Cadmium and Lead Levels in Blood and Arsenic Levels in Urine among Schoolchildren Living in Contaminated Glassworks Areas, Sweden


Abstract
:1. Introduction
2. Materials and Methods
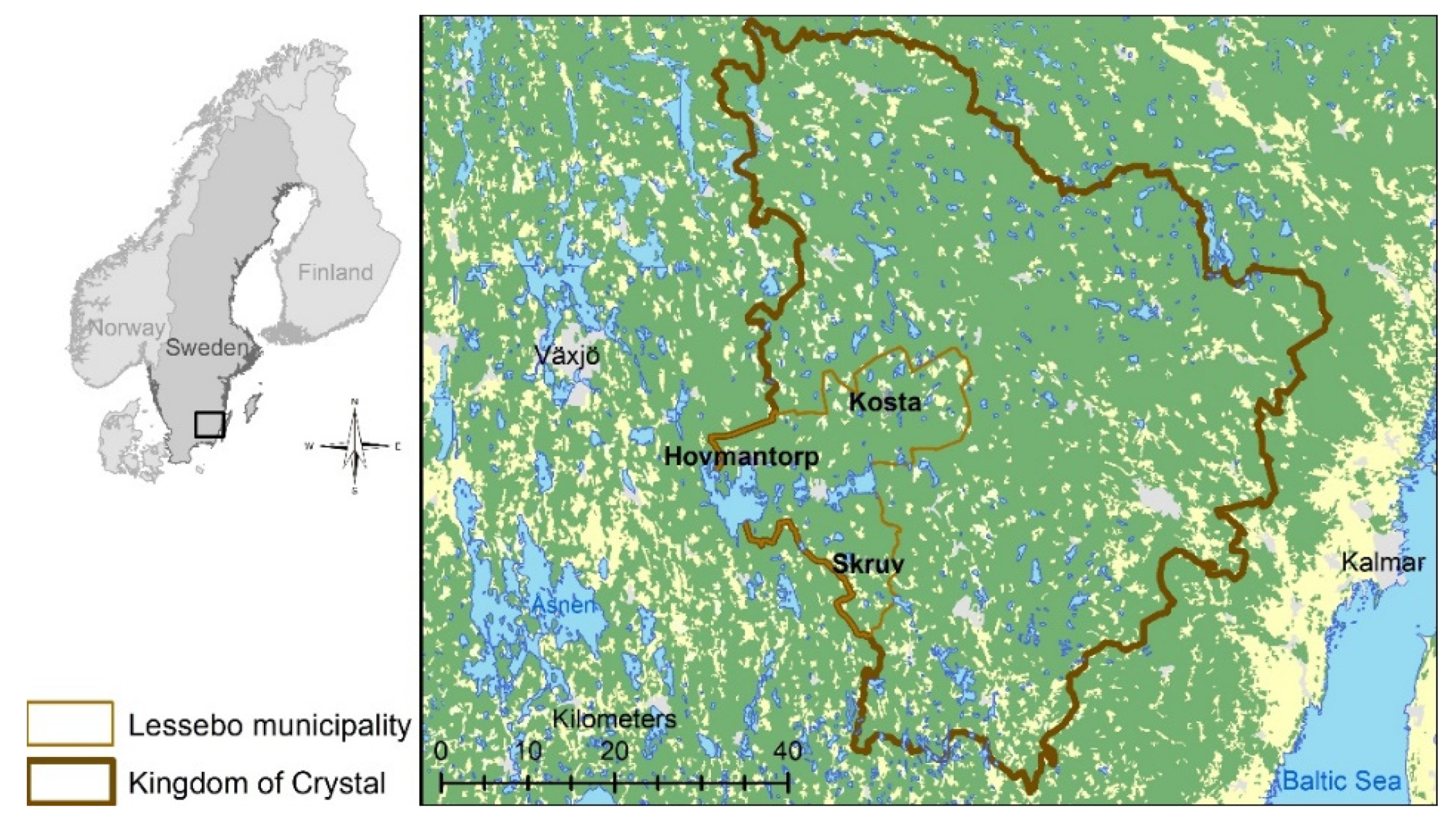
2.1. Study Area
2.2. Study Sample
2.3. Analysis of Blood Samples
2.4. Analysis of Urine
2.5. Statistical Analysis
3. Results
3.1. Cd and Pb in Blood
3.2. As in Urine
4. Discussion
4.1. Cd
4.2. Pb
4.3. As
4.4. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Höglund, L.O.; Fanger, G.; Yesilova, H. Final Report—Glasbruksprojektet 2006–2007. Slutrapport—Glasbruksprojektet 2006–2007; Kemakta Konsult AB: Stockholm, Sweden, 2007. (In Swedish) [Google Scholar]
- Augustsson, A.L.; Uddh-Söderberg, T.E.; Hogmalm, K.J.; Filipsson, M.E. Metal uptake by homegrown vegetables—The relative importance in human health risk assessments at contaminated sites. Environ. Res. 2015, 138, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, G.; Fowler, B.A.; Nordberg, M. Handbook on the Toxicology of Metals, 4th ed.; Academic Print: London, UK, 2015; Volume 2. [Google Scholar]
- European Food Safety Authority (EFSA). Cadmium in food—Scientific opinion of the Panel on Contaminants in the Food Chain. EFSA J. 2009, 7. [Google Scholar] [CrossRef]
- Swedish Environmental Protection Agency. Health Risk Assessment of Polluted Areas: Report 5859. Hälsoriskbedömning Av Förorenade Områden: Rapport 5859; Naturvårdsverket: Stockholm, Sweden, 2008. (In Swedish) [Google Scholar]
- Åkesson, A.; Berglund, M.; Schütz, A.; Bjellerup, P.; Bremme, K.; Vahter, M. Cadmium exposure in pregnancy and lactation in relation to iron status. Am. J. Public Health 2002, 92, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Åkesson, A.; Bjellerup, P.; Lundh, T.; Lidfeldt, J.; Nerbrand, C.; Samsioe, G.; Skerfving, S.; Vahter, M. Cadmium-Induced Effects on Bone in a Population-Based Study of Women. Environ. Health Perspect. 2006, 114, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Åkesson, A.; Lundh, T.; Vahter, M.; Bjellerup, P.; Lidfeldt, J.; Nerbrand, C.; Samsioe, G.; Strömberg, U.; Skerfving, S. Tubular and Glomerular Kidney Effects in Swedish Women with Low Environmental Cadmium Exposure. Environ. Health Perspect. 2005, 113, 1627–1631. [Google Scholar] [CrossRef] [PubMed]
- Järup, L.; Åkesson, A. Current status of cadmium as an environmental health problem. Toxicol. Appl. Pharmacol. 2009, 238, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Suwazono, Y.; Sand, S.; Vahter, M.; Skerfving, S.; Lidfeldt, J.; Åkesson, A. Benchmark dose for cadmium-induced osteoporosis in women. Toxicol. Lett. 2010, 197, 123–127. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC). List of Classifications by Cancer Sites with Sufficient or Limited Evidence in Humans; IARC: Lyon, France, 2018; Volume 1–124a. [Google Scholar]
