1. Introduction
The tenth revision of the International Classification of Diseases, Clinical Modification (ICD-10-CM), assigns the M79.7 to Fibromyalgia (FM) and defines the disease, together with fibromyositis, fibrositis and myofibrositis, as a chronic multisymptomatic disease of unknown etiology. FM presents with low pain threshold, muscle stiffness and tenderness, often accompanied with sleep disturbances, general fatigue, headaches and memory loss [
1,
2,
3,
4]. Similarly, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) was classified with the code R53.82, or G93.3 if post-viral. The disease is described as an acquired, complex syndrome characterized by exercise-induced exacerbated fatigue, also known as PEM (post-exertional malaise), flu-like symptoms, sleep disturbances, cognitive dysfunction and orthostatic intolerance, in conjunction with others [
5,
6]. Some authors have posited that these two diseases are part of the same somatic syndrome, based on overlapping symptomatology [
7,
8,
9]; some analytical coincidences like the increased lactate levels in ventricular cerebrospinal fluid, reported by B. Natelson et al. [
10], and epidemiologic overlaps [
11]. However, a list of differences in clinical and biological parameters, including PEM and autonomic function; hormone unbalance and differential cytokine, microRNA and gene expression profiles [
12,
13,
14,
15,
16,
17,
18,
19], suggests that the underlying pathophysiology in FM differs from that of ME/CFS [
10].
Current pharmacological treatments for FM and/or CFS/ME patients are exclusively directed to palliate symptoms, since clinical trials have so far failed to provide overall benefits without associated harms [
20,
21,
22]. In addition, polypharmacy often leads to patient deterioration, particularly for those suffering from chemical sensitivity, and extended drug use translates into patient desensitization and lack of drug-response. Non-pharmacological options are mainly dealing with CBT/GET (cognitive behavioral therapy by itself or combined with gradual exercise therapy). FM patients can engage in moderate to vigorous exercise; however, they often experience difficulties performing and adhering to even moderate intensity regimes because of increased pain symptoms [
23]. On another side, the PACE trials design and outcomes continue under debate [
24,
25].
Physiotherapy-based treatments, manual therapy (MT) included, might provide exercise-like effects on treated tissues, by inducing blood flow and/or increased muscle tone, without demanding physical efforts from the patient and therefore, contrary to GET, should not compromise patient’s health.
MT involves the manipulation of soft tissues and joints to relieve pain, reduce inflammation, release muscle contractures and increase the range of motion, to restore health. Massage maneuvers include pressures, rubbing, friction, kneading and vibrations, among others. Although different benefits are attributed to particular maneuvers, i.e., increased vagal tone by moderate pressures [
26,
27], and the duration, frequency, treated areas, repetition and pressures are known to be key on the downstream effects, to date, MT protocols are still poorly defined.
Despite this lack of protocol rigor, a recent systematic review and a meta-analysis of RCTs (randomized clinical trials) show that MT improves pain, anxiety and depression in FM patients [
28,
29], suggesting that physiotherapy treatments based on manual maneuvers could be used for therapeutic purposes by themselves or in combination with current symptomatic pharmacological treatments, as part of integrative medicine programs. Inspired by this idea, our group reviewed clinical and research evidence of MT-based therapeutics with a focus on the role of the differential effects of pressure-therapeutics [
30], finding that medium load pressure massage (4.5
N), using a particular frequency and repetitions as described by Dupont-Vergesteegden´s group [
31], can be used as an intervention to aid in the regrowth of muscle lost during immobilization and in sedentary deconditioned individuals, such as severely affected FM and/or CFS/ME patients. At the same time, and similarly to CBT and mindfulness, MT might engage patient’s mind into relaxation, boosting happiness and perhaps immune, hormonal and neurotransmitter responses [
24,
32,
33,
34,
35].
Documented with results from the clinic and those obtained from animal models and mimetic devices [
30], our group developed a custom pressure-controlled MT protocol for the treatment of FM and evaluated patient’s response to this therapeutic program in the context of the registered Clinical Trial (CT) NCT04174300. Outcome measures included the use of standardized instruments, pressure-point threshold (PPT) digital recordings and scores from a custom questionnaire (CQ) created towards gathering patient’s self-impressions of the treatment. The aim of this study was to assess the benefits of our pressure-controlled MT protocol into alleviating FM symptoms according to questionnaire scores of the standardized instruments: FIQ (Fibromyalgia Impact Questionnaire) [
36,
37], MFI (Multi-Fatigue Inventory) [
38], SF-36 [
39] and our CQ. In addition, improvement of patient hyperalgesia/allodynia was determined by increased PPTs in the 18 FM tenderpoints described by the ACR1990 FM diagnostic criteria [
2].
