015, 2, 295. [Google Scholar] [CrossRef]
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef]
- Patel, V.; Burns, J.K.; Dhingra, M.; Tarver, L.; Kohrt, B.A.; Lund, C. Income inequality and depression: A systematic review and meta-analysis of the association and a scoping review of mechanisms. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2018, 17, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Yuma-Guerrero, P.J.; Cubbin, C.; von Sternberg, K. Neighborhood Social Cohesion as a Mediator of Neighborhood Conditions on Mothers’ Engagement in Physical Activity: Results From the Geographic Research on Wellbeing Study. Health Educ. Behav. 2017, 44, 845–856. [Google Scholar] [CrossRef] [PubMed]
- Richards, E.A.; McDonough, M.; Fu, R. Longitudinal examination of social and environmental influences on motivation for physical activity. Appl. Nurs. Res. 2017, 37, 36–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamm, H.; Lamprecht, M. Structural and cultural factors influencing physical activity in Switzerland. J. Public Health 2005, 13, 203–211. [Google Scholar] [CrossRef]
- Jaeschke, L.; Steinbrecher, A.; Luzak, A.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; et al. Socio-cultural determinants of physical activity across the life course: A ‘Determinants of Diet and Physical Activity’ (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 173. [Google Scholar] [CrossRef] [Green Version]
- Juhasz, G.; Eszlari, N.; Pap, D.; Gonda, X. Cultural differences in the development and characteristics of depression. Neuropsychopharmacol. Hung 2012, 14, 259–265. [Google Scholar]
- Bird, S.P.; Tarpenning, K.M.; Marino, F.E. Designing resistance training programmes to enhance muscular fitness: A review of the acute programme variables. Sports Med. 2005, 35, 841–851. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Population and Clinical Information | Groups | Adherence to Intervention | Primary Outcomes | Secondary Outcomes | Main Findings |
|---|---|---|---|---|---|---|
| Krogh et al. [37] | Randomized trial with patients diagnosed with unipolar depression according to ICD 10th revision. A total of 165 patients (122 women, 43 men) 18–55 years-old allocated to supervised training groups (3 to 10 participants per group). Exclusion criteria: suspected of psychotic symptoms, more than 1 h of sports per week, ongoing alcohol or substance abuse, considered at risk of suicide, poor Danish language skills, medical contraindications for exercise or patients having been on sickness leave for more than 24 consecutive months. A 4-month intervention with 12-month follow-up. | Resistance training (n = 55) and 46 at 12-month follow-up. Aerobic training (n = 55) and 46 at 12-month follow-up. Relaxation training (n = 55) and 37 at 12-month follow-up. | RT—Average 18.0 sessions out of 32 (56.2%). AT—Average 16.2 sessions out of 32 (50.6%). RT—Average 10.5 sessions out of 32 (32.8%). | 17-item Hamilton Rating Scale for Depression (HAM-D17). Additional scales were used, but HAM-D17 was considered the main one by the authors. | Physical outcomes: 1RM in chest press, knee extension and leg press. Maximal oxygen uptake in cycle ergometer. Psychosocial outcomes Quality of life (WHO-5 Well-Being Index). Percentage of days absent from work during the last 10 working days (evaluated at four and 12 months) and other work-related information Cognitive abilities: Digit Span Test, Subtracting Serial Sevens, Trail Making Test, Digit Symbol Test, S phonemic fluency and verbal fluency test for animals, Buschke Test, Rey Complex Figure Test. | Exercise did not change primary outcomes, but RT reduced absences to work. RT group improved in 1RM chest press, while AT group improved in maximal oxygen uptake. No effect on cognitive abilities. |
| Moraes et al. [38] | Randomized trial with three exercise groups as adjunct treatments to pharmacotherapy (antidepressants and anxiolytics) for 25 persons diagnosed with major depressive disorder (MDD) according to DSM-IV, not engaged in physical exercise outside of the treatment setting. Patients were over 60 years old and sedentary for more than 3 months. Exclusion criteria: psychiatric comorbidities, score >18 points in HAM-D, score <24 on the Mini-Mental State Examination, cerebrovascular infarction, neurodegenerative disease, severe cardiovascular disease, illiteracy, poor mobility, balance disorders, and severe deficits in visual and/or auditory function. A 12-week intervention. | Resistance training (n = 9). Aerobic training (n = 9). Low intensity exercise control (n = 7). | All patients had a minimum of 75% attendance rate. | Hamilton Rating Scale for Depression (HAM-D17). Beck Depression Inventory (BDI), validated Portuguese translation. | None. | RT and AT groups showed significant reductions in depressive symptoms in both scales compared to controls, therefore improving upon the efficacy of pharmacological treatment only. |
