Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents

 and
and 
Abstract
1. Introduction
2. Materials and Methods
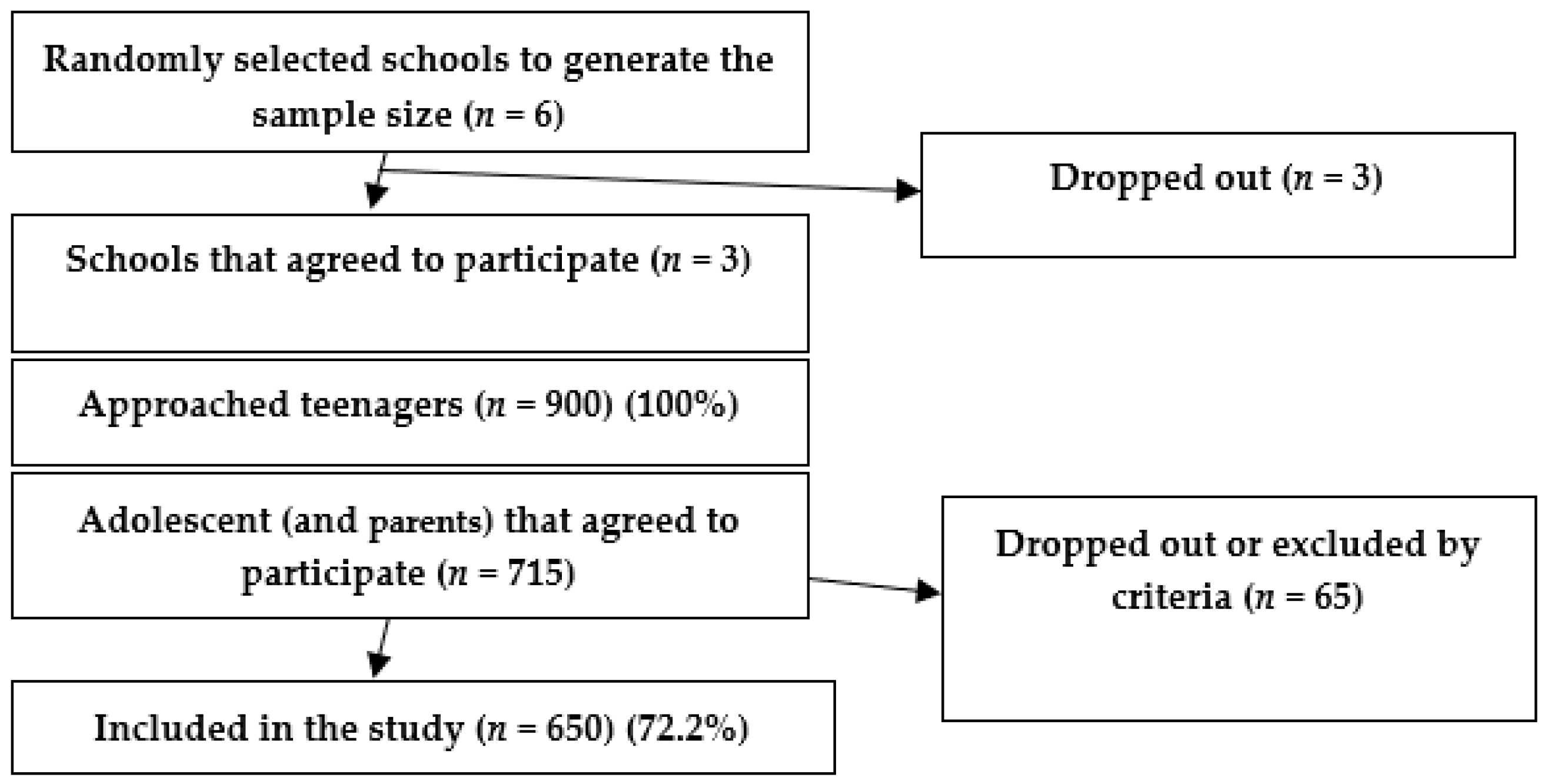
2.1. Study Design and Population
2.2. Data Collection
- (1)
- The oral clinical examination was performed by a single dentist examiner that underwent a calibration procedure following the WHO guidelines in order to have a uniform understanding and application of the International Caries Detection and Assessment System. Duplicate examinations were performed on 10% of the evaluated adolescents (n = 65). The kappa statistic was used to assess intra-examiner reproducibility. A trained dental nurse recorded the results of the clinical examinations performed by the dentist.
