Cardiorespiratory Fitness is Inversely Associated with Risk of Low Bone Mineral Density in Older Korean Men


Abstract
:1. Introduction
2. Materials and Methods
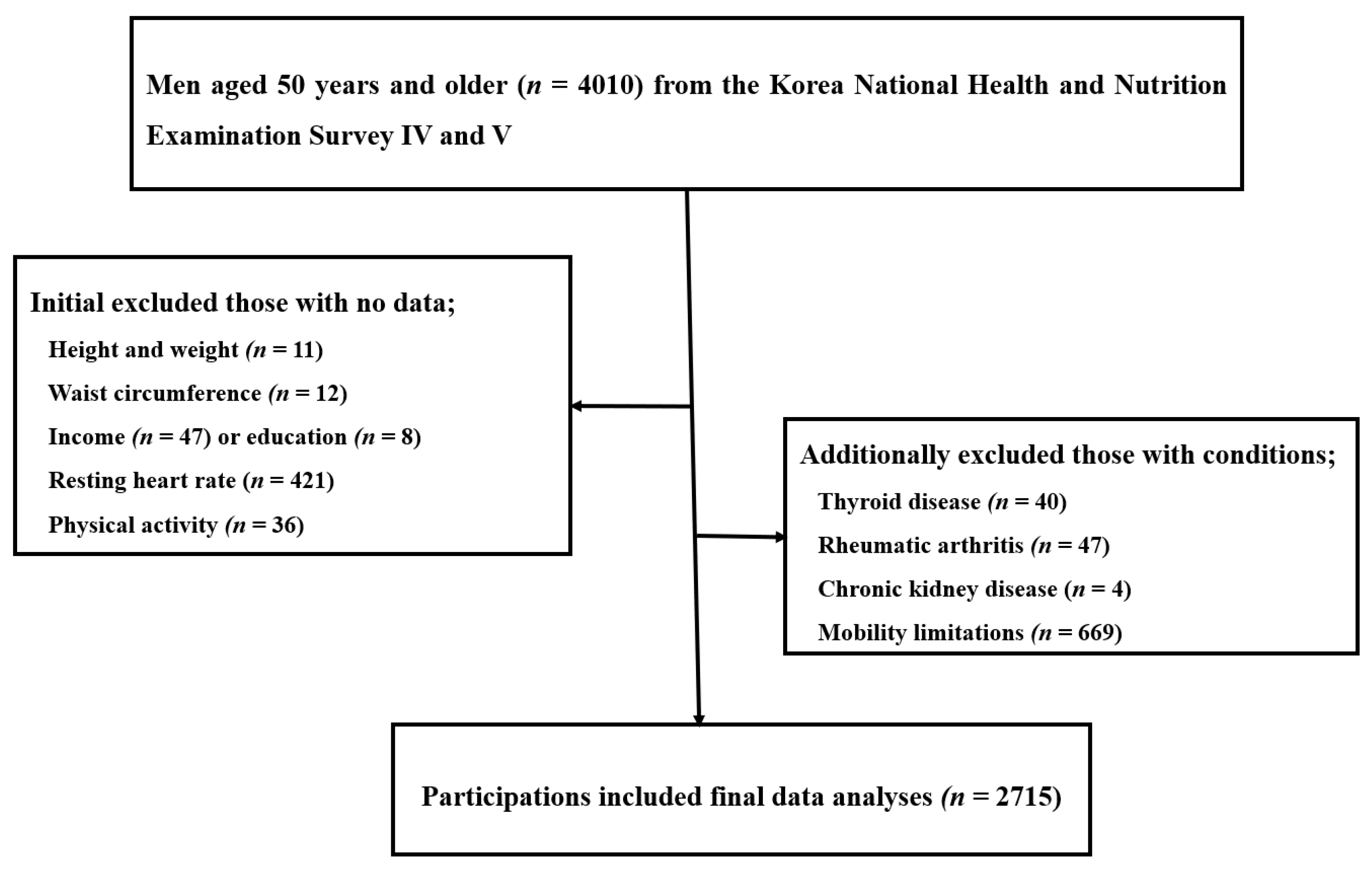
2.1. Data Source and Study Participants
2.2. Study Variables
2.2.1. Assessment of Bone Mineral Density
2.2.2. Estimation of Cardiorespiratory Fitness
2.2.3. Determination of Covariates
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, E.Y.; Kim, D.; Kim, K.M.; Kim, K.J.; Choi, H.S.; Rhee, Y.; Lim, S.-K. Age-related bone mineral density patterns in Koreans (KNHANES IV). J. Clin. Endocrinol. Metab. 2012, 97, 3310–3318. [Google Scholar] [PubMed] [Green Version]
- Kim, J.-W.; Ha, Y.-C.; Lee, Y.-K. Factors affecting bone mineral density measurement after fracture in South Korea. J. Bone Metab. 2017, 24, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, H.-D.; Hong, J.-Y.; Han, K.; Lee, J.C.; Shink, B.-J.; Choi, S.-W.; Suh, S.-W.; Yang, J.-H.; Park, S.-Y.; Bang, C. Relationship between bone mineral density and alcohol intake: A nationwide health survey analysis of postmenopausal women. PLoS ONE 2017, 12, e0180132. [Google Scholar] [CrossRef] [Green Version]
- Ha, J.; Kim, A.-A.; Lim, K.; Shin, S. The association of potassium intake with bone mineral density and the prevalence of osteoporosis among older Korean adults. Nutr. Res. Pract. 2020, 14, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; Park, Y. The association between the consumption of fish/shellfish and the risk of osteoporosis in men and postmenopausal women aged 50 years or older. Nutrients 2016, 8, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, K.-O.; Kim, M.-J.; Ly, S.-Y. Association between vitamin D intake and bone mineral density in Koreans aged ≥ 50 years: Analysis of the 2009 Korea National Health and Nutrition Examination Survey using a newly established vitamin D database. Nutr. Res. Pract. 2019, 13, 115–125. [Google Scholar] [CrossRef]
- Chang, H.K.; Chang, D.-G.; Myong, J.-P.; Kim, J.-H.; Lee, S.-J.; Lee, Y.S.; Lee, H.-N.; Lee, K.H.; Park, D.C.; Kim, C.J.; et al. Bone mineral density among Korean females aged 20–50 years: Influence of age at menarche (The Korea National Health and Nutrition Examination Survey 2008–2011). Osteoporos. Int. 2017, 28, 2129–2136. [Google Scholar] [CrossRef]
- Lee, S.H.; Kwon, H.-Y. Prevalence of Osteoporosis in Korean Patients with Chronic Obstructive Pulmonary Disease and Their Health-related Quality of Life According to the Korea National Health and Nutrition Examination Survey 2008–2011. J. Bone Metab. 2017, 24, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.-S.; Bae, S.-H.; Lee, S.H.; Lee, J.; Lee, D.R. New Reference Data on Bone Mineral Density and the Prevalence of Osteoporosis in Korean Adults Aged 50 Years or Older: The Korea National Health and Nutrition Examination Survey 2008–2010. J. Korean Med. Sci. 2014, 29, 1514–1522. [Google Scholar] [CrossRef] [Green Version]