Furthermore, since we are interested in identifying the subjacent molecular mechanisms involved in MT mechano-transduction associated therapeutic effects, a biophysical process by which cells are capable of sensing their environment and of translating cues into biochemical signals [
40,
41], we used this CT as a platform to generate a collection of blood fractions for future gene expression inquiries, as depicted here.
4. Discussion
The possibility of drug-free therapeutics seems highly attractive, particularly for diseases like FM and ME/CFS that appear often associated to varied comorbidities, multiple chemical hypersensitivity included [
49]. Moreover, for the expected low undesired secondary effects and the avoidance of harmful interactions.
The rationale behind the proposal of using pressure-controlled MT to treat FM and ME/CFS is extensively presented and carefully discussed in a review paper published by our group about 2 years ago [
30]. Some of the data supporting this proposal include several systematic reviews and meta-analysis of RCTs concluding that MT leads to beneficial effects on improving pain, anxiety and depression [
28,
30,
50]. Another meta-analysis, including 140 studies has shown that MT reduces DOMS (delayed onset muscle soreness) and fatigue after exercise, more effectively than compression garment, electrostimulation, stretching, immersion or cryotherapy, as evidenced by decrease in the muscle damage marker creatine kinase (CK) and in the inflammation markers interleukin-6 (IL-6) and C-reactive protein [
51], and therefore further supports MT as a potential therapy for FM.
MT activates mechano-transduction signaling pathways, induces mitochondria biogenesis signaling and diminishes the levels of inflammatory cytokines, such as the interleukin IL-6 and TNF (tumor necrosis factor)-α [
52], changes that could benefit FM and CFS/ME patients [
53,
54]. Application of MT to soft and connective tissues leads to biochemical changes, at the time that allows local nociceptive and inflammatory mediators be reabsorbed by raising muscle blood and lymph circulation [
55]. In fact, the use of pressure mimetic devices on animal models has shown that the intensity of therapeutic forces is determinant to obtain hypoalgesia effects [
31,
56]. Waters-Banker et al., by assaying low (1.4 N), medium (4.5 N) and high (11 N) loadings, found that high loadings drive to increased extracellular space, possibly as result of damage and edema of the muscle. While medium loading induced anti-inflammatory molecular changes and induced muscle regeneration, low pressures did not [
31], indicative of the pertinence of a moderate controlled pressure MT protocol as the choice with therapeutic potential.
In compliance with these findings, some MT studies have strived to control the applied load, towards effect replicability, using approaches like patient pain feed-back scales, as for example includes the recently published work by Nadal-Nicolás et al. [
57]. Since pain sensitivity varies across FM patients, we thought that pressure monitorization performed by a single pre-trained collegiate physiotherapist might increase inter-assay consistency. For this purpose, we developed a pressure-sensitive dispositive with built-in sensors that was used to ensure medium load MT protocols by self-training (please see Experimental Procedures for further details).
In line with our expectations, our medium load-pressure MT protocol consisting of 8-sessions of 25 min twice weekly for 4 consecutive days on alternate weekdays (
Figure 1), led to improvement of patient pain thresholds, as measured by the standard FIQ and SF-36 questionnaires (
Table 3). FIQ total and Overload were the most improved items, together with SF-36 Bodily pain. Similarly, CQ results showed most benefits for response immediately after treatment and upon completion of the whole set of 8-sessions (
p < 0.05), in contrast to 24 h after treatment, when patients reported worse condition of the treated region (
Table 4). It is possible that at that time (24 h post-treatment) some pressure-induced events lead to this feeling. It may be of interest to monitor patient evolution after treatment more closely in future trials. By contrast, no improvement was registered on patient’s fatigue, either by MFI or CQ scores (
Table 3 and
Table 4). As per the stability of the benefits obtained in pain reduction and overall status, we found that the effects persisted after a period free of treatment of 30-day (
Table 3 and
Table 4), at least to a certain extent. Longer patient follow ups are granted by continuation studies to determine MT effects washout period.