- (2)
- The research team applied a structured original questionnaire to the participants in the study, consisting of two subsections: (a) a dental behavior section and (b) a validated food frequency questionnaire (FFQ). The dental behavior section comprised questions used in previous studies [13]. The FFQ is part of a valid questionnaire adapted to Romanian habits (EPIC Norfolk) [14]. The questionnaire was pretested and re-tested on a sample of 30 subjects. Spearman’s correlation coefficient was used to assess the reliability (r = 0.763). The time necessary to fill in the survey questionnaire was 25 min.
- (a)
- The dental behavior questionnaire section investigated: (1) the tooth brushing frequency, (2) evening tooth brushing, (3) dental visit frequency, and (4) external fluoridation (use of fluoridated toothpaste), as different frequencies (Table 1).
- (b)
- In the FFQ section, we assessed the food and beverages intake habits as different frequencies: never or less than 1/month, 1–3 times/month, once/week, 2–4 times/week, 5–6 times /week, once/day, 2–3 times/day, 4–5 times/day, more than six times/day. We estimated the type of different sugary foods as mentioned in the EPIC food frequency questionnaire sweets and snacks category that, for simplicity, we consolidated the categories as follows: (a) Chocolate (chocolates, single or squares, chocolate snack bars, e.g., Mars, Crunchy, cocoa, hot chocolate); (b) cakes, ice-cream, biscuits (sweet biscuits, chocolate, e.g., digestive plain, e.g., Nice, ginger, cakes, e.g., fruit, sponge, home baked/ready-made, buns, pastries, e.g., scores, lap jacks, croissants, doughnuts, fruit pies, tarts, crumbles, sponge puddings, home baked or ready-made, milk puddings, e.g., rice, custard, trifle, ice cream, choc ices); (c) sugar and candies (sweets, toffees, mints); (d) jams and syrups (jam, marmalade, honey, syrups); (e) sugary sweetened beverages (SSB’s) respectively sodas (fizzy soft drinks, e.g., Coca Cola, Sprite, Fanta, etc., lemonade); (f) added sugar (to tea, coffee, to peanuts or other nuts). In order to perform the multivariate linear regression analyses, we stratified the results into two categories—adolescents who never or less frequently, consumed these sweets and frequently.
2.3. Statistics
3. Results
3.1. Demographics of the Studied Group
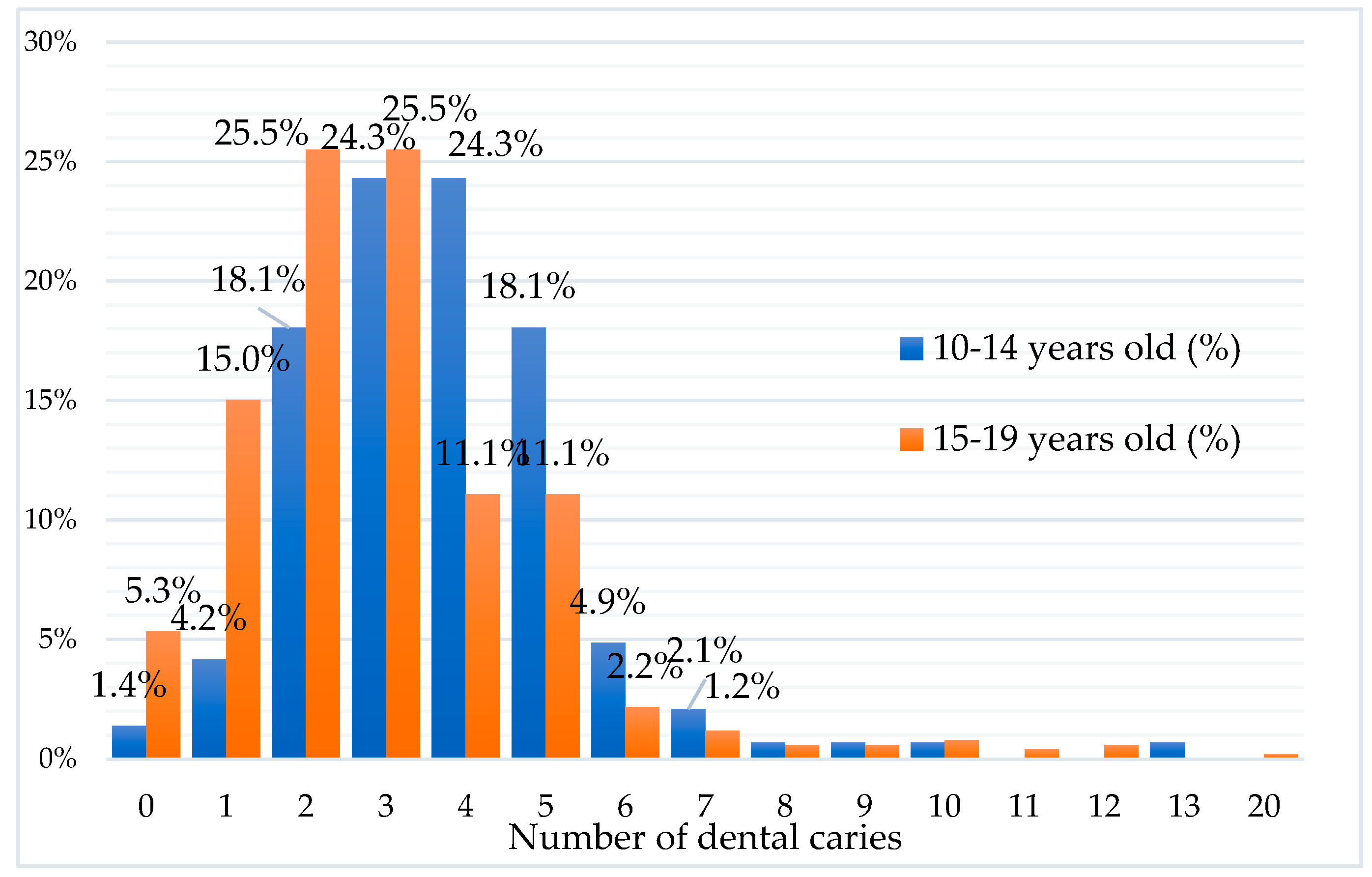
3.2. Caries Prevalence
3.3. Dental Hygiene Behavior
3.4. Food Behavior
3.5. Lifestyle Factors Predicting the DMFT Index
4. Discussion
5. Limitations
6. Strengths
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DMFT | Decayed, Missing, and Filled teeth index |
| EU | European Union |
| FDI | Federation Dentaire Internationale |
