Usability of Clinical Information in Discharge Summary Data in the Diagnosis Procedure Combination Survey for Cancer Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Data Analysis
2.3. Ethical Considerations
3. Results
3.1. Sample Characteristics
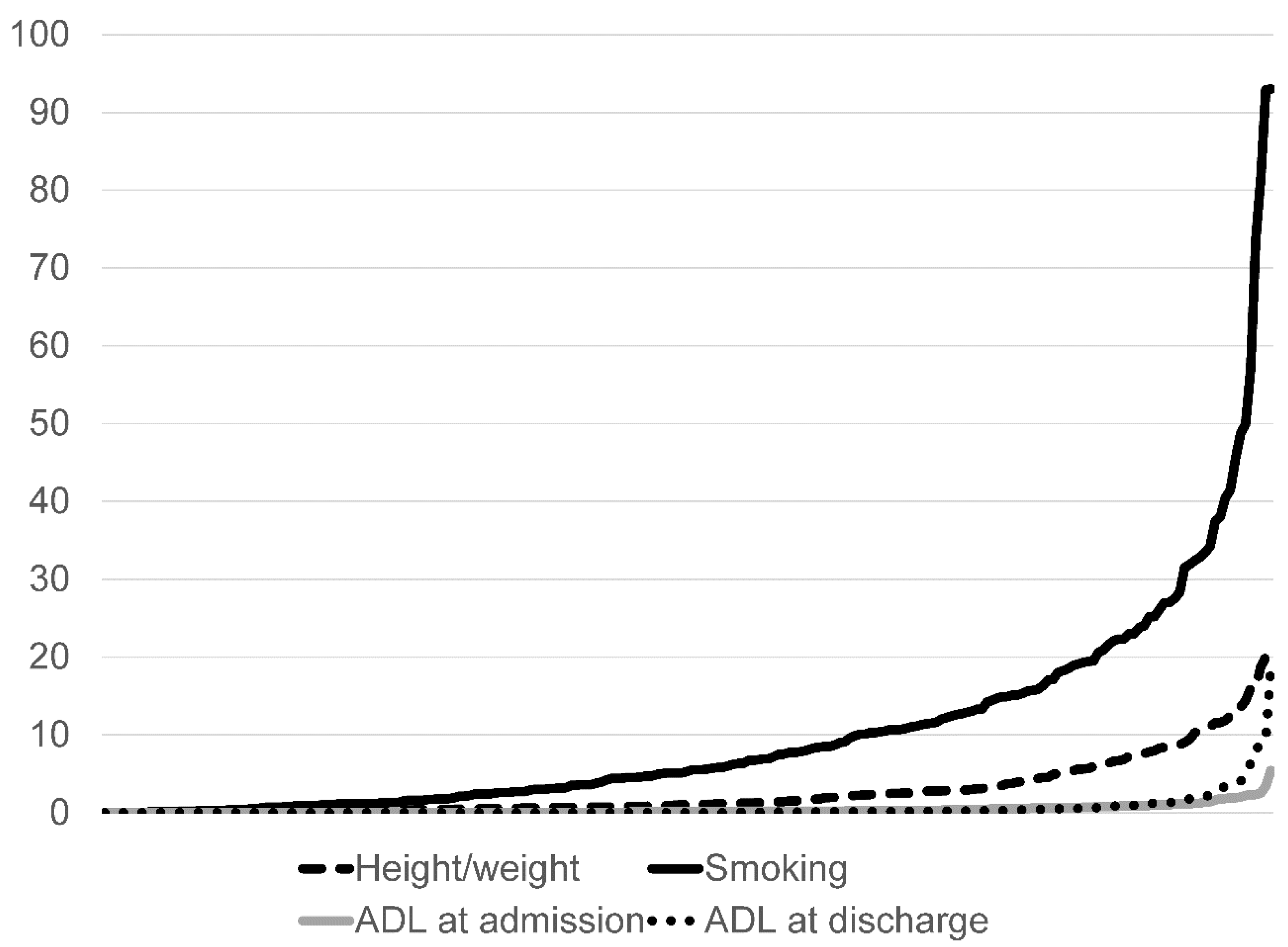
3.2. Pecentage of Unknown/Missing Data in Clinical Information (Height/Weight, Smoking Index, Activity of Daily Living)
3.3. Validation of Data By Comparing Other Variables/Data Sources
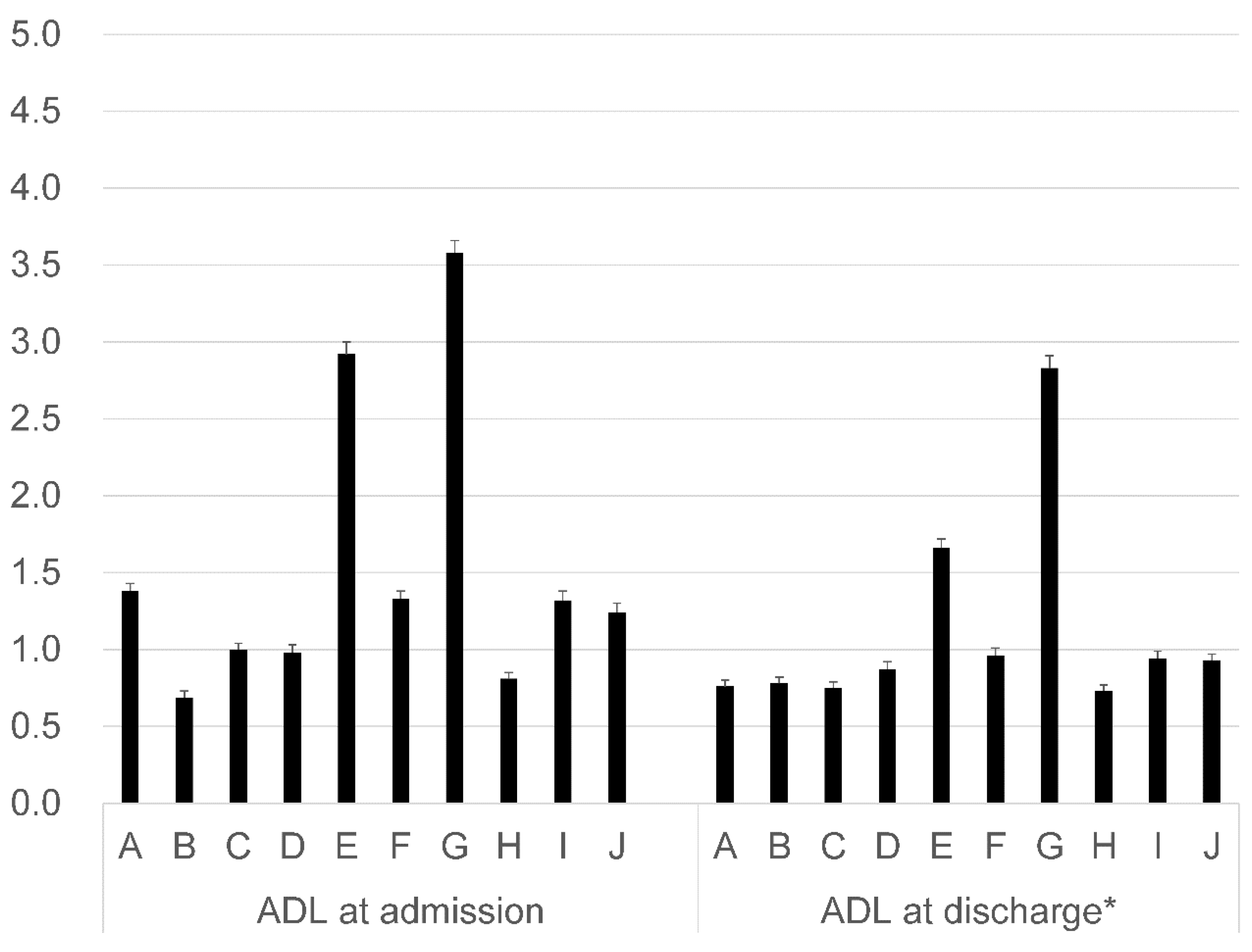
3.3.1. Consistency of ADL Data Compared to Japan Coma Scale
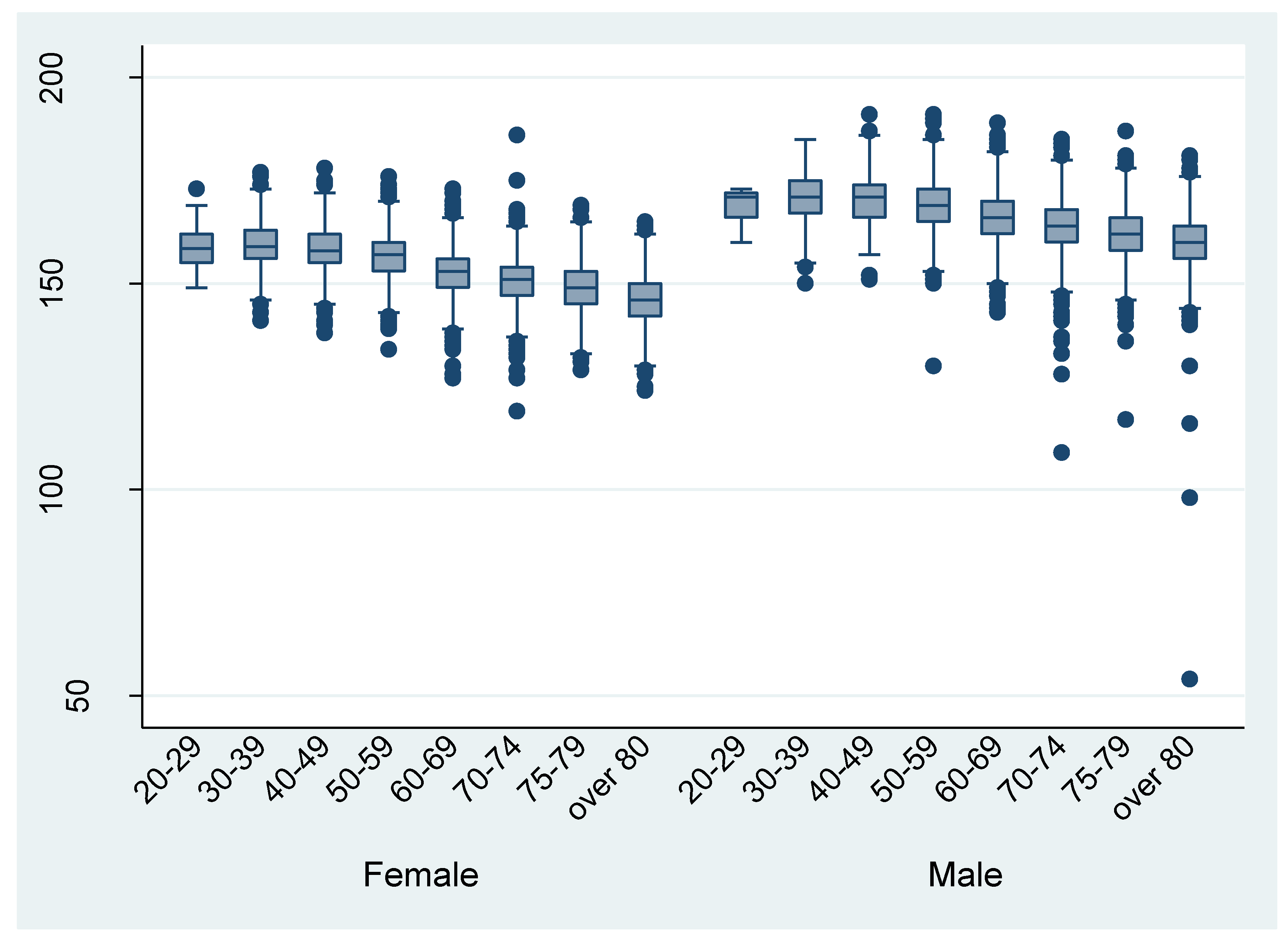
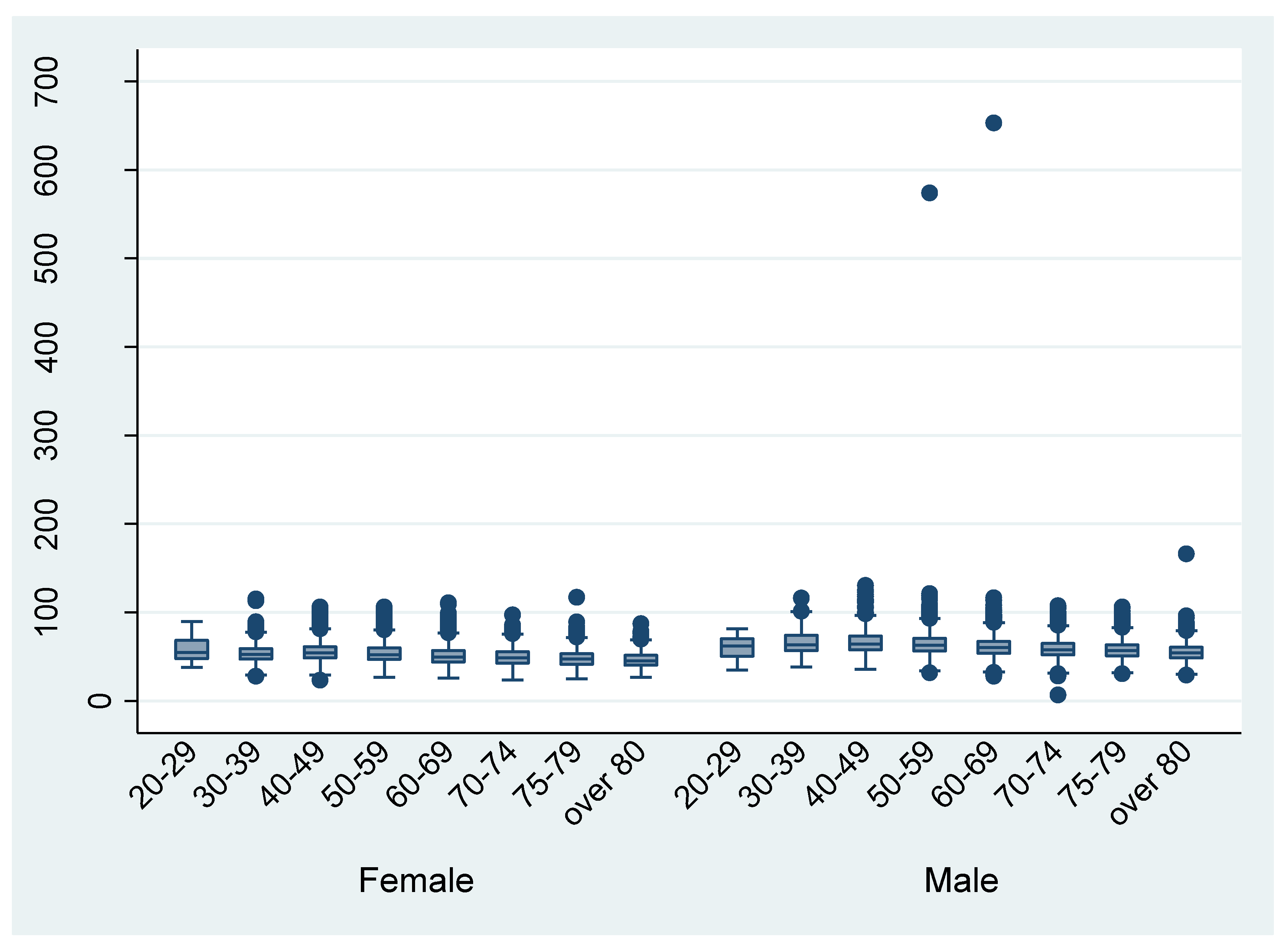
3.3.2. Height and Weight Data as Compared to the National Statistics
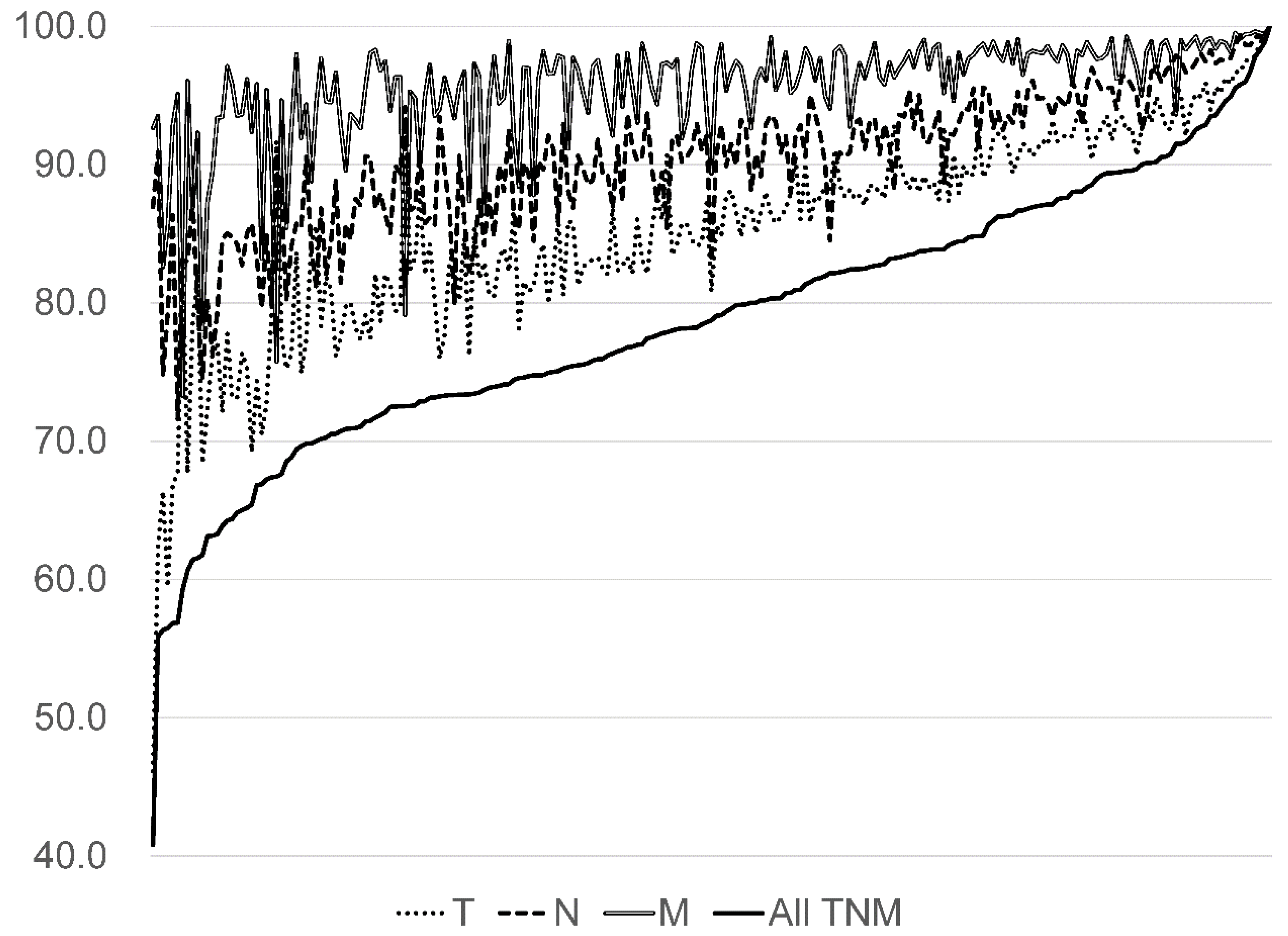
