Canan Outdoor Multisurface Terrain Enhance the Effects of Fall Prevention Exercise in Older Adults? A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Training Ground Design
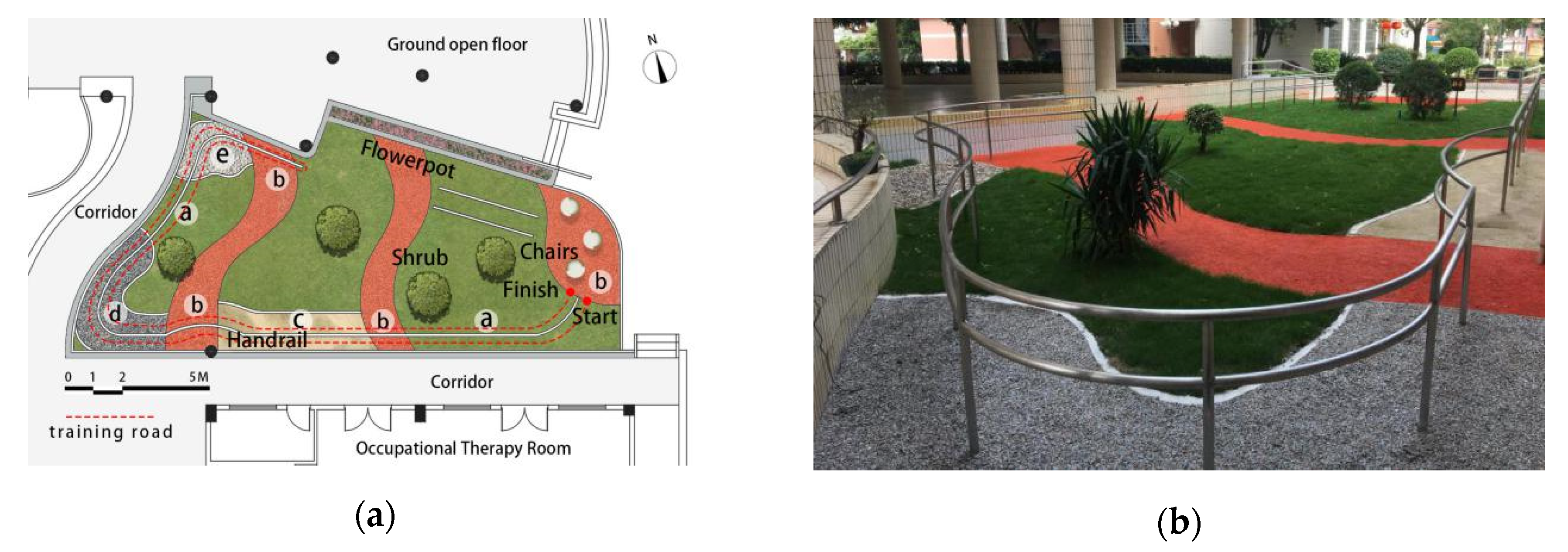
2.3.1. Outdoor Multisurface Terrain
2.3.2. Indoor Solid Ground
2.4. Intervention
2.5. Assessments
2.5.1. Measurement of Walking Ability
2.5.2. Measurement of Balance Ability
2.6. Statistical Analysis
3. Results
3.1. Changes in Walking Ability
3.2. Changes in Balance Ability
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Doucette, J.; Claus, E.; Marottoli, R. Risk factors for serious injury during falls by older persons in the community. J. Am. Geriatr. Soc. 1995, 43, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Chippendale, T.; Boltz, M. The neighborhood environment: Perceived fall risk, resources, and strategies for fall prevention. Gerontologist 2015, 55, 575–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicklett, E.J.; Lohman, M.C.; Smith, M.L. Neighborhood environment and falls among community-dwelling older adults. Int. J. Environ. Res. Public Health 2017, 14, 175. [Google Scholar] [CrossRef] [Green Version]
- Letts, L.; Moreland, J.; Richardson, J.; Coman, L.; Edwards, M.; Ginis, K.M.; Wilkins, S.; Wishart, L. The physical environment as a fall risk factor in older adults: Systematic review and meta-analysis of cross-sectional and cohort studies. Aust. Occup. Ther. J. 2010, 57, 51–64. [Google Scholar] [CrossRef]
- Li, W.; Keegan, T.H.; Sternfeld, B.; Sidney, S.; Quesenberry, C.P., Jr.; Kelsey, J.L. Outdoor Falls Among Middle-Aged and Older Adults: A Neglected Public Health Problem. Am. J. Public Health 2006, 96, 1192–1200. [Google Scholar] [CrossRef]
- Hawkins, K.A.; Clark, D.J.; Balasubramanian, C.K.; Fox, E.J. Walking on uneven terrain in healthy adults and the implications for people after stroke. NeuroRehabilitation 2017, 41, 765–774. [Google Scholar] [CrossRef] [Green Version]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Marigold, D.S.; Patla, A.E. Age-related changes in gait for multi-surface terrain. Gait Posture 2008, 27, 689–696. [Google Scholar] [CrossRef]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Age-related differences in walking stability. Age Ageing 2003, 32, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Voloshina, A.S.; Kuo, A.D.; Daley, M.A.; Ferris, D.P. Biomechanics and energetics of walking on uneven terrain. J. Exp. Biol. 2013, 216, 3963–3970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, D.J.; Rose, D.K.; Ring, S.A.; Porges, E.C. Utilization of central nervous system resources for preparation and performance of complex walking tasks in older adults. Front. Aging Neurosci. 2014, 6, 217. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, G.B.; Nitz, A.J. Dynamic ankle stability: Mechanical and neuromuscular interrelationships. J. Sport Rehab. 1994, 3, 43–57. [Google Scholar] [CrossRef]