- Nishijo, M.; Morikawa, Y.; Nakagawa, H.; Tawara, K.; Miura, K.; Kido, T.; Ikawa, A.; Kobayashi, E.; Nogawa, K. Causes of death and renal tubular dysfunction in residents exposed to cadmium in the environment. Occup. Environ. Med. 2006, 63, 545–550. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Lead—Draft for Public Comment; ATSDR: Atlanta, GA, USA, 2019. [Google Scholar]
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-Level Environmental Lead Exposure and Children’s Intellectual Function: An International Pooled Analysis. Environ. Health Perspect. 2005, 113, 894–899. [Google Scholar] [CrossRef]
- Lucchini, R.G.; Zoni, S.; Guazzetti, S.; Bontempi, E.; Micheletti, S.; Engström, K.; Parrinello, G.; Smith, N.R. Inverse association of intellectual function with very low blood lead but not with manganese exposure in Italian adolescents. Environ. Res. 2012, 118, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Skerfving, S.; Löfmark, L.; Lundh, T.; Mikoczy, Z.; Strömberg, U. Late effects of low blood lead concentrations in children on school performance and cognitive functions. Neurotoxicology 2015, 49, 114–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Food Safety Authority (EFSA). EFSA Panel on Contaminants in the Food Chain (CONTAM); Scientific Opinion on Lead in Food. EFSA J. 2010, 8, 1570. [Google Scholar] [CrossRef]
- Mason, L.H.; Harp, J.P.; Han, D.Y. Pb Neurotoxicity: Neuropsychological Effects of Lead Toxicity. BioMed Res. Int. 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Agency for Research on Cancer (IARC). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans—Inorganic and Organic Lead Compounds; IARC: Lyon, France, 2006; Volume 87. [Google Scholar]
- Cubadda, F.; Jackson, B.P.; Cottingham, K.L.; Van Horne, Y.O.; Kurzius-Spencer, M. Human exposure to dietary inorganic arsenic and other arsenic species: State of knowledge, gaps and uncertainties. Sci. Total Environ. 2017, 579, 1228–1239. [Google Scholar] [CrossRef] [Green Version]
- The Institute for Environmental Medicine. Arsenic. (In Swedish: Arsenik); The Institute for Environmental Medicin: Solna, Sweden, 2017. (In Swedish) [Google Scholar]
- Concha, G.; Vogler, G.; Nermell, B.; Vahter, M. Intra-individual variation in the metabolism of inorganic arsenic. Int. Arch. Occup. Environ. Health 2002, 75, 576–580. [Google Scholar] [CrossRef]
- Engström, K.S.; Engström, K.; Concha, G.; Nermell, B.; Warholm, M.; Vahter, M. Genetic Polymorphisms Influencing Arsenic Metabolism: Evidence from Argentina. Environ. Health Perspect. 2007, 115, 599–605. [Google Scholar] [CrossRef] [Green Version]
- Lovreglio, P.; D’Errico, M.N.; De Pasquale, P.; Gilberti, M.E.; Drago, I.; Panuzzo, L.; Lepera, A.; Serra, R.; Ferrara, F.; Basso, A.; et al. Environmental factors affecting the urinary excretion of inorganic arsenic in the general population. Med. Lav. 2012, 103, 372–381. [Google Scholar]
- Sattar, A.; Xie, S.; Hafeez, M.A.; Wang, X.; Hussain, H.I.; Iqbal, Z.; Pan, Y.; Iqbal, M.; Shabbir, M.A.; Yuan, Z. Metabolism and toxicity of arsenicals in mammals. Environ. Toxicol. Pharmacol. 2016, 48, 214–224. [Google Scholar] [CrossRef]