- Park, E.J.; Joo, I.W.; Jang, M.-J.; Kim, Y.T.; Oh, K.; Oh, H.J. Prevalence of osteoporosis in the Korean population based on Korea National Health and Nutrition Examination Survey (KNHANES), 2008–2011. Yonsei Med. J. 2014, 55, 1049–1057. [Google Scholar] [CrossRef]
- Ha, Y.-C.; Park, Y.-G.; Nam, K.-W.; Kim, S.-R. Trend in hip fracture incidence and mortality in Korea: A prospective cohort study from 2002 to 2011. J. Korean Med. Sci. 2015, 30, 483–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, H.-K.; Park, C.; Jang, S.; Jang, S.; Lee, Y.-K.; Ha, Y.-C. Incidence and mortality following hip fracture in Korea. J. Korean Med Sci. 2011, 26, 1087–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.; Han, K. The incidence of hip fracture and mortality rate after hip fracture in Korea: A nationwide population-based cohort study. Osteoporos. Sarcopenia 2019, 5, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.-C. Epidemiology of osteoporosis in Korea. J. Korean Med. Assoc. 2016, 59, 836–841. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.Y.; Jang, S.; Park, C.M.; Lee, A.; Lee, Y.K.; Kim, H.Y.; Cho, E.H.; Ha, Y.C. Trends of incidence, mortality, and future projection of spinal fractures in Korea using nationwide claims data. J. Korean Med. Sci. 2016, 31, 801–805. [Google Scholar] [CrossRef] [Green Version]
- Ha, Y.C.; Kim, T.Y.; Lee, A.; Lee, Y.K.; Kim, H.Y.; Kim, J.H.; Park, C.M.; Jang, S. Current trends and future projections of hip fracture in South Korea using nationwide claims data. Osteoporos. Int. 2016, 27, 2603–2609. [Google Scholar] [CrossRef]
- Kohrt, W.M.; Bloomfield, S.A.; Little, K.D.; Nelson, M.E.; Yingling, V.R. American College of Sports Medicine Position Stand: Physical activity and bone health. Med. Sci. Sports Exerc. 2004, 36, 1985–1996. [Google Scholar] [CrossRef] [Green Version]
- Moayyeri, A. The association between physical activity and osteoporotic fractures: A review of the evidence and implications for future research. Ann. Epidemiol. 2008, 18, 827–835. [Google Scholar] [CrossRef]
- DeFina, L.F.; Leonard, D.; Willis, B.L.; Barlow, C.E.; Finley, C.E.; Jenkins, M.R.; Pence, B.C.; Zhang, Y.; Chyu, M.-C.; Lewiecki, E.M.; et al. High cardiorespiratory fitness is associated with reduced risk of low bone density in postmenopausal women. J. Women’s Health 2016, 25, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Wainstein, H.M.; Feldman, M.; Shen, C.L.; Leonard, D.; Willis, B.L.; Finley, C.E.; Gruntmanis, U.; DeFina, L.F. The Relationship Between Cardiorespiratory Fitness and Bone Mineral Density in Men: A Cross-sectional Study. Mayo Clin. Proc. 2016, 91, 726–734. [Google Scholar] [CrossRef]