- Hirase, T.; Inokuchi, S.; Matsusaka, N.; Okita, M. Effects of a balance training program using a foam rubber pad in community-based older adults: A randomized controlled trial. J. Geriatr. Phys. Ther. 2015, 38, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Theory and Practical Applications; Williams and Wilkins: Baltimore, MD, USA, 1995. [Google Scholar]
- Weinstein, S. Intensive and extensive aspects of tactile sensitivity as a function of body part, sex and laterality. In The Skin Senses; Kenshalo, D.R., Ed.; Charles C. Thomas Publishing: Springfield, IL, USA, 1968; pp. 195–218. [Google Scholar]
- Morioka, S.; Fujita, H.; Hiyamizu, M.; Maeoka, H.; Matsuo, A. Effects of plantar perception training on standing posture balance in the old old and the very old living in nursing facilities: A randomized controlled trial. Clin. Rehabil. 2011, 25, 1011–1020. [Google Scholar] [CrossRef]
- Kogler, K.; Howard, N.; Schumacher, M.; Knight, H. Variable Surface Training and Fall Risk in the Older Adult: A Literature Review. Top. Geriatr. Rehabil. 2018, 34, 185–193. [Google Scholar] [CrossRef]
- Means, K.M. The obstacle course: A tool for the assessment of functional balance and mobility in the elderly. J. Rehabil. Res. Dev. 1996, 33, 413–428. [Google Scholar]
- Rogers, M.E.; Rogers, N.L.; Takeshima, N.; Islam, M.M. Methods to assess and improve the physical parameters associated with fall risk in older adults. Prev. Med. 2003, 36, 255–264. [Google Scholar] [CrossRef]
- Rubenstein, L.; Josephson, K.; Trueblood, P.; Yeung, K.; Harker, J.; Robbins, A. The reliability and validity of an obstacle course as a measure of gait and balance in older adults. Aging Clin. Exp. Res. 1997, 9, 127–135. [Google Scholar] [CrossRef]
- Held, S.L.; Kott, K.M.; Young, B.L. Standardized Walking Obstacle Course (SWOC): Reliability and validity of a new functional measurement tool for children. Pediatr. Phys. Ther. 2006, 18, 23–30. [Google Scholar] [CrossRef]
- Morat, T.; Kroeger, D.; Mechling, H. The Multisurface Obstacle Test for older adults (MSOT): Development and reliability of a novel test for older adults. Eur. Rev. Aging Phys. Act. 2013, 10, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Rogers, M.E.; Rogers, N.L.; Chaparro, B.S.; Stumpfhauser, L.; Halcomb, C.G. Effects of modular course training on mobility in older adults aged 79–90 years. Disabil. Rehabil. 2003, 25, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Morat, T.; Mechling, H. The functional movement circle for older adults: Feasibility and effects on physical performance. Aging Clin. Exp. Res. 2014, 26, 529–537. [Google Scholar] [CrossRef]
- David, K. Healing Garden; Images Publicatin Group Pty Ltd.: Melbourne, Australia, 2016. [Google Scholar]
- Haering, M. The Use of Outdoor Environments by Occupational and Physical Therapy Staff in the Context of Patient Treatment in Rehabilitation Settings: An Exploratory Study. Master’s Thesis, Michigan State University, East Lansing, MI, USA, 2016. [Google Scholar]
- Barton, J.; Bragg, R.; Wood, C.; Pretty, J. Green Exercise: Linking Nature, Health and Well-Being; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L.J.P.T. Clinical gait assessment in the neurologically impaired: Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef]