| SSB’s | Sugar-sweetened beverages |
| WHO | World Health Organization |
| EPIC Norfolk | European Prospective Investigation into Cancer—Norfolk |
| FFQ | Food Frequency Questionnaire |
References
- Obregón, N.-R.; Fernández-Riveiro, P.; Piñeiro-Lamas, M.; Smyth, E.-C.; Montes, A.-M.; Suarez, M.M.-C. Prevalence and caries-related risk factors in schoolchildren of 12- and 15-year-old: A cross-sectional study. BMC Oral Health 2019, 19, 120. [Google Scholar] [CrossRef]
- Eriksson, L.; Holgerson, P.L.; Johansson, I. Saliva and tooth biofilm bacterial microbiota in adolescents in a low caries community. Sci. Rep. 2017, 7, 5861. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E. Socio behavioral risk factors in dental caries – international perspectives. Commun. Dent. Oral Epidemiol. 2005, 33, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Frazão, P. Epidemiology of dental caries: When structure and context matter. Braz. Oral Res. 2012, 26, 108–114. [Google Scholar] [CrossRef]
- Watt, R.G.; Rouxel, P. Dental caries, sugars, and food policy. Arch. Dis. Child. 2012, 97, 769–772. [Google Scholar] [CrossRef]
- Touger-Decker, R.; van Loveren, C. Sugars and dental caries. AJCN 2003, 78, 881–892. [Google Scholar] [CrossRef]
- Gibson, S.; Williams, S. Dental caries in pre-school children: Associations with social class, tooth brushing habit, and consumption of sugars and sugar-containing foods. Caries Res. 1999, 33, 101–113. [Google Scholar] [CrossRef]
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Program. Commun. Dent. Oral Epidemiol. 2003, 31 (Suppl. 1), 3–24. [Google Scholar] [CrossRef]
- Al-Darwish, M.; El Ansari, W.; Bener, A. Prevalence of dental caries among 12–14-year-old children in Qatar. Saudi Dent. J. 2014, 26, 115–125. [Google Scholar] [CrossRef]
- Petersen, P.E.; Danila, I.; Samoila, A. Oral health behavior, knowledge, and attitudes of children, mothers, and schoolteachers in Romania in 1993. Acta Odontol. Scand. 1995, 53, 363–368. [Google Scholar] [CrossRef]
- Moynihan, P. Sugars and Dental Caries: Evidence for Setting a Recommended Threshold for Intake. Adv. Nutr. 2016, 7, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Patel, R. The State of Oral Health in Europe-Report Commissioned by the Platform for Better Oral Health in Europe. 2012. Available online: http://www.mah.se/PageFiles/49503/Report (accessed on 21 September 2020).
- Akarslan, Z.Z.; Sadık, B.; Sadık, E.; Hülya Erten, H. Dietary habits and oral health-related behaviors in relation to DMFT indexes of a group of young adult patients attending a dental school. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, 800–807. [Google Scholar]