| Sims et al. [39] | Randomized controlled trial with 45 stroke survivor patients (27 men and 18 women, 67.13 ± 15.23 years old) diagnosed with depressive symptoms using Prime-MD® Patient Health Questionnaire-9 (PHQ-9) and confirmed by psychiatric assessment. A 10-week intervention with a follow-up at 6 months. Exclusion criteria: stroke <6 months before the study, inability to walk ≥20 m independently (with or without a gait assistive device), <18 years-old, PHQ-9 score <5, depression with psychotic features, alcohol or drug-related depression, schizophrenia, bipolar disorder, other psychiatric diagnoses, suicidal ideation, dementia, terminal disease, uncontrolled hypertension, unstable insulin-dependent diabetes and unstable angina. | Resistance training (n = 23). Waiting list comparison control (n = 22). | Average 75% adherence to the sessions. | Centre for Epidemiologic Studies for Depression Scale (CES-D). | Physical outcomes: 1RM for seated chest and leg press. Psychosocial outcomes: Assessment of Quality of Life Instrument (AQoL), Short Form-12 Health Survey Questionnaire (SF-12), Stroke Impact Scale (SIS) 3.0, Satisfaction with Life Scale (SWLS), Social Support Survey (SSS), Life Orientation Test-Revised (LOT-R), Self-Esteem Scale (Rosenberg, 1965), Recovery Locus of Control Scale (RLOC). | Authors report the RT group had lower depression scores after the intervention, but not at the 6-month follow-up. However, the RT group already had much lower depression scores at baseline. RT group improved significantly in strength, but ultimately there were no significant changes in CES-D from pre- to post or at follow-up. |
| Singh et al. [40] | Randomized controlled trial with 60 adults (33 women and 27 men, >60 years old) with major or minor depression or dysthymia, determined through DSM-IV, and who also had GDS score ≥14. Exclusion criteria: dementia, Folstein Mini-Mental State Examination score ≤23, medical contraindications for exercise, bipolar disorder, active psychosis, perceived suicidal tendencies, currently seeing a psychiatrist, prescribed antidepressant drugs in the previous 3 months, or participating in any exercise training more than twice a week.An 8-week intervention. | High intensity RT (n = 20). Eighteen completed the study. Low intensity RT (n = 20). Seventeen completed the study. Controls (n = 20). Nineteen completed the study. | There were six drop-outs. Of those who completed the study, adherence rates were >95%. | HAM-D17. GDS. | Physical outcomes: 1RM chest press, upright row, shoulder press, leg press, knee extension and knee flexion. Psychosocial outcomes: Eysenck Personality Questionnaire (EPQ) or EPQ-Revised, Wenger Social Support Network Instrument, Self-Efficacy Scale of Sherer, Multidimensional Health Locus of Control, Medical Outcomes Survey (Short Form 36), Pittsburgh Sleep Quality Index. | A 50% reduction in HAM-D in 61% of subjects of the high intensity RT group, 29% of the low intensity group and 21% of the controls. Strength gains were associated with a reduction in depressive symptoms. The high-intensity group had a superior decline in depressive symptoms and increases in quality of life. |
| Study | W | S/w | Training Modality | WV (Min) | Exercises (n) | Sets (n) | Reps (n) | Intensity/Load (RM) | Rest Between Sets (Min) |
|---|---|---|---|---|---|---|---|---|---|
| Krogh et al. [37] | 16 | 2 | Circuit-training with machines, free weights and sandbags | 90 | 10 (of which 6 were with machines) | 2–3 | 1st phase: 12 2nd phase: 10 3rd phase: 8 | 1st: 50% 1RM 2nd: 75% 1RM 3rd: 75% 1RM | NR |
| Moraes et al. [38] | 12 | 2 | Machines | 30 | 4 | 3 | 8–12 | 70% 1RM | NR |
| Sims et al. [39] | 10 | 2 | Machines | NR | 6 | 3 | 8–10 | 80% 1RM | NR |
| Singh et al. [40] | 8 | 3 | High intensity and machines | 60 | 6 | 3 | 8 | 80% 1RM | NR |
| 8 | 3 | Low intensity and machines | 60 | 6 | 3 | 8 | 20% 1RM | NR |
| Study | W | S/w | Training Modality | WV (Min) | Exercises (n) | Sets (n) | Reps (n) | Intensity/Load (RM) | Rest Between Exercises (Min) |
|---|---|---|---|---|---|---|---|---|---|
