Overweight and Obesity in Children of Immigrant Versus Native Parents: Exploring a Local Setting in Portugal


Abstract
1. Introduction
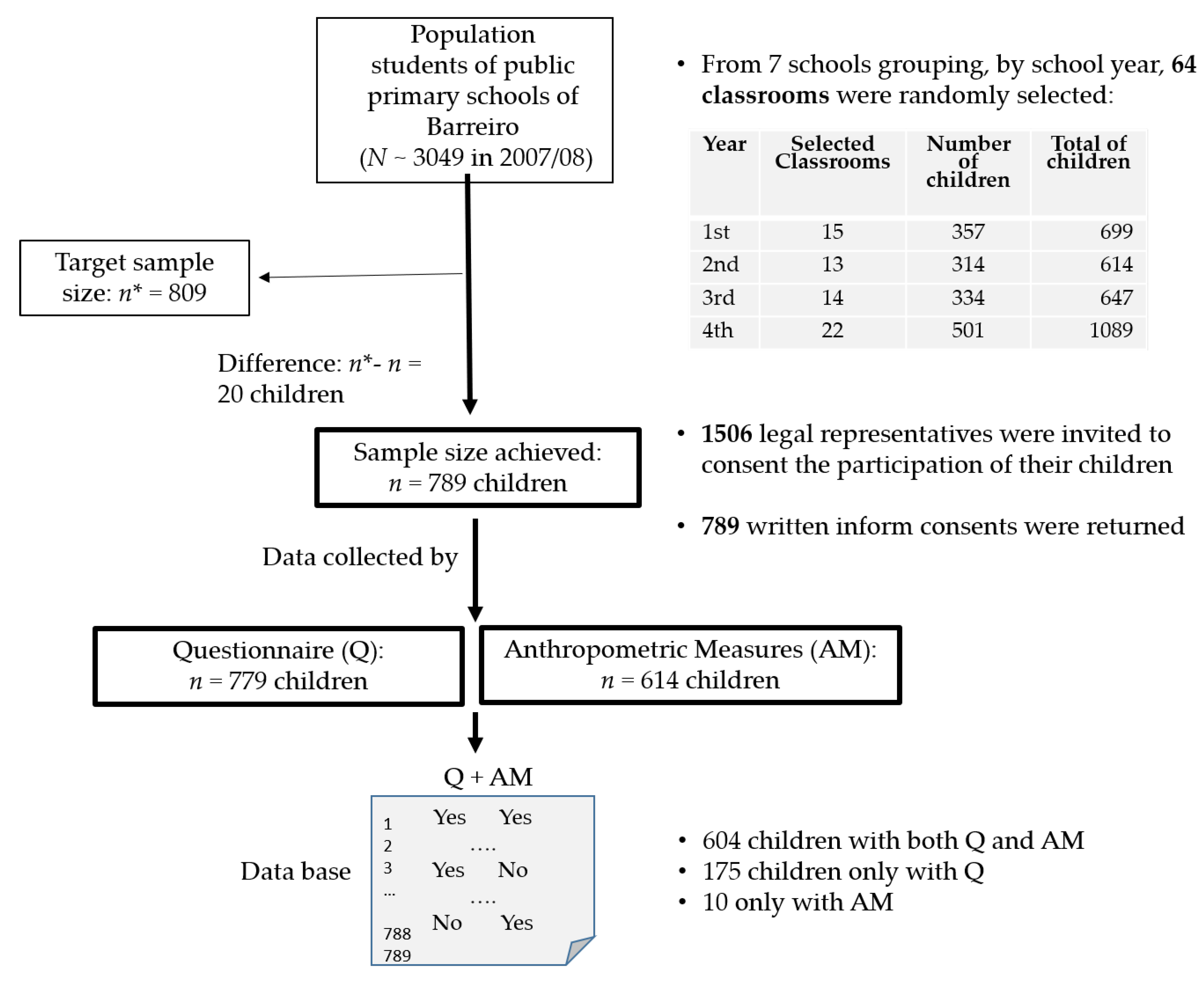
2. Methods
2.1. Sample Size and Variables
2.2. Statistical Analysis
2.3. Ethical Approval
3. Results
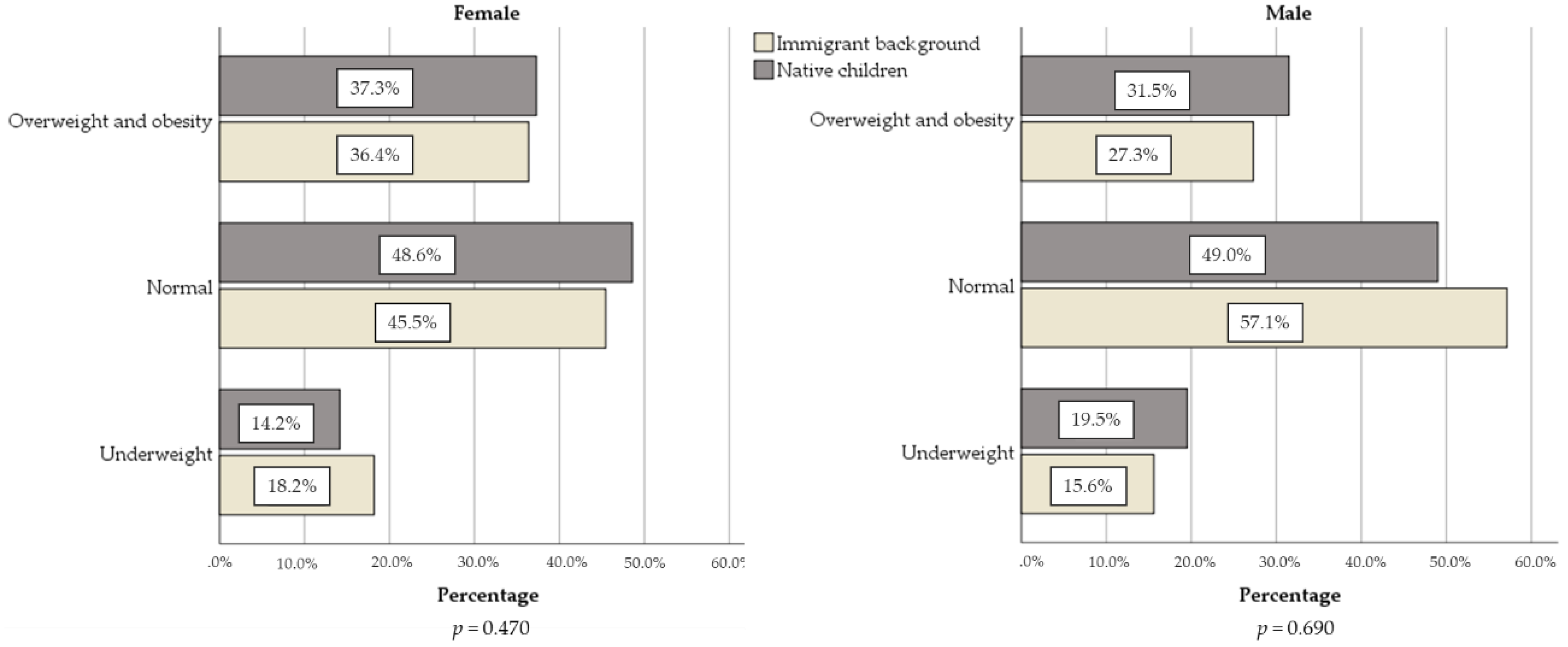
3.1. Sociodemographic Characteristics and Prevalence of Overweight and Obesity in Children, Considering the Parents’ Origin
3.2. Anthropometric Measures and Abdominal Obesity Risk
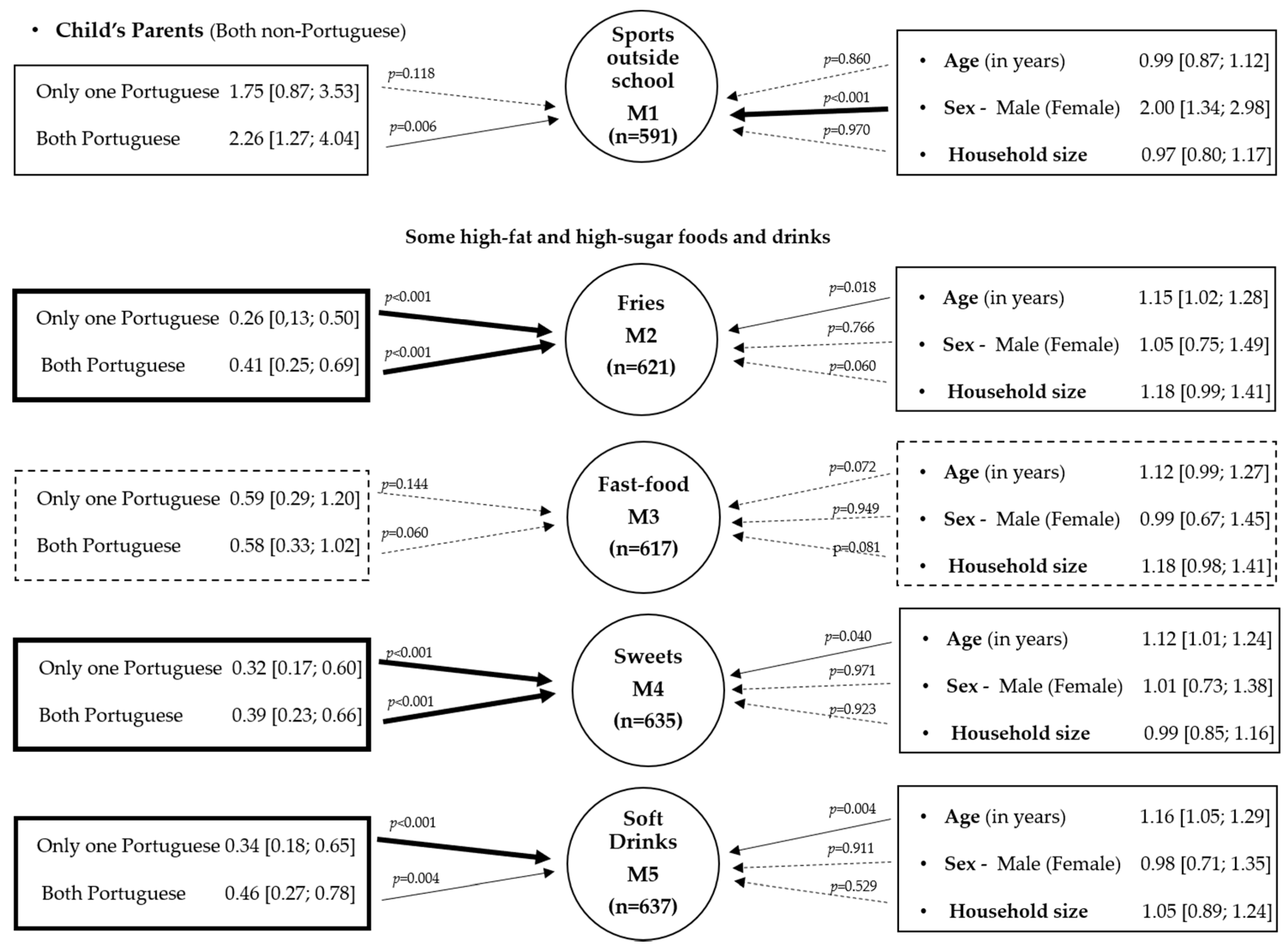
3.3. The Role of the Parent’s Origin in Some Potential Direct or Indirect Determinants of Obesity in Females and Male
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CPLP | Community of Portuguese-speaking countries |
| ISAK | International Society for the Advanced of Kinanthropometry. |
| CDC | Centers for Disease Control |
| BMI | Body mass index |
| WHtR | Waist-to-height ratio |
| EU-SILC | EU Statistics on Income and Living Conditions |
| SPSS 22.0 | Statistical Package for the Social Sciences version 22.0 |
| CI | Confidence interval |
| MWW | Mann–Whitney–Wilcoxon |
| KW | Kruskal–Wallis |
| ORa | Adjusted odds ratio |
| SD | Standard deviation |
| IOTF | International Obesity Task Force |
References
- Freedman, D.S.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. The relation of overweight to cardiovascular risk factors among children and adolescents: The Bogalusa Heart Study. Pediatrics 1999, 103, 1175–1182. [Google Scholar] [PubMed]
- Rodrigues, D.; Padez, C.; Machado-Rodrigues, A.M. Prevalence of Abdominal Obesity and Excess Weight among Portuguese Children and Why Abdominal Obesity Should Be Included in Clinical Practice. Acta Med. Port. 2018, 31, 159. [Google Scholar] [CrossRef] [PubMed]