- Lee, I.; Kim, J.; Kang, H. Estimated cardiorespiratory fitness attenuates the impacts of sarcopenia and obesity on non-alcoholic fatty liver in Korean adults. Int. J. Environ. Res. Public Health 2020, 17, 3902. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R.M.; Jackson, A.S. Exercise Concepts, Calculations, and Computer Applications; Benchmark Press: Carmel, IN, USA, 1990; pp. 95–109. [Google Scholar]
- Schwarz, P.; Jørgensen, N.; Nielsen, B.; Laursen, A.S.; Linneberg, A.; Aadahl, M. Muscle strength, power and cardiorespiratory fitness are associated with bone mineral density in men aged 31–60 years. Scan. J. Public Health 2014, 42, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, É.R.; Maia, J.A.; Beunen, G.P.; Blimkie, C.J.; Rodrigues, A.L.; Freitas, D.L. Functional fitness and bone mineral density in the elderly. Arch. Osteoporos. 2012, 7, 75–85. [Google Scholar] [CrossRef]
- Kelley, G.A. Exercise and regional bone mineral density in postmenopausal women: A meta-analytic review of randomized trials. Am. J. Phys. Med. Rehabil. 1998, 77, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Willett, W.; Colditz, G. Walking and leisure time activity and risk of hip fracture in postmenopausal women. JAMA 2002, 288, 2300–2306. [Google Scholar] [CrossRef] [Green Version]
- Kelley, G.A.; Kelley, K.S.; Tran, Z.V. Exercise and bone mineral density in men: A meta-analysis. J. Appl. Physiol. 2000, 88, 1730–1736. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S.; Kohrt, W.M. Exercise and bone mineral density in men: A meta-analysis of randomized controlled trials. Bone 2013, 53, 103–111. [Google Scholar] [CrossRef]
- Stewart, K.J.; Deregis, J.R.; Turner, K.L.; Bacher, A.C.; Sung, J.; Hees, P.S.; Tayback, M.; Ouyang, P. Fitness, fatness and activity as predictors of bone mineral density in older persons. J. Intern. Med. 2002, 252, 381–388. [Google Scholar] [CrossRef]
- Huuskonen, J.; Vaisanen, S.B.; Kroger, H.; Jurvelin, C.; Bouchard, C.; Alhava, E.; Rauramaa, R. Determinants of bone mineral density in middle aged men: A population-based study. Osteoporos Int. 2000, 11, 702–708. [Google Scholar] [CrossRef]
- Huuskonen, J.; Vaisanen, S.B.; Kroger, H.; Jurvelin, J.S.; Alhava, E.; Rauramaa, R. Regular physical exercise and bone mineral density: A four-year controlled randomized trial in middle-aged men: The DNASCO study. Osteoporos. Int. 2001, 12, 349–355. [Google Scholar] [PubMed]
- Baxter-Jones, A.D.; Kontulainen, S.A.; Faulkner, R.A.; Bailey, D.A. A longitudinal study of the relationship of physical activity to bone mineral accrual from adolescence to young adulthood. Bone 2008, 43, 1101–1107. [Google Scholar]