- European Prospective Investigation of Cancer (EPIC). Available online: https://www.epic-norfolk.org.uk/epicffq/EPIC_HC3_FFQ_V6_OCR_Uncoded.pdf (accessed on 21 September 2020).
- Schiffner, U.; Hoffmann, T.; Kerschbaum, T.; Micheelis, W. Oral health in German children, adolescents, adults and senior citizens in 2005. Commun. Dent. Health 2009, 26, 18. [Google Scholar]
- Mamai-Homata, E.; Koletsi-Kounari, H.; Margaritis, V. Gender differences in oral health status and behavior of Greek dental students: A meta-analysis of 1981, 2000, and 2010 data. J. Int. Soc. Prev. Commun. Dent. 2016, 6, 60–68. [Google Scholar] [CrossRef]
- Hobdell, M.; Petersen, P.E.; Clarkson, J.; Johnson, N. Global goals for oral health 2020. Int. Dent. J. 2003, 53, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Laganà, G.; Abazi, Y.; Beshiri Nastasi, E.; Vinjolli, F.; Fabi, F.; Divizia, M.; Cozza, P. Oral health conditions in an Albanian adolescent population: An epidemiological study. BMC Oral Health 2015, 15, 67. [Google Scholar] [CrossRef] [PubMed]
- Baciu, D.; Danila, I.; Balcos, C.; Gallagher, J.E.; Bernabe, E. Caries experience among Romanian schoolchildren: Prevalence and trends 1992–2011. Commun. Dent. Health 2015, 32, 93–97. [Google Scholar]
- Žemaitienė, M.; Grigalauskienė, R.; Vasiliauskienė, I.; Saldūnaitė, K.; Razmienė, J.; Slabšinskienė, E. Prevalence and severity of dental caries among 18-year-old Lithuanian adolescents. Medicina. 2016, 52, 54–60. [Google Scholar] [CrossRef]
- Veiga, N.; Pereira, C.; Amaral, O. Prevalence and determinants of dental caries in a sample of schoolchildren of Sátão, Portugal. Rev. Port. Estomatol. Med. Dent. Cir. Maxilofac. 2014, 55, 214–219. [Google Scholar]
- Reisine, S.T.; Psoter, W. Socioeconomic status and selected behavioral determinants as risk factors for dental caries. J. Dent. Educ. 2001, 65, 1009–1016. [Google Scholar] [CrossRef]
- Ferraro, M.; Vieira, A.R. Explaining gender differences in caries: A multifactorial approach to a multifactorial disease. Int. J. Dent. 2010, 2010, 649643. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Jiang, W.; Lin, X.; Zhu, H.; Zhou, N.; Chen, Y.; Wu, W.; Zhang, D.; Chen, H. Dental Caries Status and Caries Risk Factors in Students Ages 12–14 Years in Zhejiang. China Med. Sci. Monit. 2018, 24, 3670–3678. [Google Scholar] [CrossRef] [PubMed]
- Anopa, Y.; McMahon, A.D.; Conway, D.I.; Ball, G.E.; McIntosh, E.; Macpherson, L.M.D. Improving child oral health: Cost analysis of a national nursery tooth brushing programme. PLoS ONE 2015, 10, e0136211. [Google Scholar] [CrossRef]
- Hysi, D.; Eaton, K.A.; Vassallo, P.; Tsakos, G. Proceedings of a workshop, held in Constanta, Romania, 22 May 2014 on Oral Health of Children in the Central and Eastern European Countries in the Context of the Current Economic Crisis. In BMC Oral Health; BioMed Central: London, UK, 2014; p. 69. [Google Scholar] [CrossRef]