3.3.3. Tumour-Node-Metastasis Classifications Compared to the Hospital-Based Cancer Registries Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Langan, S.M.; Schmidt, S.A.; Wing, K.; Ehrenstein, V.; Nicholls, S.G.; Filion, K.B.; Klungel, O.; Petersen, I.; Sorensen, H.T.; Dixon, W.G.; et al. The reporting of studies conducted using observational routinely collected health data statement for pharmacoepidemiology (RECORD-PE). BMJ 2018, 363, k3532. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; Von Elm, E.; Langan, S.M.; RECORD Working Committee. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, S. Developments in post-marketing comparative effectiveness research. Clin. Pharmacol. Ther. 2007, 82, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, S.; Avorn, J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. J. Clin. Epidemiol. 2005, 58, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Higashi, T.; Nakamura, F.; Shibata, A.; Emori, Y.; Nishimoto, H. The national database of hospital-based cancer registries: A nationwide infrastructure to support evidence-based cancer care and cancer control policy in Japan. Jpn. J. Clin. Oncol. 2014, 44, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, M.; Nakamura, F.; Higashi, T. Monitoring and evaluating the quality of cancer care in Japan using administrative claims data. Cancer Sci. 2016, 107, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Booth, C.M.; Tannock, I.F. Randomised controlled trials and population-based observational research: Partners in the evolution