- Hughes, M.F. Arsenic toxicity and potential mechanisms of action. Toxicol. Lett. 2002, 133, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Denys, S.; Caboche, J.; Tack, K.; Rychen, G.; Wragg, J.; Cave, M.; Jondreville, C.; Feidt, C. In Vivo Validation of the Unified BARGE Method to Assess the Bioaccessibility of Arsenic, Antimony, Cadmium, and Lead in Soils. Environ. Sci. Technol. 2012, 46, 6252–6260. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.M.; Ohnishi, T.; Arnold, L.L.; Le, X.C. Arsenic-induced bladder cancer in an animal model. Toxicol. Appl. Pharmacol. 2007, 222, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Hirano, S. Metabolism of arsenic and its toxicological relevance. Arch. Toxicol. 2012, 87, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Abdul, K.S.M.; Jayasinghe, S.S.; Chandana, E.P.; Jayasumana, C.; De Silva, P.M.C.S. Arsenic and human health effects: A review. Environ. Toxicol. Pharmacol. 2015, 40, 828–846. [Google Scholar] [CrossRef]
- Kuo, C.-C.; Moon, K.A.; Wang, S.-L.; Silbergeld, E.; Navas-Acien, A. The Association of Arsenic Metabolism with Cancer, Cardiovascular Disease, and Diabetes: A Systematic Review of the Epidemiological Evidence. Environ. Health Perspect. 2017, 125, 087001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettinger, A.S.; Arbuckle, T.E.; Fisher, M.; Liang, C.L.; Davis, K.; Cirtiu, C.-M.; Bélanger, P.; Leblanc, A.; Fraser, W.D. Arsenic levels among pregnant women and newborns in Canada: Results from the Maternal-Infant Research on Environmental Chemicals (MIREC) cohort. Environ. Res. 2017, 153, 8–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahar, M.N.; Inaoka, T.; Fujimura, M.; Watanabe, C.; Shimizu, H.; Tasnim, S.; Sultana, N. Arsenic contamination in groundwater and its effects on adolescent intelligence and social competence in Bangladesh with special reference to daily drinking/cooking water intake. Environ. Health Prev. Med. 2013, 19, 151–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustsson, A.; Uddh-Söderberg, T.; Filipsson, M.; Helmfrid, I.; Berglund, M.; Karlsson, H.; Hogmalm, J.; Karlsson, A.; Alriksson, S. Challenges in assessing the health risks of consuming vegetables in metal-contaminated environments. Environ. Int. 2018, 113, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Alesia, F.; Rosalind, P.; Helena, S.-G. A Review of the Field on Children’s Exposure to Environmental Contaminants: A Risk Assessment Approach. Int. J. Environ. Res. Public Health 2017, 14, 265. [Google Scholar]
- Hruba, F.; Strömberg, U.; Černá, M.; Chen, C.; Harari, F.; Harari, R.; Horvat, M.; Koppova, K.; Kos, A.; Krsková, A.; et al. Blood cadmium, mercury, and lead in children: An international comparison of cities in six European countries, and China, Ecuador, and Morocco. Environ. Int. 2012, 41, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Lundh, T.; Axmon, A.; Skerfving, S.; Engström, K. Cadmium and mercury exposure over time in Swedish children. Environ. Res. 2016, 150, 600–605. [Google Scholar] [CrossRef]