- Fleming, E.; Afful, J. Prevalence of Total and Untreated Dental Caries Among Youth: United States, 2015–2016; National Center for Health Statistics: Hyattsville, MD, USA, 2018.
- Park, J.B.; Han, K.; Park, Y.G.; Ko, Y. Association between socioeconomic status and oral health behaviors: The 2008-2010 Korea national health and nutrition examination survey. Exp. Ther. Med. 2016, 12, 2657–2664. [Google Scholar] [CrossRef] [PubMed]
- Paula, J.S.; Ambrosano, G.M.; Mialhe, F.L. The impact of social determinants on school children’;s oral health. Brazil. Braz. Oral Res. 2015, 29, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Duggal, M.S.; Toumba, K.J.; Amaechi, B.T.; Kowash, M.B.; Higham, S.M. Enamel demineralization in situ with various frequencies of carbohydrate consumption with and without fluoride toothpaste. J. Dent. Res. 2001, 80, 1721–1724. [Google Scholar] [CrossRef]
- Shaffer, J.R.; Leslie, E.J.; Feingold, E.; Govil, M.; McNeil, D.W.; Crout, R.J.; Weyant, R.J.; Marazita, M.L. Caries Experience Differs between Females and Males across Age Groups in Northern Appalachia. Int. J. Dent. 2015, 938213. [Google Scholar] [CrossRef]
- Cheng, R.; Yang, H.; Shao, M.Y.; Hu, T.; Zhou, X.D. Dental erosion and severe tooth decay related to soft drinks: A case report and literature review. J. Zhejiang Univ. Sci. B 2009, 10, 395–399. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef]
- Verzeletti, C.; Maes, L.; Santinello, M.; Vereecken, C. Soft drink consumption in adolescent: Associations with food-related lifestyles and family rules in Belgium Flanders and the Veneto Region of Italy. Eur. J. Public Health. 2009, 20, 312–317. [Google Scholar] [CrossRef]
- Sdrali, D.; Anisiadou, M.; Goussia-Rizou, M.; Costarelli, V. Adolescents’ soft drinks consumption in family environment: A case study in Northern Greece. Int. J. Consum Stud. 2010, 34, 684–690. [Google Scholar] [CrossRef]
- Singh, G.M. Soda Consumption among Adolescents: Implications for Low- and Middle-Income Countries. Am. J. Public Health. 2017, 107, 1025–1027. [Google Scholar] [CrossRef] [PubMed]
- Yu Yon, M.J.; Gao, S.S.; Chen, K.J.; Duangthip, D.; Man Lo, E.C.; Chu, C.H. Medical Models in caries Management. Dent. J. 2019, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Bernabé, E.; Sheiham, A. Age, period and cohort trends in caries of permanent teeth in four developed countries. Am. J. Public Health. 2014, 104, 115–121. [Google Scholar] [CrossRef]