of medical evidence. Br. J. Cancer 2014, 110, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Sasabuchi, Y.; Yasunaga, H.; Matsui, H.; Lefor, A.T.; Horiguchi, H.; Fushimi, K.; Sanui, M. The dose-response relationship between body mass index and mortality in subjects admitted to the ICU with and without mechanical ventilation. Respir. Care 2015, 60, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Yasunaga, H.; Inokuchi, R.; Horiguchi, H.; Fushimi, K.; Matsubara, T.; Nakajima, S.; Yahagi, N. Relationship between hospital volume and early outcomes in acute ischemic stroke patients treated with recombinant tissue plasminogen activator. Int. J. Stroke 2015, 10, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Takaoka, M.; Okuyama, A.; Mekata, E.; Masuda, M.; Otani, M.; Higashide, S.; Higashi, T. Staging discrepancies between Hospital-Based Cancer Registry and Diagnosis Procedure Combination data. Jpn. J. Clin. Oncol. 2016, 46, 788–791. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Welfare, Health, and Labours in Japan. National Health and Nutrition Survey. 2013. Available online: https://www.mhlw.go.jp/bunya/kenkou/kenkou_eiyou_chousa.html (accessed on 1 November 2019).
- Sobin, L.; Gospodarwicz, M.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; International Union against Cancer: Geneva, Switzerland, 2010. [Google Scholar]
- Newgard, C.D.; Haukoos, J.S. Measuring quality with missing data: The invisible threat to national quality initiatives. Acad. Emerg. Med. 2010, 17, 1130–1133. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Song, J.; Belin, T.R.; Unützer, J. A comparison of imputation methods in a longitudinal randomized clinical trial. Stat. Med. 2005, 24, 2111–2128. [Google Scholar] [CrossRef] [PubMed]
- Newgard, C.D.; Haukoos, J.S. Advanced statistics: Missing data in clinical research—Part 2: Multiple imputation. Acad. Emerg. Med. 2007, 14, 669–678. [Google Scholar] [PubMed]
- Moons, K.G.; Donders, R.A.; Stijnen, T.; Harrell, F.E. Using the outcome for imputation of missing predictor values was preferred. J. Clin. Epidemiol. 2006, 59, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- RECORD. Reporting of Studies Conducted Using Observational Routinely—Collected Data. 2018. Available online: http://www.record-statement.org/ (accessed on 28 August 2018).