- Raj, M. Obesity and cardiovascular risk in children and adolescents. Indian J. Endocrinol. Metab. 2012, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Wühl, E. Hypertension in childhood obesity. Acta Paediatr. 2019, 108, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Bingham, D.D.; Varela-Silva, M.I.; Ferrão, M.M.; Augusta, G.; Mourão, M.I.; Nogueira, H.; Marques, V.R.; Padez, C. Socio-demographic and behavioral risk factors associated with the high prevalence of overweight and obesity in Portuguese children: Overweight and Obesity in Portuguese Children. Am. J. Hum. Biol. 2013, 25, 733–742. [Google Scholar] [CrossRef]
- Gibson, L.Y.; Allen, K.L.; Davis, E.; Blair, E.; Zubrick, S.R.; Byrne, S.M. The psychosocial burden of childhood overweight and obesity: Evidence for persisting difficulties in boys and girls. Eur. J. Pediatr. 2017, 176, 925–933. [Google Scholar] [CrossRef]
- Blundell, J.E.; Baker, J.L.; Boyland, E.; Blaak, E.; Charzewska, J.; de Henauw, S.; Frühbeck, G.; Gonzalez-Gross, M.; Hebebrand, J.; Holm, L.; et al. Variations in the Prevalence of Obesity Among European Countries, and a Consideration of Possible Causes. Obes. Facts 2017, 10, 25–37. [Google Scholar] [CrossRef]
- Freitas, A.I.; Moreira, C.; Santos, A.C. Time trends in prevalence and incidence rates of childhood overweight and obesity in Portugal: Generation XXI birth cohort. Int. J. Obes. 2019, 43, 424–427. [Google Scholar] [CrossRef]
- Gregório, M.J.; Guedes, L.; Sousa, S.M. Programa Nacional para a Promoção da Alimentação Saudável 2019; Ministério da Saúde. Direção Geral da Saúde: Lisboa, Portugal, 2019. [Google Scholar]
- André, A.L.; Padez, C.; Rosado-Marques, V.; Griffiths, P.L.; Varela-Silva, M.I. Growing up in Portugal: Cape Verdean Ancestry Children Exhibit low overweight and obesity compared with Portuguese in urban Lisbon. J. Biosoc. Sci. 2017, 49, 842–857. [Google Scholar] [CrossRef]
- Rito, A.; Sousa, R.C.; Mendes, S.; Graça, P. Childhood Obesity Surveillance Initiative: COSI Portugal 2016; Instituto Nacional de Saúde Doutor Ricardo Jorge, IP: Lisboa, Portugal, 2017; p. 74. ISBN 978-989-8794-43-7. [Google Scholar]