- Nilsson, M.; Ohlsson, C.; Mellström, D.; Lorentzon, M. Previous sport activity during childhood and adolescence is associated with increased cortical bone size in young adult men. J. Bone Miner. Res. 2009, 24, 125–133. [Google Scholar] [PubMed]
- Michaelsson, K.; Olofsson, H.; Jensevik, K.; Larsson, S.; Mallmin, H.; Berglund, L.; Vessby, B.; Melhus, H. Leisure physical activity and the risk of fracture in men. PLoS Med. 2007, 4, e199. [Google Scholar] [CrossRef]
- Han, S.S.; Kim, M.; Lee, S.M.; Lee, J.P.; Kim, S.; Joo, K.W.; Lim, C.S.; Kim, Y.S.; Kim, D.K. Association between body fat and vitamin D status in Korean adults. Asia Pac. J. Clin. Nutr. 2014, 23, 65–75. [Google Scholar]
- Kim, H.; Kim, H.; Kwon, O.; Park, H. Food and nutrient intake level by the risk of osteoporosis and cardiovascular disease in postmenopausal women: The use of the 5th Korean National Health and Nutrition Examination Surveys (2010–2011). Korean J. Community Nutr. 2019, 24, 152–162. [Google Scholar]
- Yoon, J.-S.; Song, M.-K. Vitamin D intake, Outdoor Activity Time and Serum 25-OH Vitamin D Concentrations of Korean Postmenopausal Women by Season and by Age. Korean J. Community Nutr. 2015, 20, 120–128. [Google Scholar]
- Joh, H.-K.; Lim, C.S.; Cho, B. Lifestyle and dietary factors associated with serum 25-hydroxyvitamin D levels in Korean young adults. J. Korean Med Sci. 2015, 30, 1110–1120. [Google Scholar]
- Khan, K.; McKay, H.; Kannus, P.; Bailey, D.; Wark, J.; Bennell, K. Physical Activity and Bone Health; Human Kinetics: Champaign, IL, USA, 2001. [Google Scholar]

{kind=link}
| Variables | All (n = 2715) | eCRF Levels | p for Linear Trends | ||
|---|---|---|---|---|---|
| Low (n = 678) | Middle (n = 1351) | High (n = 686) | |||
| Anthropometrics | |||||
| Age (years) | 62.5 ± 8.6 | 70.6 ± 7.6 | 61.5 ± 7.6 | 56.4 ± 5.2 | <0.001 |
| Body mass index (kg/m2) | 23.8 ± 2.9 | 24.2 ± 3.1 | 23.8 ± 3.0 | 23.3 ± 2.5 | <0.001 |
| Waist circumference (cm) | 85.2 ± 8.5 | 87.5 ± 9.3 | 85.3 ± 8.5 | 82.9 ± 7.2 | <0.001 |
| Resting heart rate (beats/min) | 70 ± 9 | 72 ± 10 | 70 ± 9 | 67 ± 8 | <0.001 |
| Heavy alcohol drinkers, n (%) | 609 (22.4) | 232 (38.1) | 265 (43.5) | 112 (18.4) | <0.001 |
| Current smokers, n (%) | 1589 (70.2) | 366 (23.0) | 779 (40.9) | 444 (27.9) | <0.001 |
| Socio-economic Status | |||||
| Education, n (%) | <0.001 | ||||
| Elementary | 873 (32.3) | 317 (36.3) | 407 (46.5) | 150 (17.2) | |
| Middle and high schools | 1323 (48.7) | 271 (20.5) | 682 (51.5) | 370 (28.0) | |
| College or higher | 519 (19.1) | 90 (17.3) | 263 (50.7) | 166 (32.0) | |
| Household income (won) | 340 ± 1172 | 210 ± 405 | 340 ± 778 | 469 ± 2015 | <0.001 |
| Physical Activity and Fitness | |||||
| Physical activity score | 3.36 ± 1.55 | 1.83 ± 0.54 | 3.31 ± 1.48 | 4.95 ± 0.21 | <0.001 |
| eCRF (METs) | 10.0 ± 1.7 | 7.9 ± 0.6 | 10.0 ± 0.9 | 12.2 ± 0.5 | <0.001 |
| Serum Vitamin and Hormones | |||||