- Okuyama, A.; Yokoyama, K.; Higashi, T. Making proposal for the Reporting of studies conducted using observational routinely collected health data. J. Jpn. Soc. Qual. Saf. Healthc. 2017, 12, 413–417, 478–480. [Google Scholar]
- Yasunaga, H.; Horiguchi, H.; Matsuda, S.; Fushimi, K.; Hashimoto, H.; Ayanian, J.Z. Body mass index and outcomes following gastrointestinal cancer surgery in Japan. Br. J. Surg. 2013, 100, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, Y.; Hasegawa, W.; Yasunaga, H.; Sunohara, M.; Jo, T.; Takami, K.; Matsui, H.; Fushimi, K.; Nagase, T. Paradoxical association between body mass index and in-hospital mortality in elderly patients with chronic obstructive pulmonary disease in Japan. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 1337–1346. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, M.; Kubo, T.; Yamamoto, M.; Muramatsu, K.; Yasunaga, H.; Horiguchi, H.; Fujimori, K.; Matsuda, S.; Fushimi, K.; Harada, M. Body mass index influences the outcome of acute pancreatitis: An analysis based on the Japanese administrative database. Pancreas 2014, 43, 863–866. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics (Per Patient) | n | (%) |
|---|---|---|
| Men | 95,872 | 53.1 |
| Age | ||
| 20–40 years | 3514 | 2.0 |
| 40–64 years | 56,928 | 31.6 |
| 65–74 years | 59,021 | 32.7 |
| 75–84 years | 49,408 | 27.4 |
| over 85 years | 11,528 | 6.4 |
| Cancer | ||
| Stomach | 48,297 | 26.8 |
| Colorectal | 38,881 | 21.6 |
| Liver | 13,814 | 7.7 |
| Lung | 43,310 | 24.0 |
| Breast | 36,097 | 20.0 |
| Clinical stage | ||
| 0 | 11,335 | 6.3 |
| I | 76,386 | 42.3 |
| II | 29,639 | 16.4 |
| III | 21,762 | 12.1 |
| IV | 29,324 | 16.3 |
| Unknown | 11,953 | 6.6 |
| Clinical department (per discharge)* | ||
| Internal medicine | 141,118 | 50.5 |
| Surgery | 127,682 | 45.7 |
| Emergency department | 480 | 0.2 |
| Others | 9826 | 3.5 |
| Proportion of Unknown Data, % (95% CI) | ||||
|---|---|---|---|---|
| Height/Weight | Smoking Index | ADL at Admission * | ADL at Discharge *,** | |
| (n = 279,451) | (n = 279,451) | (n = 279,343) | (n = 265,196) | |
| Total | 2.3 (2.2–2.4) | 10.5(10.3–10.7) | 0.3(0.3–0.4) | 0.6(0.6–0.6) |
| Sex | ||||
| Men | 2.4(2.3–2.5) | 11.9(11.6–12.1) | 0.4(0.3–0.4) | 0.6(0.6–0.7) |
| Women | 2.2(2.1–2.3) | 8.5(8.3–8.7) | 0.3(0.3–0.3) | 0.5(0.5–0.6) |
| Patients’ age | ||||
| 20–40 years | 0.9(0.7–1.2) | 8.5(7.3–9.7) | 0.2(0.1–0.4) | 1.0(0.7–1.3) |
| 40–64 years | 1.4(1.3–1.5) | 9.3(8.9–9.6) | 0.2(0.2–0.3) | 0.5(0.5–0.6) |
| 65–74 years | 1.8(1.8–1.9) | 10.6(10.3–10.9) | 0.3(0.3–0.3) | 0.6(0.5–0.6) |
| 75–84 years | 3.1(2.9–3.2) | 11.7(11.3–12.0) | 0.5(0.4–0.5) | 0.7(0.6–0.7) |
| Over 85 years | 7.6(7.1–8.2) | 12.1(11.4–12.8) | 0.8(0.6–1.0) | 0.7(0.5–0.9) |
| Cancer | ||||
| Stomach | 2.3(2.2–2.4) | 11.5(11.1–11.9) | 0.3(0.3–0.4) | 0.6(0.6–0.7) |
| Colorectal | 2.7(2.5–2.8) | 11.2(10.8–11.6) | 0.4(0.4–0.5) | 0.5(0.4–0.6) |
| Liver | 2.7(2.5–3.0) | 12.3(11.7–13.0) | 0.4(0.3–0.5) | 0.7(0.6–0.9) |
| Lung | 2.4(2.3–2.5) | 9.7(9.4–10.0) | 0.3(0.3–0.4) | 0.7(0.6–0.7) |