- Alonso, E.; Cambra, K.; Martínez, T. Lead and Cadmium Exposure from Contaminated Soil among Residents of a Farm Area near an Industrial Site. Arch. Environ. Health Int. J. 2001, 56, 278–282. [Google Scholar] [CrossRef]
- Oulhote, Y.; Le Tertre, A.; Etchevers, A.; Le Bot, B.; Lucas, J.-P.; Mandin, C.; Le Strat, Y.; Lanphear, B.; Glorennec, P. Implications of different residential lead standards on children’s blood lead levels in France: Predictions based on a national cross-sectional survey. Int. J. Hyg. Environ. Health 2013, 216, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Ranft, U.; Delschen, T.; Machtolf, M.; Sugiri, D.; Wilhelm, M. Lead Concentration in the Blood of Children and its Association with Lead in Soil and Ambient Air—Trends Between 1983 and 2000 in Duisburg. J. Toxicol. Environ. Health Part A 2008, 71, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.E.; Acosta-Saavedra, L.C.; Meza-Figueroa, D.; Vera, E.; Cebrian, M.E.; Ostrosky-Wegman, P.; Calderón-Aranda, E.S. Biomonitoring of metal in children living in a mine tailings zone in Southern Mexico: A pilot study. Int. J. Hyg. Environ. Health 2010, 213, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Zamaratskaia, G.; Lignell, S.; Bjermo, H. Contaminants in Blood and Urine from Adolescents in Sweden: Results from the National Dietary Survey Riksmaten Adolescents 2016–2017; Livsmedelsverket: Uppsala, Sweden, 2020; p. 103. [Google Scholar]
- Lundh, T.; Assarsson, E.; Broberg, K.S. Tidstrender för Bly, Kadmium Och Kvicksilver—En Uppdatering 2019; Lund Universitet: Lund, Sweden, 2020; p. 14. [Google Scholar]
- Strömberg, U.; Lundh, T.; Skerfving, S. Yearly measurements of blood lead in Swedish children since 1978: The declining trend continues in the petrol-lead-free period 1995–2007. Environ. Res. 2008, 107, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Andrén, P.; Schutz, A.; Vahter, M.; Attewell, R.; Johansson, L.; Willers, S.; Skerfving, S. Environmental exposure to lead and arsenic among children living near a glassworks. Sci. Total Environ. 1988, 77, 25–34. [Google Scholar] [CrossRef]
- County Administrative Board of Kronoberg. Inventory of Polluted Areas according to MIFO Phase 1 -Glassworks in Kalmar and Kronoberg Counties. Inventering av Förorenade Områden Enligt MIFO Fas 1 -Glasbruk i Kalmar och Kronobergs län; Länsstyrelsen: Kronoberg, Sweden, 2001. (In Swedish) [Google Scholar]
- Mattisson, K.; Tekavec, E.; Lundh, T.; Olsson, A.; Stroh, E. Environmental Health Monitoring of Children in Areas with Contaminated Land from Glassworks. Miljömedicinsk Hälsoövervakning av Barn i Områden Med Förorenad Mark Från Glasbruk- Lessebo Kommun; Lund University: Lund, Sweden, 2018. (In Swedish) [Google Scholar]