In agreement with the described questionnaire-assessed findings, differential PPTs measures obtained with a digital algometer, as described in Experimental Procedures, further confirmed significant improvement of patient’s hyperalgesia/allodynia in two of the treated sets of tender points, the Trapezius and the Gluteal. Only the Low cervical appear to worsen in the overall group assessment (
Table 2). None of the untreated point PPTs were majorly affected with the only exception of the right Second rib, when the whole group was considered (
n = 38), suggesting that the improvement was as an overall limited to the areas receiving the MT treatment. This disagrees with the compressing benefits reported by some authors, who evidenced systemic improvement on contralateral untreated limbs in experimental animal models [
31,
32]. However, when improvement PPT scores (difference between Post and Pre- PPT values: POST-PRE on
Figure 2 and
Supplementary Figure S1), were plotted, we observed patients that were responders (POST-PRE values > 0) and others that appeared as not responders (POST-PRE values < 0), involving all, treated and untreated tender points (
Figure 2 and
Supplementary Figure S1), indicating two different type of patients, and also evidencing the existence of systemic effects.
In reference to the appreciated effects on untreated areas, and its interpretation, we must point that a limitation of this study is the impossibility to attribute the applied mechanical loads to the effects obtained due to the absence of a sham treated arm (group of patients treated with a similar MT protocol using a low <1.4 N pressures) in our design (
Figure 1). This arm was not included in this initial trial since our primary interest was to test the overall benefits and the performance of the output variables before investing any additional efforts. MT treatments inherently contain an emotional component, transferred to the patient through mental relaxation and stress reduction by the sense of touch. In line with this, several are the authors that have demonstrated beneficial health effects obtained from positive emotional stimulus, either reflected by the boosting of the immune system [
34,
35,
58], and effects in weight gain and increased vagal tone [
59], among others. Future interventions should add a sham group to discern mechanical from emotional triggered effects.
Unexpectedly, a negative correlation between patient’s initial hyperalgesia/allodynia status and MT therapeutic benefit was evidenced when the Change Post-Pre values were plotted as a function of their PPT baseline (Pre) values (
Figure 2 and
Supplementary Figure S1). This importantly points out that patient sensitivity to pain, as assessed by its PPTs with an algometer, could serve as an indicator or predictor of the expected patient’s response to MT therapy. In particular, the data indicate that FM patients with worse health status (or at least with highest sensitivity to pain) will obtain most benefits while those presenting closer to normal pain threshold levels will not experiment improvements or will improve to a lesser extent. Among all 18 tender points assayed, we found that the Low cervical, in the treated group, and the Knee within the untreated, constitute the best sensors for this prediction, with prediction values of around 60%, reaching 74% individually (
Figure 2 and
Supplementary Figure S1).
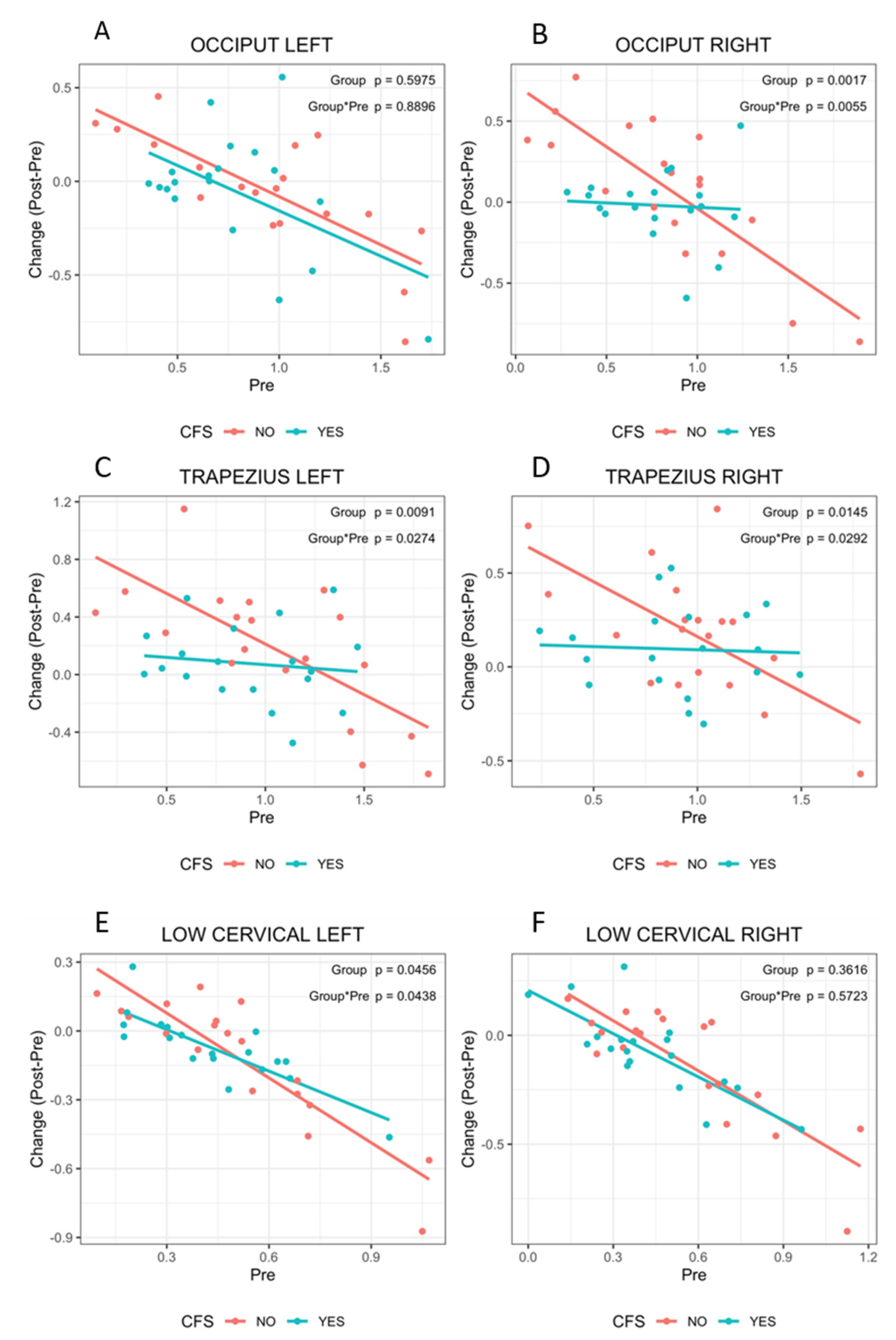