- Pires, R.P. Portuguese Emigration Today. In New and Old Routes of Portuguese Emigration; Pereira, C., Azevedo, J., Eds.; IMISCOE Research Series; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Labree, W.; van de Mheen, D.; Rutten, F.; Rodenburg, G.; Koopmans, G.; Foets, M. Differences in Overweight and Obesity among Children from Migrant and Native Origin: The Role of Physical Activity, Dietary Intake, and Sleep Duration. PLoS ONE 2015, 10, e0123672. [Google Scholar] [CrossRef]
- Taveras, E.M.; Gillman, M.W.; Kleinman, K.; Rich-Edwards, J.W.; Rifas-Shiman, S.L. Racial/Ethnic Differences in Early-Life Risk Factors for Childhood Obesity. Pediatrics 2010, 125, 686–695. [Google Scholar] [CrossRef]
- Gutiérrez-Fisac, J.L.; Marín-Guerrero, A.; Regidor, E.; Guallar-Castillón, P.; Banegas, J.R.; Rodríguez-Artalejo, F. Length of residence and obesity among immigrants in Spain. Public Health Nutr. 2010, 13, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Hook, J.V.; Baker, E. Big Boys and Little Girls: Gender, Acculturation, and Weight among Young Children of Immigrants. J. Health Soc. Behav. 2010, 51, 200–214. [Google Scholar] [CrossRef] [PubMed]
- Gualdi-Russo, E.; Zaccagni, L.; Manzon, V.S.; Masotti, S.; Rinaldo, N.; Khyatti, M. Obesity and physical activity in children of immigrants. Eur. J. Public Health 2014, 24 (Suppl. 1), 40–46. [Google Scholar] [CrossRef] [PubMed]
- Delisle, H.F.; Vioque, J.; Gil, A. Dietary patterns and quality in West-African immigrants in Madrid. Nutr. J. 2009, 8, 3. [Google Scholar] [CrossRef]
- Van Stralen, M.M.; te Velde, S.J.; van Nassau, F.; Brug, J.; Grammatikaki, E.; Maes, L.; De Bourdeaudhuij, I.; Verbestel, V.; Galcheva, S.; Iotova, V.; et al. Weight status of European preschool children and associations with family demographics and energy balance-related behaviours: A pooled analysis of six European studies: Overweight in European preschoolers. Obes. Rev. 2012, 13, 29–41. [Google Scholar] [CrossRef]
- Wang, Y.; Lim, H. The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int. Rev. Psychiatry 2012, 24, 176–188. [Google Scholar] [CrossRef]