- Era, P.; Sainio, P.; Koskinen, S.; Haavisto, P.; Vaara, M.; Aromaa, A. Postural balance in a random sample of 7979 subjects aged 30 years and over. Gerontology 2006, 52, 204–213. [Google Scholar] [CrossRef]
- Rydwik, E.; Bergland, A.; Forsen, L.; Frändin, K. Practice, Investigation into the reliability and validity of the measurement of elderly people’s clinical walking speed: A systematic review. Physiother. Theory Pract. 2012, 28, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Pin, T.W. Psychometric properties of 2-minute walk test: A systematic review. Arch. Phys. Med. Rehabil. 2014, 95, 1759–1775. [Google Scholar] [CrossRef]
- Rossier, P.; Wade, D.T. Validity and reliability comparison of 4 mobility measures in patients presenting with neurologic impairment. Arch. Phys. Med. Rehabil. 2001, 82, 9–13. [Google Scholar] [CrossRef]
- Morat, T.; Mechling, H. Training in the functional movement circle to promote strength and mobility-related activities in older adults: A randomized controlled trial. Eur. J. Ageing 2015, 12, 105–118. [Google Scholar] [CrossRef] [Green Version]
- Means, K.M.; O Sullivan, P.S. Modifying a functional obstacle course to test balance and mobility in the community. J. Rehabil. Res. Dev. 2000, 37, 621–632. [Google Scholar]
- Wall, J.C.; Bell, C.; Campbell, S.; Davis, J. The Timed Get-up-and-Go test revisited: Measurement of the component tasks. J. Rehabil. Res. Dev. 2000, 37, 109–133. [Google Scholar] [PubMed]
- Hurley, M.V.; Rees, J.; Newham, D. Quadriceps function, proprioceptive acuity and functional performance in healthy young, middle-aged and elderly subjects. Age Ageing 1998, 27, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, L.; Han, P.; Wang, J.; Ma, Y.; Jia, L.; Fu, L.; Yu, H.; Chen, X.; Niu, K.; Guo, Q. Timed Up and Go Test can predict recurrent falls: A longitudinal study of the community-dwelling elderly in China. Clin. Interv. Aging 2017, 12, 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.M.; Nasu, E.; Rogers, M.E.; Koizumi, D.; Rogers, N.L.; Takeshima, N. Effects of combined sensory and muscular training on balance in Japanese older adults. Prev. Med. 2004, 39, 1148–1155. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Gollhofer, A.; Strass, D. Training induced adaptations in characteristics of postural reflexes in elderly men. Gait Posture 2006, 24, 459–466. [Google Scholar] [CrossRef]
- Kelsey, J.L.; Berry, S.D.; Procter-Gray, E.; Quach, L.; Nguyen, U.S.D.; Li, W.; Kiel, D.P.; Lipsitz, L.A.; Hannan, M.T. Indoor and outdoor falls in older adults are different: The maintenance of balance, independent living, intellect, and Zest in the Elderly of Boston Study. J. Am. Geriatr. Soc. 2010, 58, 2135–2141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| OMTG (n =11) | ISGG (n =11) | |
|---|---|---|
| Gender (female/male) | 10/1 | 9/2 |
| Age (years) | 79.5 ± 2.1 | 80.8 ± 5.2 |
| Weight (kg) | 54.5 ± 9.9 | 53.7 ± 11.8 |
