Prototype Development of an Expert System of Computerized Clinical Guidelines for COVID-19 Diagnosis and Management in Saudi Arabia


Abstract
:1. Introduction
COVID-19 Diagnosis and Management in Saudi Arabia
2. Materials and Methods
2.1. Architecture Overview
2.2. Information Management System
2.3. Expert Systems
2.3.1. Knowledge Acquisition
2.3.2. Knowledge Verification and Validation
2.3.3. Knowledge Representation
2.3.4. Knowledge Engineer
2.3.5. Inference Engine
2.4. Adaptive Learning
2.4.1. Machine Learning
2.4.2. Radiomics Analysis for Chest Images
2.4.3. Revised Knowledge Base
2.5. Notification and Follow-Up System
2.6. Mobile Tracker
2.7. Merging the Sub-Systems
3. Results
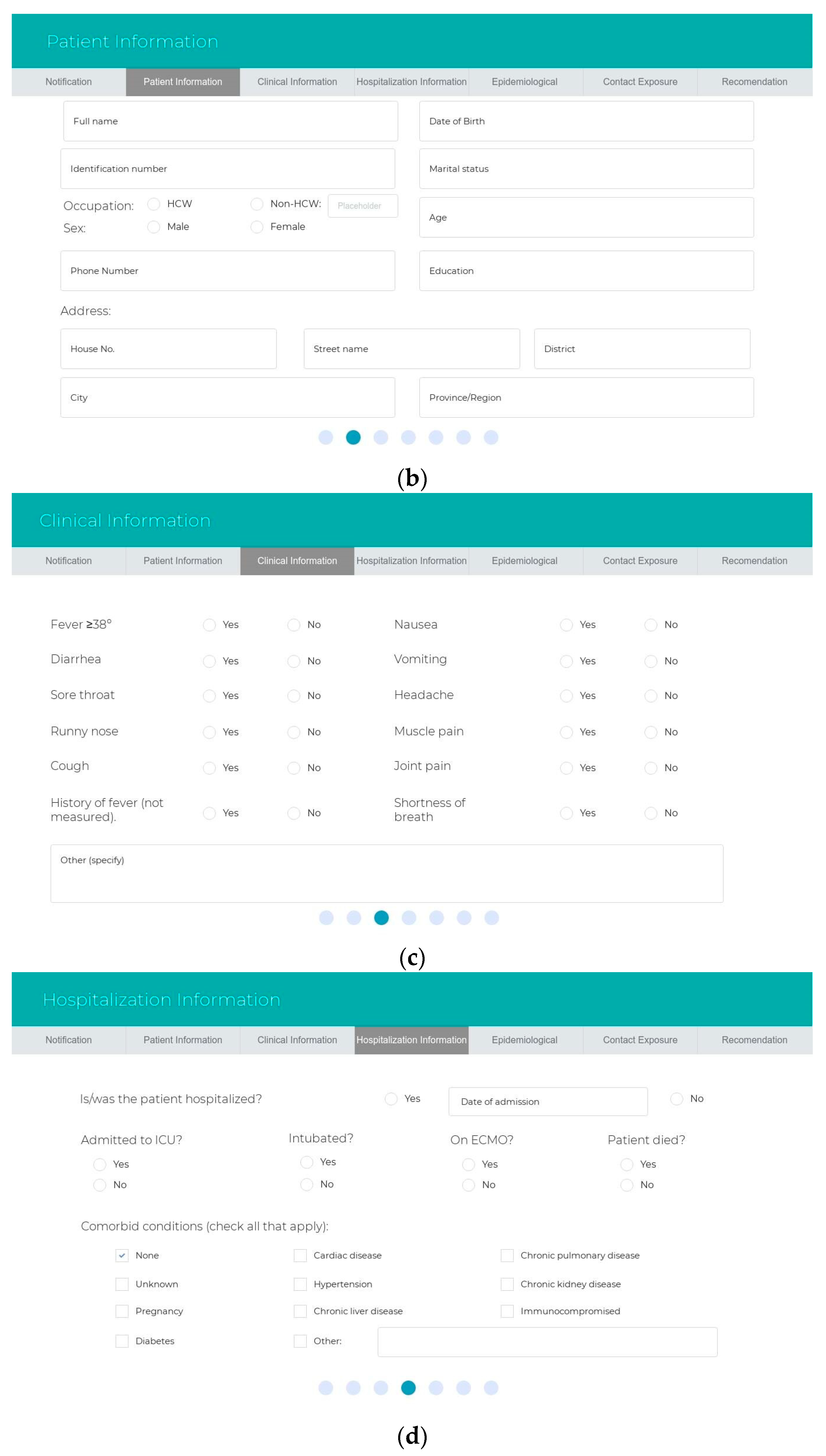
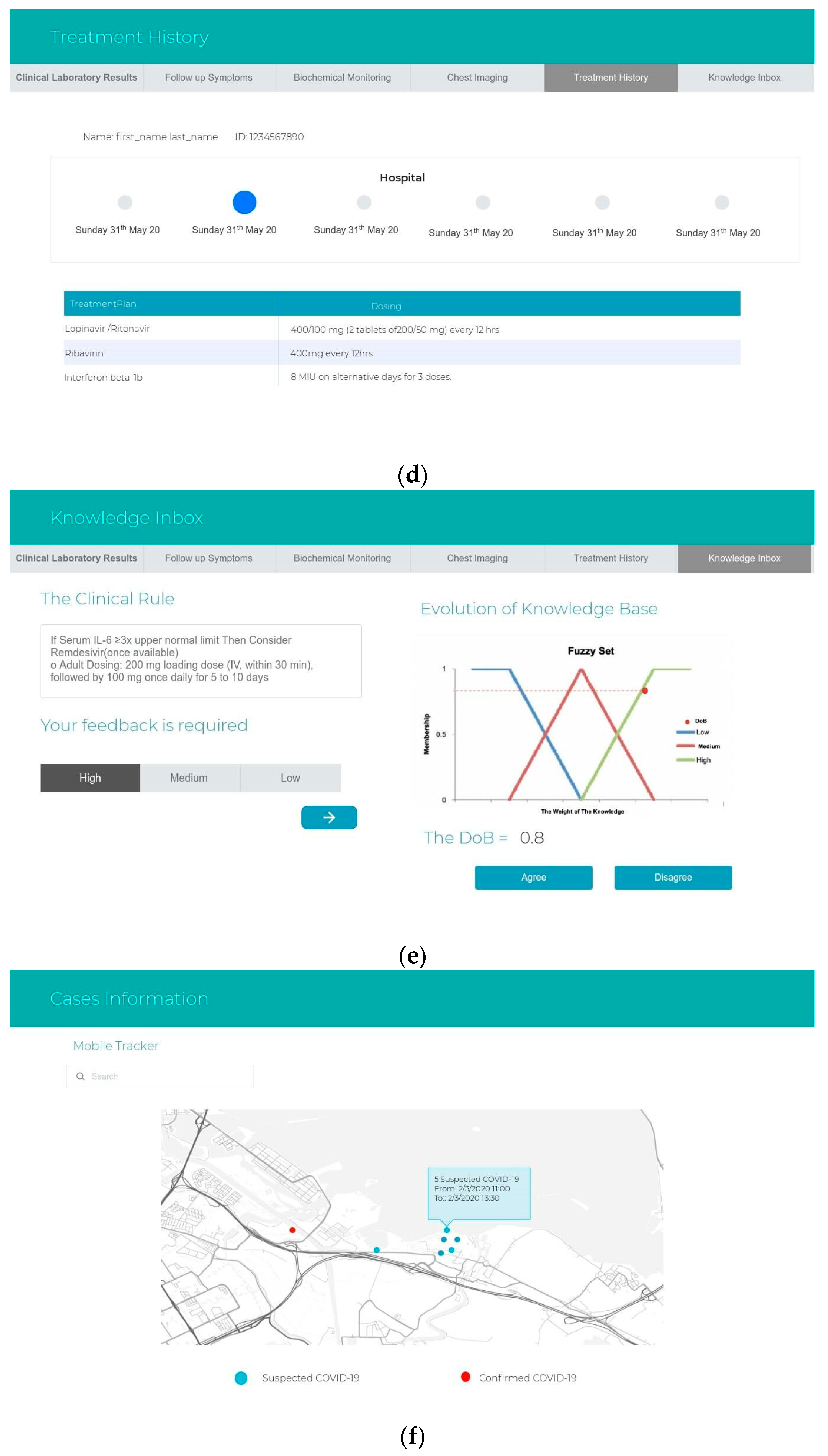
3.1. Prototype of Interface Design
3.2. Task Automation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yang, X.; Sun, R.; Zhao, M.; Chen, E.; Liu, J. Expert recommendations on blood purification treatment protocol for patients with severe COVID-19. Recommendation and consensus. Chronic Dis. Transl. Med. Chin. Med. Assoc. 2020, 6, 1–9. [Google Scholar]
- WHO. Coronavirus Disease (COVID-19) Dashboard. World Health Organization. 2020. Available online: https://covid19.who.int (accessed on 17 May 2020).