Moreover, we observed that while patients presenting only FM followed PPT improvement patterns inversely correlated with their baseline hyperalgesia/allodynia status, those diagnosed with comorbid ME/CFS did not respond to MT, at least for some of the treated points, as indicated by an overall lack of change in PPT values (
Figure 3E, green lines). This suggests different responses for patients diagnosed with FM only with respect to those presenting comorbid ME/CFS, which is further supported by the obtained CQ scores (
Table 6 and
Table 7).
These observations open the unprecedented possibility of classifying patients as potential “responders” or “not responders” to pressure-controlled MT, based on their thresholds to pain and the presence of comorbid ME/CFS, further supporting somatic and mechanistic differences behind pain perception in one or the other disease. Nevertheless, since the number of observations here is limited, and the current trial is the first to detect these correlations, the findings will need to be validated in additional, more numerous cohorts.
In reference to the studied cohort, it should be stressed that the participating patients were mainly females (35/38), with an average age of 55.6 ± 7.2 years (range 43–71) and time from primary FM diagnosis over 3 years. Most (79%) presented severe affection while 21% corresponded to moderate cases. Physical problems overweighed emotional (
Table 1). In addition, half of them had received diagnosis of ME/CFS. Potential immune and metabolic unbalance associated with low neutrophil percentages (63.8% of the participants), increased monocytes (41.6%), high lymphocytes (16.7%), high cholesterol (72.2%) and low LDL (40%) may be present. Increased levels of creatinine could relate to muscle damage in 22.9% of the participants (
Supplementary Table S2,
n = 36). The possibility that different cohorts of patients lead to distinct outcomes after applying this same protocol remains.
Differences between the participants having been diagnosed with FM only and those receiving diagnosis of both FM and ME/CFS at baseline were identified, mainly with the FIQ items Overall and Symptoms, and with the SF-36 Physical and Vitality items, MFI failed in detecting differences between these two groups. Similarly, FIQ and SF-36 were also superior at detecting differences between the response to MT of either group, with Overall and Total for the first questionnaire and Vitality, Social Functioning and Mental Health in the second. The differences found between groups 30-day after treatment withdrawal could relate to the mentioned observations of distinct response and the fact that the 30-day withdrawal seem not to be enough to washout treatment effects, mostly affecting again to physical roles, as assessed by the SF-36 instrument (
Table 5). Thus, FIQ scores and SF-36 Vitality values may turn into additional indicators of the presence of ME/CFS comorbidity in FM.
Finally, the value of the collection of blood samples gathered and Biobanked in the context of this study results evident, as particular molecular profiles from some of the sets should permit revealing the cellular pathways mediating the response to this pressure controlled-MT protocol, as previously envisioned by our group [
30]. Importantly differential molecular profiles will also allow us to understand the reasons behind patient’s response dependence according to patient’s hypoalgesia/allodynia status and with the co-diagnosis of ME/CFS. It is quite likely that these future studies yield new biomarkers for the prediction of response to MT, some perhaps allowing differential diagnosis of the FM and the ME/CFS disease.

 ,
, 



{kind=link}
{kind=link}
{kind=link}