| Height (cm) | 158.7 ± 4.6 | 158.2 ± 5.7 |
| Exercise | OMTG | ISGG | |
|---|---|---|---|
| Agility training | Forward walking | One lap | Four laps |
| Backward walking | Half a lap | Two laps | |
| Sideways walking | Half a lap | Two laps | |
| Balance training | Heel-to-toe walking | Half a lap | Two laps |
| Crossover side step | Half a lap | Two laps | |
| High-knees walking | Half a lap | Two laps | |
| Strength training | Squat | Repeat 3 times with eyes open, 3 times with eyes closed; 5 sets | Repeat 5 times with eyes open, 3 times with eyes closed; 3sets |
| Single-leg squat | Repeat 3 times with eyes open, 3 times with eyes closed; 5 sets | Repeat 5 times with eyes open, 3 times with eyes closed; 3sets | |
| Moving from the heels to the toes while standing | Repeat 3 times with eyes open, 3 times with eyes closed; 5 sets | Repeat 5 times with eyes open, 3 times with eyes closed; 3sets | |
| Parameter | OMTG | ISGG | Changes from Baseline | Z | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Z | p | Pre | Post | Z | p | OMTG | ISGG | |||
| 10 mWT (m/s) | 0.87 (0.57,1.06) | 0.94 (0.64,1.09) | −2.934 | 0.003 ** | 0.84 (0.76,1.18) | 0.94 (0.81,1.18) | −2.934 | 0.003 ** | 0.08 (0.06,0.17) | 0.06 (0.06,0.1) | −1.971 | 0.049 * |
| MTWT (s) | 92.4 (63.1,126.6) | 76.9 (58.6,108.2) | −2.937 | 0.003 ** | 69 (61,81) | 63.6 (58.7,75.3) | −2.578 | 0.01 ** | −14.2 (−19,−7.4) | −5.7 (−9.7,−3.1) | −2.331 | 0.020 * |
| 2 MWT (m) | 110 (91,135) | 120 (95,136) | −2.937 | 0.003 ** | 120 (112.8,120) | 125 (115,135) | −2.047 | 0.016 * | 7 (4,10) | 6 (2,19) | −3.976 | 0.000 ** |
| TUGT (s) | 13.1 (10.7,19) | 12.9 (9.6,16.1) | −2.937 | 0.003 ** | 12.1 (8.1,13.3) | 10.6 (8.3,12.4) | −2.134 | 0.03 * | −1.1 (−3.2,−0.5) | −0.9 (−2.3,0.2) | −1.149 | 0.25 |
| SLSTEO (s) | 2.8 (1.5,5.3) | 3.7 (3.1,8.3) | −2.805 | 0.005 ** | 3.7 (3.1,9) | 4.1 (3.1,22.9) | −2.134 | 0.722 | 1.1 (0.3,3) | 0.1 (−0.6,2.7) | −1.674 | 0.094 |
| SLSTEC (s) | 2.6 (1.2,3) | 2.8 (2.5,4) | −2.934 | 0.003 ** | 2.5 (1.6,3.2) | 2.9 (2.4,3.2) | −1.423 | 0.155 | 0.7 (0.1,1.5) | 0.2 (−0.1,1.4) | −1.084 | 0.278 |
| CCT (s) | 5.6 (4.1,8) | 9.2 (5.5,11.9) | −2.934 | 0.003 ** | 7.6 (5.7,14.2) | 8.6 (5.9,16.5) | −2.223 | 0.026 * | 2.3 (1.3,8.1) | 1.1 (0.6,3.9) | −1.806 | 0.071 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, T.-Y.; Yuan, X.-M.; Ma, X.-J. Canan Outdoor Multisurface Terrain Enhance the Effects of Fall Prevention Exercise in Older Adults? A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 7023. https://doi.org/10.3390/ijerph17197023
Zhou T-Y, Yuan X-M, Ma X-J. Canan Outdoor Multisurface Terrain Enhance the Effects of Fall Prevention Exercise in Older Adults? A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(19):7023. https://doi.org/10.3390/ijerph17197023
Chicago/Turabian StyleZhou, Tong-Yue, Xiao-Mei Yuan, and Xiao-Jun Ma. 2020. "Canan Outdoor Multisurface Terrain Enhance the Effects of Fall Prevention Exercise in Older Adults? A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 19: 7023. https://doi.org/10.3390/ijerph17197023