- Kondylakis, H.; Tsiknakis, M. Computerized clinical guidelines: Current status & principles for future research. Studies Health Technol. Inform. 2012, 180, 432–436. [Google Scholar]
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Future Health J. 2019, 6, 94–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mujawar, I.; Swami, S.; Shikshan, V. Comprehensive Study on Web Based Expert Systems for Disease. Int. J. Comput. Eng. Appl. 2017, 11, 9. [Google Scholar]
- Culebro, J. Evolution of Expert System. Ph.D. Thesis, Texas Tech University, Lubbock, TX, USA, 1993. [Google Scholar]
- Nguyen, T.T.; Waurn, G.; Campus, P. Artificial Intelligence in the Battle against Coronavirus (COVID-19): A Survey and Future Research Directions. Preprint 2020. [Google Scholar] [CrossRef]
- Medicine, N.; Medicine, N.; Imaging, O.; Iron, W.; Hospital, S.; Hospital, N. Development of a Clinical Decision Support System for Severity Risk Prediction and Triage of COVID-19 Patients at Hospital Admission: An International Multicenter Study. Eur. Respir. J. 2020, 56, 1–24. [Google Scholar]
- Liu, Y.; Wang, Z.; Tian, Y.; Zhou, M.; Zhou, T.; Ye, K. Design and development of COVID-19 risk assessment decision support system for general practitioners Table of Contents. J. Med. Internet Res. 2020. [Google Scholar] [CrossRef]
- Salman, F.M.; Abu-Naser, S.S. Expert System for COVID-19. Diagnosis 2020, 4, 1–13. [Google Scholar]
- Saudi Arabia Government. Saudi Vision 2030. Saudi National Transformation Program; Saudi Arabia Government: Riyadh, Saudi Arabia, 2016; p. 292. [Google Scholar]
- Ministry of Health in Saudi Arabia. Hesn. 2017. Available online: https://hesn.moh.gov.sa (accessed on 19 May 2020).
- Saudi Arabi Ministry of Health. E-Services. 2020. Available online: https://www.moh.gov.sa/en/eServices/Pages/Rest-assured.aspx (accessed on 19 May 2020).
- Ministry of Health in Saudi Arabia. Coronavirus Disease COVID-19 Guidelines; Ministry of Health in Saudi Arabia: Riyadh, Saudi Arabia, 2020; Volume 19, pp. 1–33.
- Tobaiqy, M.; Qashqary, M.; Al-Dahery, S.; Mujallad, A.; Hershan, A.; Kamal, M.; Helmi, N. Therapeutic management of patients with COVID-19: A systematic review. Infect. Prev. Pr. 2020, 2, 100061. [Google Scholar] [CrossRef]
- Saudi MoH Protocol for Adults Patients Suspected of Confirmed with COVID-19. 2020. Available online: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/MOH-therapeutic-protocol-for-COVID-19.pdf (accessed on 26 May 2020).
- Howell, M.D.; Donnino, M.W.; Talmor, D.; Clardy, P.; Ngo, L.; Shapiro, N. Performance of Severity of Illness Scoring Systems in Emergency Department Patients with Infection. Acad. Emerg. Med. 2007, 14, 709–714. [Google Scholar] [CrossRef]
- Deliège, D.A.; Debacker, C.; Smeesters, S.; Knani, H.; Neirynck, I.; De Clercq, E. How to build an information system application to the health domain. Stud. Health Technol. Inform. 2002, 93, 9–17. [Google Scholar]
- Grosan Abraham, C. Rule-based expert systems. In Intelligent Systems; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Shang, Y. 5-Expert Systems; Academic Press: Burlington, UK, 2005; pp. 367–377. [Google Scholar]
- Tso, G.J.; Tu, S.W.; Oshiro, C.; Martins, S.; Ashcraft, M.; Yuen, K.W.; Wang, D.; Robinson, A.; Heidenreich, P.A.; Goldstein, M.K. Automating Guidelines for Clinical Decision Support: Knowledge Engineering and Implementation. AMIA Annu. Symp. Proc. 2016, 2016, 28269916. [Google Scholar]
- Ministry of Health in Saudi Arabia. Coronavirus Disease COVID-19 Guidelines. 2020. Available online: https://www.moh.gov.sa/en/HealthAwareness/EducationalContent/PublicHealth/Pages/corona.aspx (accessed on 20 May 2020).