| Breast | 1.2(1.1–1.3) | 8.3(7.9–8.8) | 0.2(0.1–0.2) | 0.4(0.3–0.4) |
| Clinical stage | ||||
| 0 | 1.8(1.6–2.1) | 9.0(8.4–9.7) | 0.2(0.1–0.3) | 0.3(0.2–0.5) |
| I | 1.7(1.6–1.8) | 10.4(10.2–10.7) | 0.2(0.2–0.3) | 0.6(0.5–0.6) |
| II | 1.9(1.8–2.0) | 9.8(9.3–10.2) | 0.3(0.3–0.4) | 0.6(0.5–0.6) |
| III | 2.3(2.2–2.5) | 10.8(10.3–11.4) | 0.4(0.4–0.5) | 0.6(0.5–0.6) |
| IV | 3.1(3.0–3.3) | 10.7(10.3–11.2) | 0.4(0.4–0.5) | 0.7(0.7–0.8) |
| Unknown | 4.1(3.7–4.5) | 12.3(11.5–13.1) | 0.5(0.4–0.6) | 0.5(0.4–0.7) |
| Clinical department | ||||
| Internal medicine | 3.0(2.9–3.1) | 10.6(10.3–10.8) | 0.4(0.4–0.4) | 0.6(0.6–0.7) |
| Surgery | 1.4(1.4–1.5) | 10.1(9.9–10.3) | 0.3(0.2–0.3) | 0.5(0.5–0.6) |
| Emergency department | 15.8(12.8–19.4) | 24.0(20.4–28.0) | 7.7(5.7–10.4) | 1.2(0.5–3.3) |
| Others | 2.5(2.2–2.8) | 13.5(12.4–14.8) | 0.3(0.2–0.5) | 0.7(0.6–1.0) |
| N | Concordance Rate (%) | (95% Confidence Interval) | |
|---|---|---|---|
| All five cancers | |||
| T | 103,214 | 86.8 | (86.6–87.0) |
| N | 103,869 | 91.3 | (91.1–91.5) |
| M | 104,088 | 95.8 | (95.7–96.0) |
| All TNM | 103,142 | 80.6 | (80.3–80.8) |
| Stomach | |||
| T | 29,189 | 88.8 | (88.5–89.2) |
| N | 29,464 | 90.1 | (89.7–90.4) |
| M | 29,513 | 95.2 | (95.0–95.5) |
| All TNM | 29,175 | 82.0 | (81.6–82.4) |
| Colorecta | |||
| T | 19,017 | 82.1 | (81.6–82.7) |
| N | 19,179 | 86.8 | (86.3–87.3) |
| M | 19,218 | 94.5 | (94.1–94.8) |
| All TNM | 19,000 | 72.9 | (72.2–73.5) |
| Liver | |||
| T | 7697 | 70.9 | (69.9–71.92) |
| N | 7731 | 93.6 | (93.1–94.2) |
| M | 7786 | 94.8 | (94.3–95.3) |
| All TNM | 7681 | 67.9 | (66.9–69.0) |
| Lung | |||
| T | 26,184 | 91.1 | (90.7–91.4) |
| N | 26,358 | 93.4 | (93.1–93.7) |
| M | 26,430 | 97.0 | (96.8–97.2) |
| All TNM | 26,163 | 85.9 | (85.5–86.3) |
| Breast | |||
| T | 21,127 | 88.6 | (88.2–89.0) |
| N | 21,137 | 93.6 | (93.3–94.0) |
| M | 21,141 | 96.8 | (96.6–97.1) |
| All TNM | 21,123 | 83.6 | (83.1–84.1) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okuyama, A.; Higashi, T. Usability of Clinical Information in Discharge Summary Data in the Diagnosis Procedure Combination Survey for Cancer Patients. Int. J. Environ. Res. Public Health 2020, 17, 521. https://doi.org/10.3390/ijerph17020521
Okuyama A, Higashi T. Usability of Clinical Information in Discharge Summary Data in the Diagnosis Procedure Combination Survey for Cancer Patients. International Journal of Environmental Research and Public Health. 2020; 17(2):521. https://doi.org/10.3390/ijerph17020521
Chicago/Turabian StyleOkuyama, Ayako, and Takahiro Higashi. 2020. "Usability of Clinical Information in Discharge Summary Data in the Diagnosis Procedure Combination Survey for Cancer Patients" International Journal of Environmental Research and Public Health 17, no. 2: 521. https://doi.org/10.3390/ijerph17020521
APA StyleOkuyama, A., & Higashi, T. (2020). Usability of Clinical Information in Discharge Summary Data in the Diagnosis Procedure Combination Survey for Cancer Patients. International Journal of Environmental Research and Public Health, 17(2), 521. https://doi.org/10.3390/ijerph17020521