- Khanolkar, A.R.; Sovio, U.; Bartlett, J.W.; Wallby, T.; Koupil, I. Socioeconomic and early-life factors and risk of being overweight or obese in children of Swedish- and foreign-born parents. Pediatr. Res. 2013, 74, 356–363. [Google Scholar] [CrossRef]
- Foets, M.; Labree, W.; van de Mheen, D.; Rutten, F.; Rodenburg, G.; Koopmans, G. Differences in overweight among children from migrant and native origin in the Netherlands. Eur. J. Public Health 2015, 25 (Suppl. 3). [Google Scholar] [CrossRef][Green Version]
- Hancock, C.; Dinsdale, H.; Rutter, H. Are inequalities in child obesity widening? Findings from the National Child Measurement Programm. Obes. Facts 2013, 6, 1–246. [Google Scholar]
- SEF and GEPF Relatório de Imigração, Fronteiras e Asilo; Serviço de Estrangeiros e Fronteiras: Lisboa, Portugal. 2018. Available online: https://sefstat.sef.pt/Docs/Rifa2018.pdf (accessed on 27 June 2019).
- SEF and GEPF Relatório de Imigração, Fronteiras e Asilo; Serviço de Estrangeiros e Fronteiras: Lisboa, Portugal. 2019. Available online: https://sefstat.sef.pt/Docs/Rifa2019.pdf (accessed on 23 June 2020).
- Gonçalves, L.; de Oliveira, M.R.; Pascoal, C.; Pires, A. Sample size for estimating a binomial proportion: Comparison of different methods. J. Appl. Stat. 2012, 39, 2453–2473. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M. International Society for Advancement of Kinanthropometry. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Pedrosa, C.; Correia, F.; Seabra, D.; Oliveira, B.M.; Simoes-Pereira, C.; Vaz-de-Almeida, M.D. Prevalence of overweight and obesity among 7–9-year-old children in Aveiro, Portugal: Comparison between IOTF and CDC references. Public Health Nutr. 2011, 14, 14–19. [Google Scholar] [CrossRef] [PubMed][Green Version]
- DGS Consultas de Vigilância de Saúde Infantil e Juvenil-Actualização das Curvas de Crescimento. No: 05/DSMIA. 2006. Available online: https://www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/circular-normativa-n-05dsmia-de-21022006-pdf.aspx (accessed on 31 May 2013).