- Livingston, E.; Bucher, K.; Rekito, A. Coronavirus Disease 2019 and Influenza 2019–2020. JAMA 2020, 323, 1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varming, K.; Forsum, U.; Bruunshuus, I.; Olesen, H. International Federation of Clinical Chemistry and Laboratory Medicine. EJIFCC 2004, 15, 10–13. [Google Scholar] [PubMed]
- Emergency Medicine Cases. A Practical COVID-19 Resource for Emergency Medicine. 2020. Available online: https://emergencymedicinecases.com/covid-19-updates/ (accessed on 21 May 2020).
- Peleg, M. Computer-interpretable clinical guidelines: A methodological review. J. Biomed. Inform. 2013, 46, 744–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Ryzin, J.; Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees. J. Am. Stat. Assoc. 1986, 81, 253. [Google Scholar] [CrossRef]
- Freitas, A.A. Comprehensible classification models: A position paper. ACM SIGKDD Explor. 2013, 15, 1–10. [Google Scholar]
- Tamal, M.; Alshammari, M.; Alabdullah, M.; Hourani, R.; Abu Alola, H.; Hegazi, T.M. An Integrated Framework with Machine Learning and Radiomics for Accurate and Rapid Early Diagnosis of COVID-19 from Chest X-ray. medRxiv 2020. [Google Scholar] [CrossRef]
- Campagna, A.; Pagh, R. Finding associations and computing similarity via biased pair sampling. Knowl. Inf. Syst. 2011, 31, 505–526. [Google Scholar] [CrossRef]
- Zadeh, L. Soft computing and fuzzy logic. IEEE Softw. 1994, 11, 48–56. [Google Scholar] [CrossRef]
- Smith, M.W.; Murphy, D.; Laxmisan, A.; Sittig, D.; Reis, B.; Esquivel, A.; Singh, H. Developing software to “track and catch” missed follow-up of abnormal test results in a complex sociotechnical environment. Appl. Clin. Inform. 2013, 4, 359–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, J.L.; Lo, L.; Ferguson, J.; Goldberg, H.; Diaz-Martinez, J.P.; Tomlinson, G.; Grimshaw, J.M.; Shojania, K.G. Computerised clinical decision support systems and absolute improvements in care: Meta-analysis of controlled clinical trials. BMJ 2020, 370. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Task ID | Tasks | Pre-Automation | Post-Automation |
|---|---|---|---|
| 1 | Health awareness, education, support, and medical advice. | Hotline for health care workers for medical consultations. | Automatically inherited by the knowledge stored in the system. |
| 2 | Designated laboratory tests for confirmed cases. | To be selected after registering on the HESN website. | Recommended laboratory test by the expert system and based on the EHR tracking. |
| 3 | CURB-65 severity score. | Manual. | The score integrated in the expert system. |
| 4 | Visual Triage Checklist. | Risks scores are calculated manually for acute respiratory illnesses and reported using forms. | Integrated into the expert system. |
| 5 | Clinical action to manage the COVID-19 cases in mild, severe, and critical cases. | Manual. | The system automatically classifies patients in his/her risk category and recommends a suitable action and management plan. |
| 6 | List of the individuals who reported their symptoms during health status monitoring under quarantine. | Manually by health workers. | Up-to-date medical history displayed in timeline. |
| 7 | Healthy person to know the safe places to visit. | Not applicable. | Mobile tracker notifies a healthy person of any suspected cases in his/her destination. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banjar, H.R.; Alkhatabi, H.; Alganmi, N.; Almouhana, G.I. Prototype Development of an Expert System of Computerized Clinical Guidelines for COVID-19 Diagnosis and Management in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 8066. https://doi.org/10.3390/ijerph17218066
Banjar HR, Alkhatabi H, Alganmi N, Almouhana GI. Prototype Development of an Expert System of Computerized Clinical Guidelines for COVID-19 Diagnosis and Management in Saudi Arabia. International Journal of Environmental Research and Public Health. 2020; 17(21):8066. https://doi.org/10.3390/ijerph17218066
Chicago/Turabian StyleBanjar, Haneen Reda, Heba Alkhatabi, Nofe Alganmi, and Ghaidaa Ibraheem Almouhana. 2020. "Prototype Development of an Expert System of Computerized Clinical Guidelines for COVID-19 Diagnosis and Management in Saudi Arabia" International Journal of Environmental Research and Public Health 17, no. 21: 8066. https://doi.org/10.3390/ijerph17218066
APA StyleBanjar, H. R., Alkhatabi, H., Alganmi, N., & Almouhana, G. I. (2020). Prototype Development of an Expert System of Computerized Clinical Guidelines for COVID-19 Diagnosis and Management in Saudi Arabia. International Journal of Environmental Research and Public Health, 17(21), 8066. https://doi.org/10.3390/ijerph17218066