- De Burbure, C.; Buchet, J.-P.; Leroyer, A.; Nisse, C.; Haguenoer, J.-M.; Mutti, A.; Smerhovsky, Z.; Cikrt, M.; Trzcinka-Ochocka, M.; Razniewska, G.; et al. Renal and Neurologic Effects of Cadmium, Lead, Mercury, and Arsenic in Children: Evidence of Early Effects and Multiple Interactions at Environmental Exposure Levels. Environ. Health Perspect. 2006, 114, 584–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillol, C.; Dor, F.; Denys, S.; Tack, K.; Labat, L.; Seta, N. Arsenic urinary concentrations in children living in a naturally arsenic contaminated area. J. Expo. Sci. Environ. Epidemiol. 2012, 23, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadmium dietary exposure in the European population. EFSA J. 2012, 10. [CrossRef]
- Swedish Chemicals Agency. Economic Cost of Fractures Caused by Dietary Cadmium Exposure; Swedish Chemicals Agency: Sundyberg, Sweden, 2013. [Google Scholar]
- European Food Safety Authority (EFSA). Lead Dietary Exposure in the European Population; Scientific Report of EFSA; European Food Safety Authority: Parma, Italy, 2012. [Google Scholar]
- Centre for Disease Control and Prevention (CDC). Fourth National Report on Human Exposure to Environmental Chemicals; Updated Tables; CDC: Atlanta, GA, USA, 2019; Volume 1. [Google Scholar]
- Stromberg, U.; Schutz, A.; Skerfving, S. Substantial decrease of blood lead in Swedish children, 1978-94, associated with petrol lead. Occup. Environ. Med. 1995, 52, 764–769. [Google Scholar] [CrossRef] [Green Version]
- Basu, A.; Mitra, S.; Chung, J.; Mazumder, D.G.; Ghosh, N.; Kalman, D.; Von Ehrenstein, O.S.; Steinmaus, C.; Liaw, J.; Smith, A.H. Creatinine, Diet, Micronutrients, and Arsenic Methylation in West Bengal, India. Environ. Health Perspect. 2011, 119, 1308–1313. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Gender | N (%) |
|---|---|
| Girl | 40 (46%) |
| Boy | 47 (54%) |
| School | |
| Hovmantorp | 60 (69%) |
| Lustigkullaskolan | 14 (16%) |
| Björkskolan | 13 (15%) |
| Attended grade | |
| 2 | 29 (33%) |
| 3 | 35 (40%) |
| 4 | 23 (26%) |
| Born and raised in the area | |
| Yes | 50 (58%) |
| No | 36 (42%) |
| Smoking parent | |
| Yes | 9 (10%) |
| No | 78 (90%) |
| Play or cast tin soldiers, fish with Pb sinker or shoots with air rifle | |
| Yes | 10 (12%) |
| No | 75 (88%) |
| Eat locally grown vegetables | |
| Yes | 40 (46%) |
| No | 47 (54%) |
| Drink water from own well | |
| Yes | 19 (22%) |
| No | 67 (78%) |
| Eat local fresh water fish | |
| Yes | 21 (24%) |
| No | 66 (76%) |
| Study Area | Cd (µg/L) | Pb (µg/L) | ||||
|---|---|---|---|---|---|---|
| Location | Year | N | GM | Range | GM | Range |
| Lessebo | 2017 | 85 | 0.09 | 0.04–0.26 | 9.9 | 4.2–42 |
| Grouping Variable | Cd | (µg/L) | Pb | (µg/L) | ||||
|---|---|---|---|---|---|---|---|---|
| N | GM | Range | p-Value | GM | Range | p-Value | ||
| Gender | Girl | 39 | 0.10 | 0.05–0.24 | 0.302 | 10 | 4.6–42 | 0.748 |
| Boy | 46 | 0.09 | 0.04–0.26 | 9.7 | 4.2–25 | |||
| Born and raised in the area | Yes | 49 | 0.08 | 0.04–0.24 | 0.002 | 8.6 | 4.2–23 | 0.002 |
| No | 35 | 0.11 | 0.05–0.26 | 12 | 5.9–42 | |||
| Smoking parent | Yes | 8 | 0.08 | 0.04–0.19 | 0.359 | 12 | 5.8–42 | 0.443 |
| No | 77 | 0.09 | 0.04–0.26 | 9.6 | 4.2–25 | |||