- UNICEF. The State of the World’s Children 2019.Children, Food and Nutrition: Growing Well in a Changing World; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- Sergeant, ESG Epitools Epidemiological Calculators. 2018. Available online: http://epitools.ausvet.com.au (accessed on 3 August 2020).
- DasGupta, A.; Cai, T.T.; Brown, L.D. Interval Estimation for a Binomial Proportion. Stat. Sci. 2001, 16, 101–133. [Google Scholar] [CrossRef]
- Gomes, T.; Katzmarzyk, P.; dos Santos, F.; Souza, M.; Pereira, S.; Maia, J.A. Overweight and Obesity in Portuguese Children: Prevalence and Correlates. Int. J. Environ. Res. Public Health 2011, 11, 11398–11417. [Google Scholar] [CrossRef] [PubMed]
- Moreira, P. Overweight and obesity in Portuguese children and adolescents. J. Public Health 2007, 15, 155–161. [Google Scholar] [CrossRef]
- Moreira, P.; Santos, S.; Padrão, P.; Cordeiro, T.; Bessa, M.; Valente, H.; Barros, R.; Teixeira, V.; Mitchell, V.; Lopes, C.; et al. Food Patterns According to Sociodemographics, Physical Activity, Sleeping and Obesity in Portuguese Children. Int. J. Environ. Res. Public Health 2010, 7, 1121–1138. [Google Scholar] [CrossRef]
- Pereira, M.; Nogueira, H.; Padez, C. Association between childhood obesity and environmental characteristics: Testing a multidimensional environment index using census data. Appl. Geogr. 2018, 92, 104–111. [Google Scholar] [CrossRef]
- Viveiro, C.; Brito, S.; Moleiro, P. Sobrepeso e obesidade pediátrica: A realidade portuguesa. Rev. Port. de Saude Publica 2016, 34, 30–37. [Google Scholar] [CrossRef][Green Version]
- Machado-Rodrigues, A.M.; Fernandes, R.; Gama, A.; Mourão, I.; Nogueira, H.; Rosado—Marques, V.; Padez, C. The association of irregular sleep habits with the risk of being overweight/obese in a sample of Portuguese children aged 6–9 years. Am. J. Hum. Biol. 2018, 30, e23126. [Google Scholar] [CrossRef]
- Albuquerque, D.; Nóbrega, C.; Manco, L.; Padez, C. The contribution of genetics and environment to obesity. Br. Med. Bull. 2017, 123, 159–173. [Google Scholar] [CrossRef]
- Camarinha, B.; Graça, P.; Nogueira, P. Prevalence of Pre-Obesity/Obesity in Pre and Basic School Children at Vila Nova de Gaia, Portugal. Acta Médica Port. 2016, 29, 31–40. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tzioumis, E.; Adair, L.S. Childhood dual burden of under- and overnutrition in low- and middle-income countries: A critical review. Food Nutr. Bull. 2014, 35, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Gasparinho, C. Malnutrition and Enteric Infections in Children in Bengo Province, Angola—A Four-Arm Experimental Study. Dissertação para Obtenção de Grau de Doutor; Instituto de Higiene e Medicina Tropical-Universidade Nova de Lisboa: Lisboa, Portugal, 2019. [Google Scholar]
- Goulão, B.; Santos, O.; do Carmo, I. The impact of migration on body weight: A review. Cad. Saude Publica 2015, 31, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Caprio, S.; Daniels, S.R.; Drewnowski, A.; Kaufman, F.R.; Palinkas, L.A.; Rosenbloom, A.L.; Schwimmer, J.B. Influence of Race, Ethnicity, and Culture on Childhood Obesity: Implications for Prevention and Treatment: A consensus statement of Shaping America’s Health and the Obesity Society. Diabetes Care 2008, 31, 2211–2221. [Google Scholar] [CrossRef] [PubMed]
- Rothe, E.; Holt, C.; Kuhn, C.; McAteer, T.; Askari, I.; O’Meara, M.; Sharif, A.; Dexter, W. Barriers to Outdoor Physical Activity in Wintertime among Somali Youth. J. Immigr. Minor. Health 2010, 12, 726–736. [Google Scholar] [CrossRef]