- Graça, S.R.; Albuquerque, T.S.; Luis, H.S.; Assuncao, V.A.; Malmqvist, S.; Cuculescu, M.; Slusanschi, O.; Johannsen, G.; Galuscan, A.; Podariu, A.C.; et al. Oral health knowledge, perceptions, and habits of adolescents from Portugal, Romania, and Sweden: A comparative study. J. Int. Soc. Prev. Commun. Dent. 2019, 9, 470. [Google Scholar] [CrossRef]
- Lucaciu, P.O.; Mester, A.; Constantin, I.; Orban, N.; Cosma, L.; Candrea, S.; Mesaros, A.S. A WHO Pathfinder Survey of Dental Caries in 6 and 12-Year Old Transylvanian Children and the Possible Correlation with Their Family Background, Oral-Health Behavior, and the Intake of Sweets. Int. J. Environ. Res. Public Health 2020, 17, 4180. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Dental Hygiene Variable/Frequency | Total (No./%) | Males (No./%) | Females (No./%) | p |
|---|---|---|---|---|
| Tooth brushing frequency | ||||
| Twice/day | 507 (78.0%) | 95 (65.1%) | 412 (81.7%) | <0.001 |
| Less than once/day or “sometimes I forgot” | 143 (22.0 %) | 51 (34.9%) | 92 (18.3%) | |
| Evening tooth brushing frequency | ||||
| Every evening | 431 (66.3%) | 89 (60.9%) | 342 (67.8%) | 0.140 |
| Rare/not at all | 219 (33.7%) | 57 (39.1 %) | 162 (32.2%) | |
| Dental visit frequency | ||||
| 1–2 times/year | 386 (59.4%) | 82 (56.2%) | 304 (60.3%) | 0.420 |
| In pain/not at all | 264 (40. 6%) | 64 (43.8%) | 200 (39.7%) | |
| Fluoridated toothpaste use | ||||
| With fluoride | 489 (75.2%) | 97 (66.4%) | 392 (77.8%) | <0.001 |
| Without fluoride | 161 (24.8%) | 49 (33.6%) | 112 (22.2%) | |
| Hygiene Behaviors Variable | DMFT (Mean ± SD) | p |
|---|---|---|
| Teeth brushing frequency | ||
| Twice/day | 3.1 ± 1.9 | <0.814 |
| Less than once/day or “sometimes I forgot” | 3.2 ± 2.1 | |
| Evening tooth brushing frequency | ||
| Rare/never | 3.2 ± 2.2 | 0.770 |
| Frequent | 3.1 ± 1.9 | |
| Dental visit frequency | ||
| 1–2 times per year | 3.0 ± 2.0 | 0.404 |
| In pain/ not at all | 3.1 ± 2.1 | |
| Fluoridated toothpaste use | ||
| with fluoride | 3.1 ± 1.9 | 0.055 |
| without fluoride | 3.2 ± 2.3 |
| Food Type and Frequency | Total No % | Male No % | Female No % | p |
|---|---|---|---|---|
| Chocolate | ||||
| Never/rare | 246 (37.8%) | 60 (41.1%) | 186 (36.9%) | 0.410 |
| Frequent | 404 (62.1%) | 86 (58.9%) | 318 (63.1%) | |
| Cakes, ice-cream, biscuits | ||||
| Never/rare | 405 (62.3%) | 87 (59.6%) | 318 (63.1%) | 0.500 |
| Frequent | 245 (37.7%) | 59 (40.4%) | 186 (36.9%) | |
| Sugar, candies | ||||
| Never/rare | 438 (67.4%) | 99 (67.8%) | 339 (67.3%) | 0.980 |
| Frequent | 212 (32.6%) | 47 (32.2%) | 165 (32.7%) | |
| Jams and syrup | ||||
| Never/rare | 465 (71.4%) | 96 (65.7%) | 369 (73.2%) | 0.090 |
| Frequent | 185 (28.6%) | 50 (34.2%) | 135 (26.7%) | |
| Sugary sweetened beverages (SSB’s) (sodas) | ||||
| Never/rare | 419 (64.5%) | 80 (54.8%) | 339 (67.3%) | <0.001 |