| Krogh et al. [37] | 16 | 2 | Aerobic training group: using machines, small carpets, trampoline, step bench, jump rope and Ski Fitter (Fitter International; Calgary, Alberta, Canada). | 90 | 10 (of which 5 with machines) | 2 | 1st phase: 2 min. Gradual increase to 3 min. | 1st phase: 70% maximal HR. Gradual increase up to 89% maximal HR. | 1st phase: 2 min. Gradual decrease to 1 min. |
| 16 | 2 | Relaxation group: 20–30 min for exercises on mattresses or Bobath balls (Ledregomma; Udine, Italy) or back massage using Ball Stick Ball (Select; Glostrup, Denmark). 10–20 min of light balance exercises. 20–30 min of relaxation exercises with alternating muscle contraction and relaxation while lying down. | 50–80 | NR | NR | NR | <12 on the Borg scale. | NR | |
| Moraes et al. [38] | 12 | 2 | Aerobic training group on stationary bikes or treadmills. | 30 | 1 | 1 | 1 | 60% VO2max or 70% HRmax. | — |
| 12 | 2 | Low-intensity control group: 5 min low-intensity walking or cycling ±15 min resistance training with minimum load±10 min stretching | 30 | 8 | 1 | 1 | Minimum possible | — |
| Study | Group | N | Age | Pre (Mean) | Pre (SD) | Post (Mean) | Post (SD) | % Change (Pre-Post) | Follow-Up Test (Mean) | Follow-Up Test (SD) | % Change (Post Follow-Up) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Krogh et al. [37] | RT HAM-D17 | 46 | 41.9 ± 8.7 | 18.2 | 3.6 | 10.0 | 6.4 | −45.1 | 11.0 | 7.1 | 10.0 |
| AT HAM-D17 | 46 | 38.1 ± 9.0 | 18.2 | 3.8 | 12.1 | 6.4 | −33.5 | 11.9 | 6.5 | −1.7 | |
| Relaxation HAM-D17 | 37 | 36.7 ± 8.7 | 16.7 | 3.8 | 10.6 | 5.6 | −36.5 | 10.0 | 5.6 | −5.7 | |
| Moraes et al. [38] | RT HAM-D | 9 | 72.9 ± 7.1 | 13.4 | 3.5 | 8.6 | 2.9 | −35.8 | — | — | — |
| BDI | 25.6 | 9.1 | 12.9 | 4.9 | −49.6 | — | — | — | |||
| AT HAM-D | 9 | 70.9 ± 5.9 | 14.3 | 2.82 | 7.4 | 2.1 | −48.3 | — | — | — | |
| BDI | 19.7 | 6.44 | 12.8 | 3.6 | −35.0 | — | — | — | |||
| LI-control HAM-D | 7 | 69.3 ± 5.3 | 14.6 | 1.81 | 13.4 | 2.1 | −8.2 | — | — | — | |
| BDI | 20.4 | 3.33 | 16.9 | 3.6 | −17.2 | — | — | — | |||
| Sims et al. [39] | RT CES-D | 23 | 68.0 ± 14.8 | 15.4 | 7.49 | 15.1 | 8.5 | −1.9 | 13.8 | 8.0 | −8.6 |
| Control CES-D | 22 | 66.3 ± 16.0 | 23.3 | 8.9 | 20.6 | 11.8 | −11.6 | 22.7 | 11.2 | 10.2 | |
| Singh et al. [40] | HI RT HAM-D | 18 | 69.0 ± 5.0 | 18.0 | 4.5 | 8.5 | 5.5 | −52.8 | — | — | — |
| GDS | 20.0 | 4.1 | 8.4 | 7.0 | −58.0 | — | — | — | |||
| LI RT HAM-D | 17 | 70.0 ± 7.0 | 19.5 | 5.3 | 12.4 | 6.3 | −36.4 | — | — | — | |
| GDS | 22.0 | 4.3 | 13.3 | 7.0 | −39.5 | — | — | — | |||
| Control HAM-D | 19 | 69.0 ± 7.0 | 19.7 | 3.9 | 14.4 | 6.0 | −26.9 | — | — | — | |
| GDS | 18.7 | 3.5 | 14.0 | 5.2 | −25.1 | — | — | — |
| Cochrane RoB 2 | Krogh et al. [37] | Moraes et al. [38] | Sims et al. [39] | Singh et al. [40] |
|---|---|---|---|---|
| 1. Bias arising from the randomization process | Low | Some concerns | Some concerns | Low |
| 2. Bias due to deviations from intended interventions (effect of assignment to intervention) | Low | Low | Low | Low |
| 2. Bias due to deviations from intended interventions (effect of adhering to intervention) | High | Low | Low | Low |
| 3. Bias due to missing outcome data | Low | Low | Low | Low |
| 4. Bias in measurement of the outcome | Low | Some concerns | Some concerns | Some concerns |
| 5. Bias in selection of the reported result | Low | Low | Low | Low |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carneiro, L.; Afonso, J.; Ramirez-Campillo, R.; Murawska-Ciałowciz, E.; Marques, A.; Clemente, F.M. The Effects of Exclusively Resistance Training-Based Supervised Programs in People with Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2020, 17, 6715. https://doi.org/10.3390/ijerph17186715
Carneiro L, Afonso J, Ramirez-Campillo R, Murawska-Ciałowciz E, Marques A, Clemente FM. The Effects of Exclusively Resistance Training-Based Supervised Programs in People with Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2020; 17(18):6715. https://doi.org/10.3390/ijerph17186715
Chicago/Turabian StyleCarneiro, Lara, José Afonso, Rodrigo Ramirez-Campillo, Eugenia Murawska-Ciałowciz, Adilson Marques, and Filipe Manuel Clemente. 2020. "The Effects of Exclusively Resistance Training-Based Supervised Programs in People with Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 17, no. 18: 6715. https://doi.org/10.3390/ijerph17186715
APA StyleCarneiro, L., Afonso, J., Ramirez-Campillo, R., Murawska-Ciałowciz, E., Marques, A., & Clemente, F. M. (2020). The Effects of Exclusively Resistance Training-Based Supervised Programs in People with Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 17(18), 6715. https://doi.org/10.3390/ijerph17186715