- Cohen, E.; Bernard, J.Y.; Ponty, A.; Ndao, A.; Amougou, N.; Saïd-Mohamed, R.; Pasquet, P. Development and Validation of the Body Size Scale for Assessing Body Weight Perception in African Populations. PLoS ONE 2015, 10, e0138983. [Google Scholar] [CrossRef]
- Rodrigues, D.; Muc, M.; Rodrigues, P.R.M.; Pinto, A.M.; Padez, C. Dietary Patterns and Their Socioeconomic and Behavioral Determinants in 6- to 8-Year-Old Portuguese Children. Ecol. Food Nutr. 2016, 55, 428–441. [Google Scholar] [CrossRef]
- Rodrigues, P.R.M.; Pereira, R.A.; Santana, A.M.S.; Gama, A.; Carvalhal, I.M.; Nogueira, H.; Rosado-Marques, V.; Padez, C. Patterns of lifestyle-related behaviors and parents’ overweight are associated with increased body adiposity in schoolchildren: A cross-sectional study in Portugal. Nutrire 2017, 42, 23. [Google Scholar] [CrossRef]
- Millar, L.; Rowland, B.; Nichols, M.; Swinburn, B.; Bennett, C.; Skouteris, H.; Allender, S. Relationship between raised BMI and sugar sweetened beverage and high fat food consumption among children: Sweet Drinks and High Fat Food and BMI. Obesity 2014, 22, E96–E103. [Google Scholar] [CrossRef]
- Sweeting, H.N. Gendered dimensions of obesity in childhood and adolescence. Nutr. J. 2008, 7, 1. [Google Scholar] [CrossRef]
- Holmboe-Ottesen, G.; Wandel, M. Changes in dietary habits after migration and consequences for health: A focus on South Asians in Europe. Food Nutr. Res. 2016, 56, 18891. [Google Scholar] [CrossRef] [PubMed]
- Terragni, L.; Garnweidner, L.; Pettersen, S.; Mosdøl, A. Migration as a Turning Point in Food Habits: The Early Phase of Dietary Acculturation among Women from South Asian, African, and Middle Eastern Countries Living in Norway. Ecol. Food Nutr. 2014, 53, 273–291. [Google Scholar] [CrossRef] [PubMed]
- Labree, L.J.W.; van de Mheen, H.; Rutte, F.F.H.; Foets, M. Differences in overweight and obesity among children from migrant and native origin: A systematic review of the European literature: Differences in overweight and obesity among children. Obes. Rev. 2011, 12, e535–e547. [Google Scholar] [CrossRef] [PubMed]
- Renzaho, A.M.N.; Burns, C. Post-migration food habits of sub-Saharan African migrants in Victoria: A cross-sectional study. Nutr. Diet. 2006, 63, 91–102. [Google Scholar] [CrossRef]
- Silva, C.; Fassnacht, D.B.; Ali, K.; Gonçalves, S.; Conceição, E.; Vaz, A.; Crosby, R.D.; Machado, P.P. Promoting health behaviour in Portuguese children via Short Message Service: The efficacy of a text-messaging programme. J. Health Psychol. 2015, 20, 806–815. [Google Scholar] [CrossRef]
- Zulfiqar, T.; Strazdins, L.; Banwell, C.; Dinh, H.; D’Este, C. Growing up in Australia: Paradox of overweight/obesity in children of immigrants from low-and-middle -income countries: Obesity in children of Australian Immigrants. Obes. Sci. Pract. 2018, 4, 178–187. [Google Scholar] [CrossRef]
- Rolland-Cachera, M.F. Childhood obesity: Current definitions and recommendations for their use. Int. J. Pediatr. Obes. 2011, 6, 325–331. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Child | Father | Mother | ||||
|---|---|---|---|---|---|---|
| Country of birth | n | (%) | n | (%) | n | (%) |
| Portugal | 707 | 94.4 | 587 | 79.4 | 596 | 80.2 |
| Angola | 2 | 0.3 | 47 | 6.4 | 42 | 5,7 |
| Cape-Verde | 12 | 1.6 | 38 | 5.1 | 32 | 4.3 |
| Guinea-Bissau | 8 | 1.1 | 17 | 2.3 | 18 | 2.4 |
| Mozambique | 0 | 0.0 | 18 | 2.4 | 12 | 1.6 |
| Brazil | 10 | 1.3 | 13 | 1.8 | 14 | 1.9 |