| Vitamin D (ng/mL) | 21.5 ± 7.5 | 21.1 ± 7.7 | 21.3 ± 7.3 | 22.1 ± 7.6 | 0.004 |
| Parathyroid hormone (pg/mL) | 65.5 ± 26.4 | 69.1 ± 31.7 | 65.0 ± 24.6 | 63.5 ± 24.1 | <0.001 |
| Nutrient intake | |||||
| Energy (kcal/day) | 2139 ± 789 | 1904 ± 655 | 2166 ± 803 | 2340 ± 828 | <0.001 |
| Protein (g/day) | 75 ± 35 | 64 ± 30 | 76 ± 36 | 83 ± 36 | <0.001 |
| Calcium (mg/day) | 554 ± 330 | 488 ± 361 | 575 ± 399 | 585 ± 330 | <0.001 |
| Vitamin A (μgRE) | 847 ± 876 | 706 ± 770 | 864 ± 811 | 966 ± 1,074 | <0.001 |
| Vitamin C (mg/day) | 111 ± 92 | 94 ± 79 | 116 ± 99 | 120 ± 88 | <0.001 |
| Variables | All (n = 2715) | eCRF Levels | p for Trends | ||
|---|---|---|---|---|---|
| Low (n = 678) | Middle (n = 1351) | High (n = 686) | |||
| BMD (g/cm2) | 0.75 ± 0.11 | 0.71 ± 0.12 | 0.75 ± 0.12 | 0.78 ± 0.11 | <0.001 |
| T-score (mean ± SD) | −0.76 ± 0.95 | −1.06 ± 0.98 | −0.74 ± 0.98 | −0.51 ± 0.88 | <0.001 |
| Osteopenia (n, [%]) | 1044 (38.5) | 320 (47.2) | 524 (38.8) | 200 (29.2) | <0.001 |
| Osteoporosis (n, [%]) | 71 (2.6) | 41 (6.0) | 25 (1.9) | 5 (0.7) | <0.001 |
| Low BMD (n, [%]) | 1115 (41.1) | 361 (53.2) | 549 (40.6) | 205 (29.9) | <0.001 |
| Normal (n, [%]) | 1600 (60.5) | 317 (49.8) | 802 (60.5) | 481 (70.6) | <0.001 |
| Variables | Low eCRF | Middle eCRF | p Value | High eCRF | p Value |
|---|---|---|---|---|---|
| Osteopenia | |||||
| Crude OR (95% CI) | 1 | 0.647 (0.535–0.783) | <0.001 | 0.412 (0.328–0.517) | <0.001 |
| Adjusted a OR (95% CI) | 1 | 0.923 (0.703–1.213) | 0.565 | 0.692 (0.480–0.998) | 0.049 |
| Osteoporosis | |||||
| Crude OR (95% CI) | 1 | 0.241 (0.144–0.403) | 0.001 | 0.080 (0.031–0.206) | 0.001 |
| Adjusted a OR (95% CI) | 1 | 0.708 (0.308–1.632) | 0.418 | 0.354 (0.089–1.413) | 0.142 |
| Low Bone Mineral Density | |||||
| Crude OR (95% CI) | 1 | 0.601 (0.499–0.724) | <0.001 | 0.374 (0.300–0.407) | <0.001 |
| Adjusted a OR (95% CI) | 1 | 0.905 (0.691–1.184) | 0.467 | 0.669 (0.497–0.966) | 0.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.; Kim, J.; Kang, H. Cardiorespiratory Fitness is Inversely Associated with Risk of Low Bone Mineral Density in Older Korean Men. Int. J. Environ. Res. Public Health 2020, 17, 7907. https://doi.org/10.3390/ijerph17217907
Lee I, Kim J, Kang H. Cardiorespiratory Fitness is Inversely Associated with Risk of Low Bone Mineral Density in Older Korean Men. International Journal of Environmental Research and Public Health. 2020; 17(21):7907. https://doi.org/10.3390/ijerph17217907
Chicago/Turabian StyleLee, Inhwan, Jeonghyeon Kim, and Hyunsik Kang. 2020. "Cardiorespiratory Fitness is Inversely Associated with Risk of Low Bone Mineral Density in Older Korean Men" International Journal of Environmental Research and Public Health 17, no. 21: 7907. https://doi.org/10.3390/ijerph17217907