| Play or cast tin soldiers, fish with Pb sinker or shoots with air rifle | Yes | 10 | 0.09 | 0.05–0.20 | 0.850 | 13 | 7.1–23 | 0.066 |
| No | 75 | 0.09 | 0.04–0.26 | 9.5 | 4.2–42 | |||
| Eat homegrown vegetables | Yes | 38 | 0.09 | 0.04–0.26 | 0.949 | 9.5 | 4.2–25 | 0.466 |
| No | 47 | 0.09 | 0.04–0.24 | 10 | 4.6–42 | |||
| Drink water from own well | Yes | 18 | 0.09 | 0.05–0.26 | 0.726 | 11 | 6.3–25 | 0.153 |
| No | 66 | 0.10 | 0.04–0.24 | 9.6 | 4.6–42 | |||
| Eat local caught fresh water fish | Yes | 21 | 0.09 | 0.42–0.24 | 0.693 | 8.7 | 4.6–17 | 0.153 |
| No | 64 | 0.09 | 0.45–0.26 | 10 | 4.2–42 |
| As Compound | GM (uq/L) | Range (uq/L) | GM ug/g Creatinine |
|---|---|---|---|
| DMA | 4.2 | 0.40–44 | 4.8 |
| MMA | 0.47 | 0–4.8 | 0.53 |
| AsIII | 0.28 | 0–2.0 | 0.29 |
| AsV | 0.82 | 0.44–2.5 | 0.93 |
| The sum of inorganic As | 6.1 | 1.2–48 | 6.9 |
| Grouping Variable | Inorganic As | (µg/L) | Inorganic As | (µg/g Creatinine) | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | GM | Range | p-Value | N | GM | Range | p-Value | ||
| Gender | Girl | 40 | 5.9 | 1.5–36 | 0.732 | 40 | 6.7 | 2.6–31 | 0.583 |
| Boy | 47 | 6.3 | 1.2–48 | 46 | 7.2 | 2.5–31 | |||
| Born and raised in the area | Yes | 50 | 5.7 | 1.2–48 | 0.367 | 49 | 6.3 | 2.5–31 | 0.049 |
| No | 36 | 6.6 | 2.0–30 | 36 | 8.0 | 3.8–30 | |||
| Smoking parent | Yes | 9 | 7.5 | 5.3–15 | 0.120 | 9 | 7.5 | 4.6–13 | 0.671 |
| No | 78 | 6.0 | 1.2–48 | 77 | 6.9 | 2.5–31 | |||
| Play or cast tin soldiers, fish with Pb sinker or shoots with air rifle | Yes | 10 | 8.8 | 2.3–33 | 0.116 | 10 | 7.4 | 2.9–19 | 0.730 |
| No | 77 | 5.8 | 2.5–31 | 76 | 6.9 | 2.5–31 | |||
| Eat homegrown vegetables | Yes | 40 | 6.4 | 1.7–36 | 0.581 | 40 | 6.8 | 2.5–31 | 0.679 |
| No | 47 | 5.8 | 1.2–48 | 46 | 7.1 | 2.5–31 | |||
| Drink water from own well | Yes | 19 | 8.0 | 1.8–33 | 0.102 | 19 | 7.2 | 2.6–19 | 0.788 |
| No | 67 | 5.7 | 1.2–48 | 66 | 6.9 | 2.5–31 | |||
| Eat local caught fresh water fish | Yes | 21 | 6.6 | 1.7–36 | 0.568 | 21 | 7.2 | 2.5–31 | 0.736 |
| No | 66 | 5.9 | 1.2–48 | 65 | 6.9 | 2.5–31 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mattisson, K.; Tekavec, E.; Lundh, T.; Stroh, E. Cadmium and Lead Levels in Blood and Arsenic Levels in Urine among Schoolchildren Living in Contaminated Glassworks Areas, Sweden. Int. J. Environ. Res. Public Health 2020, 17, 7382. https://doi.org/10.3390/ijerph17207382
Mattisson K, Tekavec E, Lundh T, Stroh E. Cadmium and Lead Levels in Blood and Arsenic Levels in Urine among Schoolchildren Living in Contaminated Glassworks Areas, Sweden. International Journal of Environmental Research and Public Health. 2020; 17(20):7382. https://doi.org/10.3390/ijerph17207382
Chicago/Turabian StyleMattisson, Kristoffer, Eva Tekavec, Thomas Lundh, and Emilie Stroh. 2020. "Cadmium and Lead Levels in Blood and Arsenic Levels in Urine among Schoolchildren Living in Contaminated Glassworks Areas, Sweden" International Journal of Environmental Research and Public Health 17, no. 20: 7382. https://doi.org/10.3390/ijerph17207382