| São Tomé | 2 | 0.3 | 4 | 0.5 | 4 | 0.5 |
| Other countries | 8 | 1.0 | 15 | 2.1 | 25 | 3.4 |
| Variables/Categories | Frequencies | |
|---|---|---|
| n | % | |
| Sex | ||
| Male | 388 | 49.2 |
| Female | 401 | 50.8 |
| Total | 789 | 100.0 |
| Age (in years) | ||
| 5 | 38 | 5.0 |
| 6 | 125 | 16.5 |
| 7 | 121 | 16.0 |
| 8 | 157 | 20.7 |
| 9 | 185 | 24.4 |
| 10 | 104 | 13.7 |
| 11 | 27 | 3.6 |
| Total | 757 | 100.0 |
| Number of siblings | ||
| 0 | 179 | 24.3 |
| 1 | 380 | 51.5 |
| 2 | 106 | 14.8 |
| >=3 | 73 | 9.9 |
| Total | 738 | 100.0 |
| Child’s parents | ||
| Both non-Portuguese | 92 | 12.5 |
| Only one Portuguese | 115 | 15.6 |
| Both Portuguese | 531 | 72.0 |
| Total | 738 | 100.0 |
| Nutritional Status | |||||
|---|---|---|---|---|---|
| Variables | Underweight | Normal Weight | Overweight and Obesity | Total | |
| n (%) | n (%) | n (%) | n | p | |
| Sex | 0.125 | ||||
| Male | 55 (12.2) | 157 (52.0) | 90 (29.8) | 302 | |
| Female | 48 (15.4) | 147 (47.1) | 117 (37.5) | 312 | |
| Total | 103 (16.8) | 304 (49.5) | 207 (33.7) | 614 | |
| Age (in years) | 0.093 | ||||
| 5 | 5 (17.9) | 17 (60.7) | 6 (21.4) | 28 | |
| 6 | 17 (17.0) | 47 (47.0) | 36 (36.0) | 100 | |
| 7 | 11 (10.9) | 61 (60.4) | 29 (28.7) | 101 | |
| 8 | 34 (25.2) | 59 (43.7) | 42 (31.1) | 135 | |
| 9 | 17 (12.2) | 68 (48.9) | 54 (38.8) | 139 | |
| 10 | 11 (17.5) | 34 (54.0) | 18 (28.6) | 63 | |
| 11 | 3 (18.8) | 6 (37.5) | 7 (43.8) | 16 | |
| Total | 98 (16.8) | 292 (50.2) | 192 (33.0) | 582 | |
| Number of siblings | 0.261 | ||||
| 0 | 16 (11.2) | 74 (51.7) | 53 (37.1) | 143 | |
| 1 | 55 (18.6) | 142 (48.1) | 98 (33.2) | 295 | |
| 2 | 14 (17.7) | 46 (58.2) | 19 (24.1) | 79 | |
| ≥3 | 10 (19.2) | 24 (46.2) | 18 (34.6) | 52 | |
| Total | 95 (16.7) | 286 (50.3) | 188 (33.0) | 569 | |
| Child’s parents | 0.978 | ||||
| Both non-Portuguese | 11 (17.2) | 32 (50.0) | 21 (32.8) | 64 | |
| Only one Portuguese | 15 (16.7) | 47 (52.2) | 28 (31.1) | 90 | |
| Both Portuguese | 69 (16.7) | 201 (48.8) | 142 (34.5) | 412 | |
| Total | 95 (16.8) | 280 (49.5) | 191 (33.7) | 566 | |
| Female | Male | |||||
|---|---|---|---|---|---|---|
| Variables (units) | Immigrant Background (n = 78) | Native (n = 212) | p | Immigrant Background (n = 77) | Native (n = 200) | p |
| Decimal age (years) | 8.61 ± 1.49 | 8.81 ± 1.34 | 0.303 | 8.80 ± 1.49 | 8.68 ± 1.46 | 0.550 |
| Weight (kg) | 31.90 ± 9.03 | 32.07 ± 9.15 | 0.893 | 32.20 ± 11.18 | 31.29 ± 9.56 | 0.501 |
| Height (cm) | 133.88 ± 11.02 | 133.35 ± 9.59 | 0.689 | 134.02 ± 10.68 | 132.97 ± 10.25 | 0.449 |
| Sitting Height (cm) | 70.38 ± 4.90 | 70.80 ± 4.54 | 0.491 | 70.79 ± 4.63 | 70.92 ± 4.68 | 0.841 |
| BMI (kg/cm2) | 17.55 ± 3.48 | 17.77 ± 3.51 | 0.632 | 17.53 ± 3.94 | 17.36 ± 3.32 | 0.708 |
| Body fat (%) | 20.30 ± 8.30 | 22.57 ± 9.51 | 0.063 | 18.59 ± 10.29 | 18.33 ± 8.81 | 0.834 |
| Skinfolds | ||||||
| Tricipital | 12.99 ± 5.29 | 14.56 ± 6.22 | 0.032a | 11.88 ± 6.50 | 11.58 ± 5.72 | 0.701 |
| Thigh (mm) | 20.19 ± 8.22 | 22.61 ± 9.02 | 0.039 | 17.81 ± 8.89 | 18.14 ± 8.87 | 0.785 |
| Calf (mm) | 13.71 ± 6.01 | 15.10 ± 6.57 | 0.104 | 12.21 ± 7.13 | 12.14 ± 6.55 | 0.930 |
| Subscapular (mm) | 9.56 ± 5.77 | 10.55 ± 6.83 | 0.258 | 9.10 ± 6.82 | 8.32 ± 5.90 | 0.343 |
| Suprailliac (mm) | 9.95 ± 6.23 | 11.47 ± 7.27 | 0.101 | 9.37 ± 7.91 | 8.59 ± 7.18 | 0.429 |
| Circumferences | ||||||
| Relaxed arm | 20.64 ± 3.30 | 21.42 ± 3.66 | 0.100 | 20.44 ± 4.11 | 20.39 ± 3.93 | 0.925 |
| Tensed arm | 21.33 ± 3.19 | 21.98 ± 3.45 | 0.153 | 21.36 ± 3.89 | 21.24 ± 3.56 | 0.807 |