| Frequent | 231 (35.5%) | 66 (45.2%) | 165 (32.7%) | |
| Added Sugar | ||||
| Never/rare | 228 (35.1%) | 62 (42.5%) | 166 (32.9%) | 0.170 |
| Frequent | 422 (64.9%) | 84 (57.5%) | 338 (67.1%) | |
| Sugary Food Consumption | DMFT Index (Mean) | ±SD | p |
|---|---|---|---|
| Chocolate | |||
| Frequent | 3.2 | ±2.1 | 0.610 |
| Never/rare | 3.06 | ±1.9 | |
| Cakes, ice-cream, biscuits | |||
| Frequent | 3.2 | ±1.9 | 0.220 |
| Never/rare | 3.1 | ±2.1 | |
| Sugar candies | |||
| Frequent | 3.2 | ±2.0 | 0.164 |
| Never/rare | 3.1 | ±2.1 | |
| Jams syrups | |||
| Frequent | 3.5 | ±2.3 | 0.004 |
| Never/rare | 3.0 | ±1.9 | |
| Sugary sweetened beverages SSB’s (sodas) | |||
| Frequent | 3.1 | ±1.8 | 0.414 |
| Never/rare | 3.1 | ±2.2 | |
| Added Sugar | |||
| Frequent | 3.1 | ±1.4 | 0.012 |
| Never/rare | 2.6 | ±1.7 |
| Independent Variable | B | ±Standard Error (SE) | Beta | t | p |
|---|---|---|---|---|---|
| (Constant) | 4.04 | 0.63 | 6.46 | 0.000 | |
| Residence (urban/rural) | −0.11 | 0.41 | −0.02 | −0.26 | 0.790 |
| Age | 0.84 | 0.38 | 0.17 | 2.21 | 0.020 |
| Gender | 0.13 | 0.39 | 0.03 | 0.32 | 0.750 |
| Father education | 0.22 | 0.37 | 0.04 | 0.59 | 0.560 |
| Mother education | −0.54 | 0.40 | −0.10 | −1.3 | 0.180 |
| Dental behavior | |||||
| Teeth brushing frequency | −0.23 | 0.36 | −0.04 | −0.65 | 0.520 |
| Dentist visit frequency | −0.30 | 0.35 | −0.06 | 0.86 | 0.040 |
| Toothpaste | 0.05 | 0.37 | 0.01 | 0.15 | 0.880 |
| Eating behavior | |||||
| Sodas (SSB’s) | 0.91 | 0.41 | 0.17 | −2.21 | 0.030 |
| Cakes, biscuits, ice cream | −0.37 | 0.39 | −0.07 | −0.96 | 0.340 |
| Sugar, candies | −0.48 | 0.43 | −0.09 | −1.14 | 0.260 |
| Jam, syrup | 0.63 | 0.41 | 0.12 | 1.54 | 0.120 |
| Chocolate | 0.63 | 0.38 | 0.12 | 1.66 | 0.100 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tudoroniu, C.; Popa, M.; Iacob, S.M.; Pop, A.L.; Năsui, B.A. Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6923. https://doi.org/10.3390/ijerph17186923
Tudoroniu C, Popa M, Iacob SM, Pop AL, Năsui BA. Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(18):6923. https://doi.org/10.3390/ijerph17186923
Chicago/Turabian StyleTudoroniu, Cosmin, Monica Popa, Simona Maria Iacob, Anca Lucia Pop, and Bogdana Adriana Năsui. 2020. "Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents" International Journal of Environmental Research and Public Health 17, no. 18: 6923. https://doi.org/10.3390/ijerph17186923
APA StyleTudoroniu, C., Popa, M., Iacob, S. M., Pop, A. L., & Năsui, B. A. (2020). Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents. International Journal of Environmental Research and Public Health, 17(18), 6923. https://doi.org/10.3390/ijerph17186923