| Calf (cm) | 28.25 ± 3.75 | 28.74 ± 3.76 | 0.322 | 28.35 ± 4.05 | 28.15 ± 5.17 | 0.760 |
| Waist (cm) | 58.69 ± 7.20 | 60.41 ± 8.10 | 0.099 | 60.38 ± 9.19 | 60.37 ± 7.93 | 0.992 |
| Hip (cm) | 71.87 ± 9.21 | 72.55 ± 9.43 | 0.588 | 71.24 ± 10.72 | 70.36 ± 10.00 | 0.520 |
| Biepicondylar Breadths | ||||||
| Humerus (cm) | 5.17 ± 0.46 | 5.19 ± 0.47 | 0.854 | 5.36 ± 0.55 | 5.29 ± 0.50 | 0.355 |
| Femur (cm) | 7.75 ± 0.66 | 7.71 ± 0.64 | 0.710 | 8.1 6 ± 0.79 | 8.08 ± 0.69 | 0.415 |
| Other measures | ||||||
| Waist-to-height ratio | 0.45 ± 0.05 | 0.45 ± 0.04 | 0.035 | 0.45 ± 0.05 | 0.45 ± 0.04 | 0.568 |
| Waist-to-hip ratio | 0.82 ± 0.05 | 0.84 ± 0.07 | 0.062 | 0.85 ± 0.05 | >0.87 ± 0.14 | 0.311 |
| Arm muscle area | 218.46 ± 53.56 | 226.34 ± 57.42 | 0.293 | 224.03 ± 67.59 | 225.40 ± 72.38 | 0.885 |
| Arm fat area | 124.44 ± 66.94 | 144.32 ± 80.17 | 0.071 b | 117.15 ± 88.26 | 113.09 ± 76.06 | 0.704 |
| Variables | Total and by Sex (n) | Percentage of Affirmative Responses | χ2 (p) | ||
|---|---|---|---|---|---|
| Both Non-Portuguese (n = 92) | Only One Portuguese (n = 115) | Both Portuguese (n = 531) | |||
| Practice sports outside school | Total (716) | 33.0 | 41.7 | 50.9 | 11.32 (0.003) |
| Female (364) | 15.2 | 28.8 | 43.2 | 15.31 (0.001) | |
| Male (352) | 52.4 | 55.7 | 58.7 | 0.69 (0.707) | |
| Housekeeping tasks | Total (603) | 87.0 | 68.8 | 71.2 | 9.23 (0.010) |
| Female (323) | 89.5 | 74.1 | 73.6 | 4.53 (0.104) | |
| Male (280) | 84.6 | 61.9 | 68.3 | 5.48 (0.064) | |
| Eggs consumption * | Total (661) | 65.1 | 38.7 | 39.0 | 20.23 (<0.001) |
| Female (333) | 70.0 | 38.2 | 40.3 | 13.03 (0.010) | |
| Male (328) | 60.5 | 39.2 | 37.6 | 7.92 (0.019) | |
| French fries * | Total (664) | 58.0 | 23.6 | 33.5 | 25.41 (<0.001) |
| Female (336) | 64.1 | 31.1 | 33.9 | 18.68 (<0.001) | |
| Male (328) | 52.4 | 22.0 | 36.0 | 9.15 (0.001) | |
| Fast food * | Total (659) | 38.2 | 22.0 | 22.1 | 9.48 (0.009) |
| Female (334) | 42.1 | 23.6 | 19.9 | 9.12 (0.010) | |
| Male (325) | 34.2 | 20.4 | 24.4 | 2.32 (0.313) | |
| Sweets * | Total (680) | 67.9 | 39.6 | 43.4 | 18.71 (<0.001) |
| Female (349) | 75.0 | 41.1 | 41.5 | 16.12 (<0.001) | |
| Male (331) | 61.0 | 38.0 | 45.4 | 5.01 (0.082) | |
| Soft drinks * | Total (685) | 72.1 | 44.9 | 51.4 | 15.92 (<0.001) |
| Female (348) | 72.1 | 51.8 | 49.4 | 7.59 (0.022) | |
| Male (337) | 72.1 | 37.3 | 53.5 | 11.38 (0.003) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, S.; Gonçalves, L. Overweight and Obesity in Children of Immigrant Versus Native Parents: Exploring a Local Setting in Portugal. Int. J. Environ. Res. Public Health 2020, 17, 7897. https://doi.org/10.3390/ijerph17217897
Moreira S, Gonçalves L. Overweight and Obesity in Children of Immigrant Versus Native Parents: Exploring a Local Setting in Portugal. International Journal of Environmental Research and Public Health. 2020; 17(21):7897. https://doi.org/10.3390/ijerph17217897
Chicago/Turabian StyleMoreira, Susana, and Luzia Gonçalves. 2020. "Overweight and Obesity in Children of Immigrant Versus Native Parents: Exploring a Local Setting in Portugal" International Journal of Environmental Research and Public Health 17, no. 21: 7897. https://doi.org/10.3390/ijerph17217897
APA StyleMoreira, S., & Gonçalves, L. (2020). Overweight and Obesity in Children of Immigrant Versus Native Parents: Exploring a Local Setting in Portugal. International Journal of Environmental Research and Public Health, 17(21), 7897. https://doi.org/10.3390/ijerph17217897